Article Text

Abstract
Background Chronic migraine is a disabling condition, often associated with comorbidities including cognitive dysfunction, anxiety and depression. It is unclear whether cognitive complaints are associated with the underlying migraine pathophysiological process or related to drugs or comorbidities of depression and anxiety.
Objective To evaluate cognitive changes in chronic migraine and assess reversibility of cognitive dysfunction following effective migraine treatment using onabotulinumtoxinA.
Methods This was a prospective real-world study of 60 patients with chronic migraine treated with onabotulinumtoxinA. Headache diaries recorded total headache days at baseline and duration of 12 weeks post-treatment. Computerised cognitive tests of reaction time and working memory (WM) speed and accuracy using a purpose-specific website was implemented at baseline, 6 weeks and 12 weeks. The Patient Health Questionnaire (PHQ-9) and Penn State Worry Questionnaire-Past Week (PSWQ-PW) were administered for depression and anxiety levels. Associations between clinical response, cognitive parameters, PHQ-9 and PSWQ-PW were analysed.
Results At 6 weeks post-treatment, 88% patients achieved good response (≥50% reduction in headache frequency) with improvement of PHQ-9, PSWQ-PW, cognitive speed tests and WM accuracy compared with baseline (all p<0.05). There was no overall correlation between good headache response and improved cognitive measures and no association between good headache response and improved PHQ-9 and PSWQ-PW scores. Improved WM accuracy correlated with reduced PSWQ-PW (p=0.047). There was no correlation between improved WM accuracy and reduced PHQ-9.
Conclusions OnabotulinumtoxinA treatment for chronic migraine improved anxiety, depression and cognitive performances but these improvements did not correlate with reduction in headache and migraine frequency. Improved WM accuracy was significantly associated with reduced anxiety level.
- migraine
- memory
- cognition
- neuropsychology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Chronic migraine is a common and disabling condition with a population prevalence of about 2%.1 Compared with patients with episodic migraines, those with chronic migraines have poorer health-related quality of life, increased headache related disability, particularly involving employment, social and family functioning, as well as greater psychiatric and medical comorbidities.2 3 Chronic migraine patients often report cognitive complaints such as poor memory and difficulty with mental tasks. Although several studies have investigated cognitive function in heterogeneous cohorts of migraine patients, the findings lack general consensus.4–12 These studies, which involve diverse subsets of migraineurs, suggest migraine patients in general have lower cognitive performance than controls, especially in neuropsychological domains such as visual and verbal memory, information processing speed, attention and executive functions. Systematic studies of cognitive dysfunction in patients with chronic migraine are lacking and it is unclear as to whether cognitive complaints are associated with the underlying migraine pathophysiological process or related to effects of drugs or comorbidities such as mood disorders. Although studies have shown that depression and anxiety are common comorbidities of migraine,13–17 it is unclear how these mood disorders relate to cognitive dysfunction.
Currently, onabotulinumtoxinA treatment is one of the most successful management approaches for chronic migraine.18–23 Three recent studies found that prophylactic onabotulinumtoxinA treatment for chronic migraine was associated with statistically significant improvements in depression and anxiety symptoms16–18 and that this improvement in comorbid depression and anxiety may be independent of the reduction in headache frequency. However, there are no previous studies on the effects of onabotulinumtoxinA on cognitive function in patients with chronic migraine.
One of the objectives of our study was to investigate the relationship between cognitive disability in chronic migraine and the comorbidities of depression and anxiety. We hypothesise that patients with chronic migraine have a risk of cognitive impairment and that if the neurocognitive disability is a direct consequence of increased headache frequency, following effective treatment, using onabotulinumtoxinA, there will be a positive correlation between good headache response and improved neurocognitive parameters. We designed our study enrolling a homogenous group of patients who met the ICHD-3 (International Classification of Headache Disorders - 3rd edition, 2018) definition of chronic migraine24 and we attempted to control for confounding effects of pain and drugs on cognitive testing by administering the cognitive tests during the interictal headache-free state. We controlled for the impact of maintenance medications such as topiramate, by testing for intra-subject change in cognitive performance. Although the primary efficacy measure in this study was change from baseline in headache days at 6 weeks and 12 weeks post-onabotulinumtoxinA treatment, our exploratory outcome measures were changes in cognitive performance, Patient Health Questionnaire (PHQ-9) and Penn State Worry Questionnaire-Past Week (PSWQ-PW) scores post-treatment.
Methods
This was a prospective real-world evidence study of 60 patients with chronic migraine who attended a General Neurology Clinic in Perth, Western Australia between July 2017 and February 2019 who were eligible for Pharmaceutical Benefits Scheme (PBS)-subsidised onabotulinumtoxinA treatment. We investigated comorbidities of cognitive and mood changes at baseline and at 6 weeks and 12 weeks following treatment. Patients gave informed consent.
In Australia, to be eligible for PBS-subsidised onabotulinumtoxinA treatment for the prophylaxis of chronic migraine, patients need to be aged 18 years or older, under the care of a neurologist and had experienced an average of 15 or more headache days per month, with at least eight migraine days per month over a period of 6 months or longer. PBS eligibility also required poor efficacy and/or intolerability of at least three preventive migraine medications. We excluded patients with medication overuse headaches (MOH) from the study. To control for medication effect during intra-subject testing, patients continued all their existing regular medications including other concurrent oral migraine preventive medications and antidepressants, with doses of these medications remaining stable during the entire 12 weeks of the study. Using a headache diary, patients recorded headache days (defined as a 24-hours period in which a headache of mild to moderate intensity lasted at least 1 hour) and migraine days (defined as high intensity, lateralised pain with a significant impairment on daily activities) and the number of days on which they used symptomatic medication, particularly triptans. A computerised cognitive test was performed at baseline (prior to onabotulinumtoxinA treatment) and at 6 weeks and 12 weeks post-treatment. Patients were asked to perform all cognitive tests during the inter-ictal state with no headache symptoms for at least 24 hours before testing. Patients were instructed to refrain from alcoholic beverages or over-the-counter medications for at least 48 hours before cognitive testing and not to consume caffeinated beverages at least 24 hours before testing.
The computerised cognitive test used a purpose-specific website made available by UBrain (www.ubrain.com.br). The validation of this methodology has been previously published in the context of cognitive screening in multiple sclerosis.25 Our study platform tested patients’ information processing speed, attention, working memory (WM) and episodic memory using a self-paced computerised system. The test consisted of three different tasks, using a set of universal, very simple stimuli presented in a visual game-like interface. Participants were asked to perform at least one practice test prior to each clinic-based test. This allowed for familiarisation of the system while limiting practice effects. The cognitive testing included the following: the first task, testing psychomotor (processing) speed (Simple Reaction Test (SRT)), required participants to press the ‘YES’ button as soon as a soccer ball appeared on the screen. The second task, testing visual attention (Choice Reaction Test (CRT)), required participants to press the ‘YES’ button if the soccer ball appearing was red, otherwise to press the ‘NO’ button. The third task (Learning Test) required participants to press ‘YES’ or ‘NO’ button if the card displayed had been seen before in the testing session. The final task, testing WM (One Back Test), required participants to press the ‘YES’ or ‘NO’ button if the card displayed was the same as the immediately previous card. The cards presented consisted of a combination of four colours, four shapes and eight numbers, allowing for 128 unique possibilities in stimuli. All tasks had a prestimulus interval of 1000 ms and a 100–5000 stimulus interval between 0–1000 ms. The cards were presented using random order, timing and correct response, allowing a very large number of equivalent alternate forms of the tasks to be generated. The speed tests were measured in milliseconds and the accuracy tests were expressed as percentage of correct responses. The total cognitive test battery duration was 10–15 min. Patients were asked to rate their cognitive performance using a subjective scale at baseline and at 6 weeks post-onabotulinumtoxinA treatment, where 1=much worse than normal, 2=worse than normal, 3=normal, 4=better than normal and 5=much better than normal.
Prior to the onabotulinumtoxinA treatment (baseline) and at 6-weeks follow-up, questionnaires assessing anxiety and depression status were also administered. Participants rated their level of anxiety (using a simple 10 points Likert-type scale from ‘None’ to ‘Very anxious’). PSWQ-PW26 assessed anxiety during the past week using subjective ratings for 15 simple statements (maximum score 90). PHQ-927 assessed mood using a subjective rating of nine short statements covering mood and somatic symptoms of depression over the past 2 weeks (maximum score 27, mild depression ≥5).
All patients received onabotulinumtoxinA injections at baseline in accordance with the Phase 3 REsearch Evaluating Migraine Prophylaxis Therapy (PREEMPT) 2 protocol.28 29 Study injections were administered by the principal investigator (SH) using a 31 fixed-site, fixed dose, intramuscular injection protocol (minimum total dose of 155U) across seven specific head/neck muscle areas and ‘follow the pain’ strategy with additional dosing at the investigator’s discretion (maximum dose 195U).
Outcome measures
The primary efficacy measure in this study was change from baseline in total headache days per month at 6 weeks and 12 weeks as assessed by patients’ daily diaries. Change from baseline in migraine days per month at 6 weeks and 12 weeks was also assessed. A subgroup analysis was performed in patients who experienced ≥75%, ≥50%, or ≤25% reductions in headache and/or migraine days. Clinical response was classified as excellent (≥75% reduction in headache and/or migraine days), good (≥50% reduction in headache and/or migraine days) or poor (≤25% reduction in headache and/or migraine days). Exploratory outcome measures included change from baseline in cognitive parameters including SRT, CRT and WM speed and SRT, CRT, WM accuracy at 6 weeks and 12 weeks as well as change from baseline in PHQ-9 and PSWQ-PW (depression and anxiety) scores at 6 weeks.
Statistical analysis
Changes from baseline in frequencies of total headache days and migraine days were analysed as mean changes from baseline using 1-tailed paired t-test. Data was presented as means and SD for continuous data or medians and IQRs when data was skewed. To account for missing data, we used linear mixed models for repeated measures to compare within group differences for the PHQ9, PSWQ-PW and speed variables, with mean differences and their 95% CIs produced. Unlike other statistical methods, linear mixed models have the ability to give unbiased results in the presence of missing data, without the need for listwise deletion and therefore not compromising both power and bias of the study. For accuracy variables, changes in scores between each time point were calculated with median difference and their corresponding 95% CIs produced with statistical significance determined using the non-parametric Wilcoxon signed rank test. For mean or median difference, a negative value would indicate a reduced score from the first to second time point. For speed variables, a reduced score would indicate improvement, whereas for accuracy scores, an increase would indicate an improvement. The association between clinical response scores and baseline accuracy, speed, PHQ-9 and PSWQ-PW was investigated using Analysis of Variance (ANOVA) and box plots. The association between questionnaires (PHQ-9 and PSWQ-PW) was tested using Pearson’s correlation coefficients and scatter plots. Paired t-tests were analysed using Excel and all other data analysed using Strata V.14.1. Statistical significance was considered p<0.05.
Results
Patient demographics and disposition
A total of 60 patients fulfilling the chronic migraine criteria were enrolled in the study. All patients completed the headache diaries for the entire study duration of 12 weeks. Two patients had missing PHQ-9 and PSWQ-PW results due to computer technical difficulties. Three patients completed the 6-weeks follow-up cognitive assessment but did not complete the 12-weeks follow-up cognitive assessment due to scheduling difficulties.
The study population had a mean (SD) age of 46.7 (12.4) years and were predominantly female (n=54, 90%) and Caucasian (n=55, 91.7%). At baseline, the mean (SD) total number of headache days per month was 24.6 (5.6), of which the mean (SD) number of severe migraine days per month was 13 (4.7). At baseline, 48 patients (82.8%) had mild or worse depression status (PHQ-9 ≥5) with a mean (SD) PHQ-9 of 9.85 (6.17) indicating mild to moderate depressive symptoms. At baseline, 29 patients (50%) had at least moderate anxiety symptoms (PSWQ-PW ≥44) with a mean PSWQ-PW score of 45.8 (15.08) indicating moderate anxiety level. Concomitant regular medications, which included other migraine prophylactic agents taken by the patients are summarised in table 1. These medications were continued with dose remaining stable, during the 12 weeks duration of the study. Symptomatic ‘pain killer’ medications taken by patients on an as needed basis for acute migraine attacks are also summarised in table 1. Patients refrained from taking these medications for 48 hours before the cognitive testing.
Patient medication profile
Treatment efficacy outcome
Fifty-three patients (88%) achieved a 50% or greater reduction from baseline in total headache days per month at 6 weeks and at 12 weeks post-onabotulinumtoxinA treatment. There was a statistically significant reduction in mean (SD) total headache days at 6 weeks compared with baseline (8.6 (7.8) days vs 24.6 (5.6) days, p<0.0001). There was also a statistically significant reduction in mean (SD) total headache days at 12 weeks compared with baseline (10.6 (7.1) days vs 24.6 (5.6) days, p<0.0001). There was a statistically significant increase in mean (SD) total headache days at 12 weeks compared with 6 weeks (8.6 (7.8) days vs 10.6 (7.1) days, p=0.00043), most likely reflecting medication wearing off effect towards the end of the onabotulinumtoxinA injection cycle. Similarly, there was a statistically significant reduction in mean (SD) migraine days at 6 weeks compared with baseline (2.3 (2.9) days vs 13.0 (4.7) days, p<0.0001) and at 12 weeks compared with baseline (3.7 (3.4) days vs 13.0 (4.7) days, p<0.0001), (table 2). We found that patients’ subjective report of excellent improvement concurred more with reduction in migraine days than reduction in total headache days. One patient with less than 25% reduction of total headache days considered her treatment a success as she had (≥50% reduction in migraine days) and thus she was considered in the good responder category. Overall, clinical response was considered excellent in 19 patients (31.7%), good in 35 patients (58.3%) and poor in 6 patients (10%).
Treatment efficacy outcome measures at baseline, 6 weeks and 12 weeks
Exploratory outcome measures
At 6 weeks post-onabotulinumtoxinA treatment, there was statistically significant improvement of mean (SD) PHQ-9 scores compared with baseline (6.72 (4.57) vs 9.85 (6.17), p<0.001), indicating lower depression levels (table 3). There was statistically significant improvement of mean (SD) PSWQ-PW scores compared with baseline (40.24 (16.23) vs 45.80 (15.08), p<0.001), indicating lower anxiety levels.
Mood measures: changes in PHQ-9 and PSWQ-PW scores
Results of cognitive outcome measures are shown in table 4. From baseline to 6 weeks, improved scores were demonstrated for all speed outcome variables, with reduction in time across all three outcomes (p<0.05). From baseline to 12 weeks, all speed outcomes demonstrated improved score, with reduction in time across all three outcomes (p<0.05). There was no statistical change from 6 weeks to 12 weeks for the speed outcomes. WM accuracy was the only accuracy score to show an improvement with a median increase of 3.0 from baseline to 6 weeks (p<0.001). There was no statistically significant improvement in WM accuracy from baseline to 12 weeks.
Cognitive measures: speed and accuracy outcomes for each time point
At baseline, mean (SD) subjective cognitive performance score was 2.81 (0.52) denoting ‘worse than normal’ cognitive performance. At 6 weeks, mean (SD) subjective cognitive performance score was 3.31 (0.77), denoting ‘normal’ cognitive performance (p<0.001).
Correlation between outcome measures
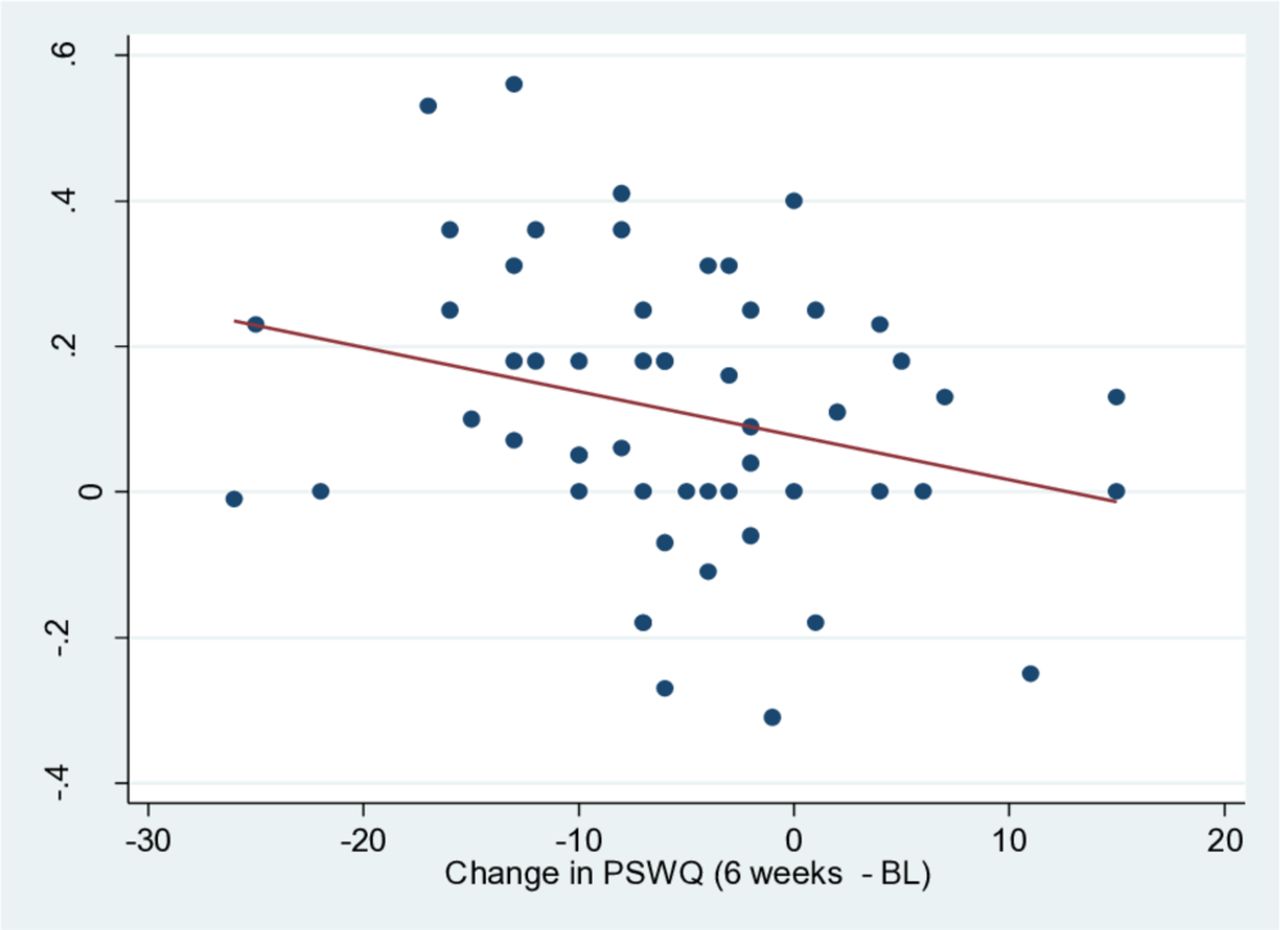
There was no statistically significant association between good headache response and improved cognitive measures (table 5). There was no statistically significant association between good headache response and change in PHQ-9 and PSWQ-PW scores (all p>0.05) (table 5). Improvement in WM accuracy at 6 weeks post-treatment correlated with reduced PSWQ-PW scores (lower anxiety levels, p=0.047) (table 6 and figure 1). However, there was no correlation between improvement in WM accuracy and reduced PHQ-9 (depression) scale at 6 weeks post-onabotulinumtoxinA treatment (table 6). Improvement in speed measures (SRT, CRT, WM accuracy) at 6 weeks post-treatment was not associated with improved PSWQ-PW and PHQ-9 scores at 6 weeks (table 5). However, baseline PHQ-9 and SRT scores were positively correlated (higher severity of depression associated with slower speed), which was not an unexpected finding.
Clinical response and associations
Correlation of change in PHQ-9, PSWQ-PW scores and change in speed, accuracy
{kind=link}
Association of change in working memory (WM) accuracy and change in PSWQ. Y-axis represents change in WM accuracy scores between 6 weeks and baseline (BL). There is an association suggested with change in PSWQ-PW score and WM score. With an improvement in WM accuracy there is greater reduction in PSWQ-PW score. With PSWQ-PW change where patient scores indicate greater anxiety level from BL to 6 weeks, there is reduction in accuracy score. PSWQ-PW, Penn State Worry Questionnaire-Past Week.
Safety
No serious adverse events were reported at any time during the study. Mild adverse events considered most probably related to the onabotulinumtoxinA occurred in five patients (8.5%) and included injection site bruising (2), cervical muscle pain (2) and mild partial ptosis (1).
Discussion
In this prospective real-world evidence study, onabotulinumtoxinA treatment of patients with chronic migraine was associated with statistically significant reductions, from baseline to weeks 6 and 12, in number of total headache days and number of migraine days. In addition, there were statistically significant improvements, from baseline to week 6, in depression symptoms (PHQ-9), anxiety symptoms (PSWQ-PW) and cognitive measures of speed and accuracy.
The phase 3 PREEMPT trials demonstrated that onabotulinumtoxinA significantly reduced the frequency of headaches and migraine days compared with placebo.30–32 Our findings concurred with those from many observational studies that have confirmed the safety and efficacy of onabotulinumtoxinA for the prevention of chronic migraine.16 18–23 The proportion of patients achieving a ‘good response’ (defined as ≥50% reduction in headache days per month) in our study was 88%, which was notably higher than the ‘good response’ rate reported in other real-world evidence studies (74% reported by Stark et al,23 46% for headache reduction and 74% for migraine reduction reported by Kalil et al 19 and 39.5% at week 24% and 61.1% at week 108 reported by the COMPEL study.18 Possible explanation for the higher ‘good response’ rate in our study may be explained by the exclusion of all patients with MOH from our study in contrast to the other studies, which included patients with MOH. Furthermore, unlike the other studies, which implemented a fixed-site, fixed dose injection paradigm that did not allow for >155U onabotulinumtoxinA, we included a ‘follow the pain’ strategy with additional dosing at the investigator’s discretion (maximum dose 195U). Superior efficacy of the 195U ‘follow the pain’ strategy has been previously demonstrated.33 Negro et al 33 showed that the higher dose was more effective than the standard 155U in terms of mean reduction in headache days, migraine days, pain medication intake days and Headache Impact Test (HIT-6) score and that the 195U superior efficacy in all considered measures was evident since the first injection and was maintained over 2 years. Placebo effect may also be a contributing factor in our study.
Depression and anxiety are common comorbidities of chronic migraine and recent studies have found that onabotulinumtoxinA treatment was associated with statistically significant reduction in depression and anxiety scores.16–18 Our study also demonstrated statistically significant reduction in depression and anxiety scores in addition to reduction in headache day frequency at 6 weeks following onabotulinumtoxinA treatment. The definitions of anxiety and depression in our study was based on the self-reported PSWQ-PW and PHQ-9 questionnaires, which have been previously validated26 27 and were used because of their ease of administration. Our study showed that there was no association between clinical response (reduction in headache frequency) and reduction in PSWQ-PW score (anxiety level) and no association between clinical response and reduction in PHQ-9 score (depression level) (table 4). We did not analyse if the improvement in PSWQ-PW and PHQ-9 scores were clinically relevant changes but previously, Blumenfeld et al,16 have found that onabotulinumtoxinA treatment was associated with a clinically relevant change in anxiety and depression symptoms regardless of whether patients had a reduction in headache days.
We believe our utilisation of a computerised cognitive test via a purpose-specific website for assessment of cognitive changes in patients with chronic migraine is novel. We found a statistically significant improvement in cognitive speed measures (SRT, CRT, WM speed) and WM accuracy at 6 weeks compared with baseline (all p<0.05). There was no correlation between good headache response and improved cognitive measures and no association between good headache response and improved PHQ-9 and PHWQ-PW scores. However, improved WM accuracy correlated with reduced PSWQ-PW (lower anxiety level) (p=0.047).
Our study has limitations in that we do not have a control group for the cognitive testing. However, the study was designed to test for changes between two time points rather than actual numbers. We believe the overall significant improvement in speed measures at 6 weeks and 12 weeks are unlikely to be explained by practice effect. Although the lack of association with clinical response could imply practice effect, this is more likely to be due to something else such as lack of statistical power in our study design, onabotulinumtoxinA having an independent effect on cognitive measures or an independent pathophysiological process. Arguments against practice effect include the following: first, subjects did a practice test before the first (baseline) scored test and a recent study25 has demonstrated excellent test–retest reliability following the second administration using a computerised battery employing a similar testing paradigm. Second, table 4 showed WM accuracy improved from baseline to 6 weeks (median difference (95% CI) 3.0 (0.00, 6.0), p<0.001) but not changed from baseline to 12 weeks (median difference (95% CI) 0.00 (0.00, 3.0), p=0.058). If practice effect was the case, there should also be an improvement from baseline to 12 weeks. On the contrary, there was a reduction in WM accuracy scores from 6 weeks to 12 weeks (median difference (95% CI) 0.00 (−3.0, 0.00), p=0.005), which can be better explained by onabotulinumtoxinA wearing off towards the end of the treatment cycle. Our study also showed a statistically significant increase in mean (SD) total headache days at 12 weeks compared with 6 weeks (8.6 (7.8) days vs 10.6 (7.1) days, p=0.00043), which also supports medication wearing-off effect. Our study did not demonstrate correlation between better headache or migraine control and improvement in depression, anxiety or cognitive performances even though these aspects were improved in the group overall. Although this may raise the possibility that onabotulinumtoxinA has an independent effect on these outcomes, it is also possible that the study was simply not powered to demonstrate a link between headache response and these other parameters.
Further studies are needed to investigate the relationship between cognitive and mood changes in patients with chronic migraine. The recent study by Blumenfeld e t al 16 also showed that onabotulinumtoxinA was associated with improvement in sleep quality and fatigue in patients with chronic migraine. It is still unclear if these other comorbidities indirectly contribute to cognitive dysfunction in chronic migraine or if the underlying migraine pathophysiological process directly affects cognition. Neurophysiological and functional imaging studies suggest that brain networks are altered before the onset of migraine headache.34 For example, Positron Emission Tomograph (PET) studies have indicated anterior cingulate cortex activation mediating mood and cognitive changes in patients with chronic migraine. Future studies with functional neuroimaging to investigate mood and cognitive changes in the prodromal state of migraine may provide further insights.
Conclusion
Our study demonstrated that onabotulinumtoxinA treatment for chronic migraine improved anxiety, depression and cognitive measures in addition to improvement in headache and migraine control. However, direct correlation between reduction in headache and migraine frequency and improvement in mood and cognitive outcomes could not be demonstrated. Improved WM accuracy was significantly associated with reduced anxiety level. Further studies are needed to investigate the complex relationship between mood, cognition and other comorbidities in patients with chronic migraine. From a clinical perspective, it is reassuring to patients with chronic migraine that their mood and cognitive symptoms can be improved following onabotulinumtoxinA treatment and this is in addition to reduction in headache and migraine frequency.
References
Footnotes
Contributors SH contributed to study design, recruited patients, administered onabotulinumtoxinA injections, collected data, analysed and interpreted results, performed statistical analysis with Excel and drafted the manuscript. DD contributed to study design, adapted cognitive testing website software for the purpose of this study, contributed to data analysis and contributed to drafting manuscript. NB performed statistical analysis using Stata V.14.1.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the St John of God Health Care Human Research Ethics Committee. Ref No/ ID: 1151.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Data will be made available to anyone who wishes to access data beginning 9 months and ending 36 months following article publication.