Article Text

Abstract
Background and objective Retinal vascular density (VD) measured using optical coherence tomography with angiography (OCTA) has been suggested as a potential marker of intracerebral vascular changes in Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL). We aimed to determine whether VD is related to the clinical and imaging manifestations of the disease.
Methods OCTA was performed in 104 CADASIL patients (parallel to their clinical and imaging assessment) and in 83 healthy individuals.
Results A significant reduction of VD related to age was detected in patients and controls in the superficial and deep vascular plexus of the whole foveal or parafoveal retinal area (p<0.0001). After adjustment for age, these parameters were found significantly lower in patients than in controls (p<0.03). Multivariable analysis did not show any association between retinal VD and history of stroke, modified Rankin Scale or Mini-Mental Status Examination scores. No significant association was found with MRI lesions either .
Conclusion In CADASIL, retinal VD is decreased early and progresses with ageing but does not appear related to the severity of clinical or imaging manifestations.
- Genetics
- Vascular dementia
- CADASIL
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Various abnormalities of retinal vessels have been observed in Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL) patients. Several authors have reported sheathed arteries, tortuous vessels, arteriovenous nicking, arteriolar narrowing or venous enlargement at retinal level.1 2 However, in most reports, these findings were found largely heterogeneous and inconsistent.2
Recently, a decreased density of retinal vessels in the deep retinal plexus was reported using optical coherence tomography with angiography (OCTA) in CADASIL patients and considered as a promising biomarker to follow directly the progression of the vessel disease in-vivo.3 These data were obtained in a small sample and the analysis did not include exact measures of cerebral lesions or consider key factors modulating the disease severity.
In this study, we aimed to determine whether retinal vascular density (VD) measured using OCTA is independently related to the clinical severity and to the main imaging manifestations of CADASIL.
Methods
Patients
A total of 104 patients (53.8±11.9 years; range 27–83; 66 (64%) women) participating in the French Cohort study of CADASIL patients were recruited consecutively for optical coherence tomography angiography (OCTA) assessment from 2019 up to 2021. The diagnosis of the disease was confirmed in all individuals by genetic testing.
Data obtained in parallel from 83 ambulatory individuals (mean age=41.1±15.7 years; range 22–76) consulting for their current eye examinations and visual tests in the ophthalmology department were used as controls. These individuals, who did not have MRI examination, were selected after verifying the absence of vascular risk factor, cardiovascular disease, stroke events or neurological disorder.
Optical coherence tomography with angiography
OCTA examination was performed with the AngioVue-Imaging System (RTVue-XR-Avanti, Optovue); a spectral-domain OCT that enables simultaneous three-dimensional (3D) structural imaging of the retina and generation of en face maps of blood flow through a dedicated algorithm.4
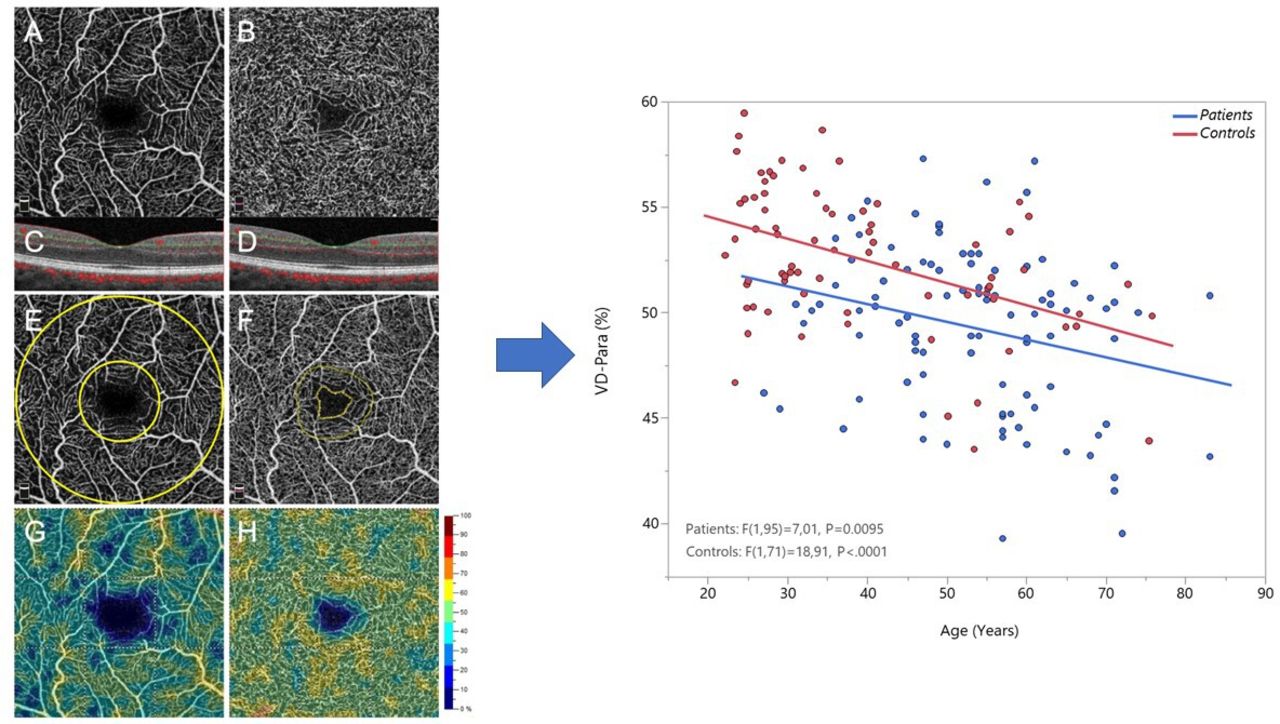
VD was automatically calculated using the phase 7.0 AngioVue analytic software in the superficial vascular plexus and the deep capillary complex as the percentage of the surface occupied by vessels based on adaptive thresholding binarisation (figure 1). Vessel density was measured in the parafoveal area (VD-para) and in the whole area (VD-whole) (details in online supplemental material).
Supplemental material
{kind=link}
Left side: Illustration of OCTA measurement of macular VD on a 3×3 mm angiogram of a CADASIL patient. (A–D): OCT-angiograms and B-scans showing segmentation boundaries (red and green lines) of the superficial vascular plexus (A–C) and the deep capillary complex (B–D); E: inner 1 mm diameter ring centred on the fovea. The parafoveal area is included between the inner ring and outer 3 mm ring. VD whole is calculated in the total area; F: contour of the foveal avascular zone (inner yellow ring); G, H: angiograms with colour-coded VD (H) (colour bar: warmer colours for higher VD). Right side: VD measured in patients and controls in the deep parafoveal vascular plexus according to age. OCT, optical coherence tomography; OCTA, optical coherence tomography with angiography; VD, vascular density.
Clinical and imaging parameters
OCTA examination was performed in each patient at the time of follow-up visits. The details of the work-up obtained at each visit have been previously reported.5 6 Particularly, the presence of any vascular risk factor was systematically recorded. Disability was scored using the modified Rankin Scale (mRS) and cognitive status using the Mini-Mental State Examination (MMSE).
MRI data were obtained using a 3-Tesla imaging system. All lesions (white matter hyperintensities (WMH), lacunes, microbleeds, brain volume) were assessed as previously detailed.6 Briefly, the volume of WMH was segmented using the Brain Intensity AbNormality Classification Algorithm (BIANCA) method and normalised to the volume of the intracranial cavity as well as the brain volume (providing the brain parenchymal fraction (BPF)). Two experts assessed visually the 3DT1-weighted and susceptibility-weighted images to obtain the total number of lacunes and of microbleeds.
Analysis
Data obtained in patients and controls were compared after adjustment for age and sex. Association between clinical or imaging parameters and each retinal vascular parameter was assessed by multivariable analyses using generalised linear models and adjustment for age, presence of hypertension (HT), presence of other vascular risk factors, location of mutation in EGFR domains of the Notch3 protein, from 1 to 6 vs 7 to 34, which has been shown to influence the severity of the CADASIL phenotype.7 8
Results
In the CADASIL sample, 58 (56%) patients had a cysteine mutation within the epidermal growth factor receptor (EGFR) domains from 1 to 6, 25 (24%) had a history of HT, 68 (66%) had other vascular risk factors. At the time of the study, 54 (52%) individuals already had a stroke, 35% had an mRS higher than 1, the MMSE score was less than 24 in 11 patients (10%). The mean systolic blood pressure was 125±17 and diastolic blood pressure 79±9.5 mm Hg. The mean volume of WMH was 167767 ± 68173 mm3, the median value and IQR were 2 and 0–7 for the number of lacunes, 0 and 0–3 for the number of microbleeds. The mean BPF was 80.16% ±3.8%.
Mean values of VD-para, VD-whole at superficial and deep retinal levels measured in patients, and controls are detailed in table 1. A significant reduction of VD in the parafoveal area or in the whole foveal area was observed with age for both the superficial and deep vascular plexus (p<0.0001). After adjustment for age, VD-para and VD-whole were found significantly lower in patients than in controls both in the superficial and deep vascular retinal plexus. No significant effect of sex on these parameters was detected (figure 1).
Results of multivariable analysis showing the significant age and group effect (between patients and controls) as well the mean and least square (LS or adjusted) mean values obtained for each retinal vascular parameter in the two groups
Multivariable analysis did not show any association between VD measured in parafoveal retinal areas in both the superficial and deep vascular plexus and each of the following clinical parameters: past occurrence of stroke, mRS and MMSE scores (online supplemental table). There was also no significant association at cerebral MRI level with the number of lacunes, that of microbleeds, the normalised WMH and brain volumes (online supplemental table). In contrast, a strong age-related decrease of VD was measured in the deep and superficial plexus. The results were exactly similar when the analysis was performed using VD-whole (data not shown).
Discussion
Our results show that there is a significant reduction of retinal vessel density in a large cohort of CADASIL patients in comparison to non-hypertensive and non-diabetic controls. Our findings confirm the significant decrease of the retinal vascular network density using OCTA previously detected in 11 CADASIL patients compared with 21 age-matched controls3 and are in line with the fractal dimension changes of the retinal vascular network already detected in another sample.9 They also further emphasise the strong reduction of retinal VD recently reported with normal ageing.10 In this study, this reduction is observed both in the superficial and deep vascular plexus and seems to evolve in the same way as with normal ageing, in patients and in healthy individuals. After age adjustment, a 2%–4% reduction of retinal VD is measured in patients (see table 1). Our data suggest that this difference might occur since the early stage of the disease.
The lack of correlation with the clinical and imaging features of the disease contradicts some initial results in the literature using the same technology.11 Retinal VD was previously found lower in stroke than in non-stroke CADASIL patients and correlations have been highlighted with gait speed and the number of lacunes.12 These discrepancies might be related to the different age, ethnic origin, prevalence of HT or mutation location in the previous studies. We think however that our findings are reliable for multiple reasons. First, the size of our sample is at least two times larger than in all previous studies. Our clinical scales are currently used to assess clinical severity in this disorder.6 Both quantified and validated measures of cerebral lesions were obtained in contrast with most previous reports. Finally, the analysis was performed separately for each clinical or imaging marker with taking into account key modifiers of the disease phenotypic variability such as age, sex, HT, vascular risk factors and the location of NOTCH3 gene mutation. Due to the cross-sectional nature of the study, however, one limitation is that, we cannot exclude small changes that may also occur during the course of the disease.
These results are important because they show that significant changes in the vascular network within extracerebral tissues such as those detected in the retina do not necessarily have clinical or pathogenic correlates at cross-sectional level in CADASIL. Although the retinal VD may be reduced at the outset in such condition, we think that our results indicate that this alteration should not be necessarily considered as a mirror of the cerebrovascular alterations leading to tissue lesions and subsequently to disability and dementia in CADASIL. Other retinal vessel structural or functional markers should be investigated to link cerebral lesions to retinal vessel changes in this disorder.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Institutional Review Board of INSERM (IRB00003888, IORG0003254, FWA00005831) Advice number 17-388. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We warmly thank the team in charge of formatting and cleaning the database Mrs Claire Pacheco under the direction of Pr S Chevret (INSERM UMR1153). We thank very much the team in charge of the neuropsychological assessments particularly Mrs Sonia Reyes, Aude Jabouley, Carla Machado, Helene De Sanctis; Mrs Solange Hello and Celine Martin who managed and organised the appointment of multiple family members involved in the study, Mrs Nathalie Gastelier and Fanny Fernandes, the research managers in charge of the Cohort Study. We thank also the CADASIL France Association for their help and permanent support.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors VK: acquisition, analysis, writing. MP: analysis, writing. DH: clinical evaluation, inclusion, writing. CD: retinal data analysis. AT: organisation, data verification, database management. NG: authorisation, logistics, organisation. EJ: cerebral imaging data analysis. JL: cerebral imaging data analysis. RT: supervision of ophtalmological research and writing. HC: funcing, cohort follow-up, data analysis, writing.
Funding This work was funded by the RHU TRT_cSVD project (France 2030 - ANR-16-RHUS-004) and the ARNEVA (Association de Recherche en Neurologie VAsculaire), Hopital Lariboisiere, France.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.