Article Text

Abstract
The COVID-19 pandemic has reshaped the way healthcare systems operate around the world. The major hurdles faced have been availability of personal protective equipment, intensive care unit beds, ventilators, treatments and medical personnel. Detroit, Michigan has been an epidemic ‘hotspot’ in the USA with Wayne County among the hardest hit counties in the nation. The Department of Neurology at Henry Ford Hospital, in the heart of Detroit, has responded effectively to the pandemic by altering many aspects of its operations. The rapid engagement of the department and enhanced utilisation of teleneurology were two of the pivotal elements in the successful response to the pandemic. In this review, we describe the transformation our department has undergone, as it relates to its infrastructure redesigning, coverage restructuring, redeployment strategies, medical education adaptations and novel research initiatives.
- health policy & practice
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/ .
Statistics from Altmetric.com
Introduction
Initially, the first confirmed cases of COVID-19 in Michigan were recorded on 12 March 2020. On 9 April 2020, the State of Michigan revised their data and reported that 56 people were found to be COVID-19 positive on 1 March 2020. Detroit rapidly became one of the country’s ‘hotspots’ with Wayne County making the top five most affected counties in the USA. At the time of writing, the tri-county area (Wayne, Oakland and Macomb) made up 5% of the country’s COVID-19-related death toll. Henry Ford Health System (HFHS), through its six hospitals across southeast Michigan emergently restructured the majority of its operations to respond effectively to the pandemic. Every department made alterations to their practices and processes as part of surge capacity management which peaked in early April 2020 with 732 admitted patients with COVID-19 at HFHS hospitals, 310 admitted at Henry Ford Hospital (HFH) alone. About one-third of those were admitted to intensive care units (ICUs), 80% of whom were intubated. This paper showcases the methods by which a neurology department can transform and reorganise itself to address an unprecedented health crisis.
Departmental communication
Starting on 15 March 2020, the Chair of the department organised a ‘huddle call’ at 17:00 every day, open to all members of the department. The organisation of the huddles was based on his work of more than a decade in leading a Trauma Support Group for women with post-traumatic stress disorder. The agenda of the meeting began with department updates, particularly with news of successes in dealing with issues and follow-up to questions posed in the previous huddles in the past day or two, hospital updates from leadership meetings and announcements, review of dashboards from hospitals in the health system as well as dashboards from the State of Michigan, the adjacent Canadian province of Ontario and national data on the coronavirus. Many members of the department were tasked with reporting to the group over the course of the surge. Pertinent research and news articles with URLs and some summaries were discussed including a section on Correcting Misinformation to provide facts to counteract rumours and bad advice that was often seen on the internet or in social media. An open discussion would follow. The meeting would last 30–60 min and was attended by an average of 100 department healthcare providers (HCPs) and administrative members every night. It served as an effective way of communication, but also as a daily ‘debriefing’ session for team members in the middle of a healthcare crisis. In the first 2 weeks, the meetings were focused on ensuring the availability of personal protective equipment (PPE), the shutting down of all neurology outpatient and most inpatient activities, establishment of virtual care activity and seeking volunteers for redeployment openings listed by Incident Command on the daily leadership calls. Later discussions became more far ranging including discussion of the healthcare disparities especially concerning the disproportionate effect on African Americans in the Detroit area as well as the role of implicit bias in healthcare. While most of the reference materials were freshly published, in these broader discussions, venerable texts were cited going back to Plato’s Apology of Socrates and the value of living an examined life. The patient case conference was also part of the huddles when novel presentations were observed as front line clinicians discussed their patients and reports from journals were disseminated. Attendants were also reminded on a daily basis about mental health resources, and they received support from their supervisors and peers. A summary email was sent to all members of the department shortly after the call ended.
Infrastructure transformation
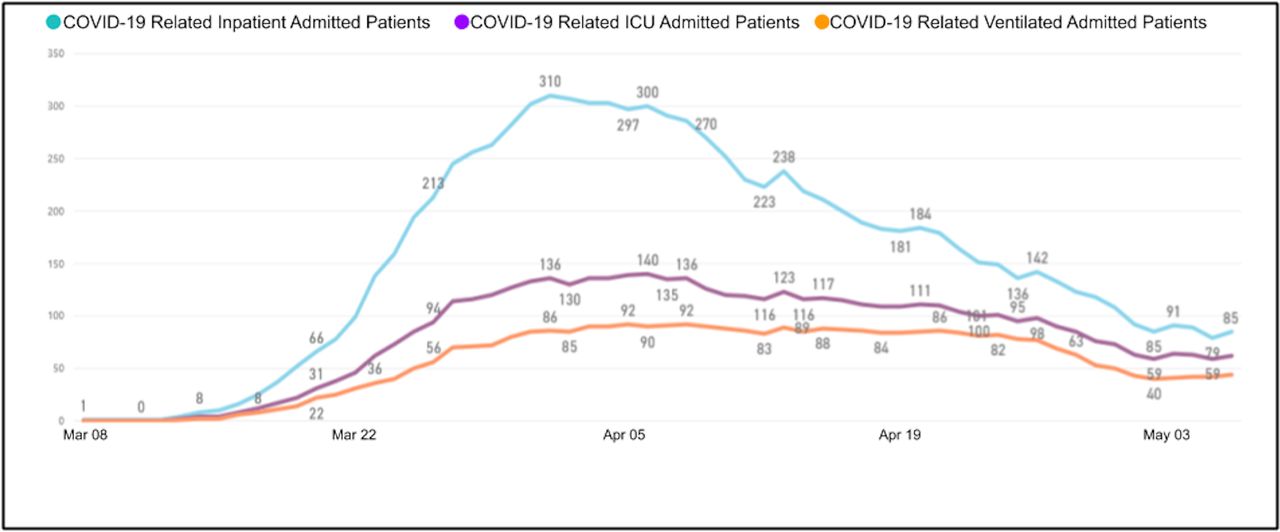
In early March 2020, elective admissions to our epilepsy monitoring units at two hospitals were put on hold due to infection risk, freeing eight beds at HFH and four beds at HF West Bloomfield Hospital (HFWBH) which became isolation units for patients with COVID-19. Within 2 weeks, as COVID-19 admissions took over our hospitals, our HFH stroke unit and neurology/neurosurgery inpatient ward were also converted to COVID-19 isolation units (figure 1).

Plot of COVID-19 total inpatients, ICU patients, and ventilated patients with COVID-19 at Henry Ford Hospital (adapted from the Henry Ford Hospital COVID-19 Dashboard). Prior to the pandemic, most patients in general wards were in semi-private rooms but all beds were converted to private rooms during the pandemic. Note that on 6 April 2020, the peak day for COVID-19 ICU admissions at 140 (with only 14 non-COVID-19 ICU patients that day), the Centers for Medicare and Medicaid Services (CMS)-adjusted Case Mix Index (CMI) was 1.822. The maximum CMI was reached on 4 May 2020 with a value of 3.910 when the majority of the patients with COVID-19 were intubated and/or in ICU beds. ICU, intensive care unit.
The stroke unit at HFH is split into two units. In order to expand the number of ICU beds, the larger unit, consisting of 18 beds, became an extension of the medical ICU (MICU) for patients with confirmed or suspected COVID-19 and was staffed by internal medicine (IM) physicians and residents. The smaller eight-bed unit became a step-down for COVID-19+ patients, also staffed by IM. Nursing in these units was provided by neurointensive care unit (NICU) and stroke unit nurses. Some of our neurology advanced practice providers (APPs) were redeployed to the emergency room (ER), MICUs, COVID-19 units and swabbing tents.
Inpatient neurology services
The inpatient services at HFH consist of the inpatient neurology service, consult service and NICU. Coinciding with the beginning of the pandemic, we saw a decline in our neurology admissions as patients sheltered at home and a Tier 1 Stroke Protocol was developed to discharge patients with transient ischemic attacks (TIA) and minor strokes from ERs with rapid telemedicine follow-up. This policy was in effect until mid-June 2020. Patients with stroke who received intravenous thrombolysis or endovascular interventions were admitted to the NICU, while patients with non-intervention stroke who could not be sent home from the ER were diverted to a non-COVID-19 telemetry unit, unless they were diagnosed or suspected of being infected. Neurological checks and National Institutes of Health Stroke Scale assessments were performed using video devices to limit exposure to HCPs. Consensus was reached between the stroke team, neurointerventional team and radiology on an amended policy to manage patients receiving thrombectomy during the pandemic. This policy stipulated performing thrombectomies of all eligible patients under general anaesthesia whether suspected to be infected or not. Intubation was to be conducted solely by the anaesthesia team to reduce the number of attempts. Postprocedure extubation, if applicable, was carried out in a negative-pressure room either in the recovery unit or the NICU, depending on the patient’s clinical condition.
The usual HFH inpatient consult service consists of two attendings, a senior and two junior neurology residents along with a couple of rotators and medical students, divided in two teams. One team covers the wards and ED, while the other covers the ICUs. During the pandemic, the service was downsized to one team only with a backup team on standby at home. Patients who could not reliably be screened for COVID-19 symptoms were assumed to be infected. In-room teaching was suspended, and staffing took place where social distancing could be practiced. The number of individuals entering the room was limited to one person, usually the attending. While initial evaluation happened face-to-face, follow-ups for patients with COVID-19 were usually done through chart review. Moreover, protocols guiding the management of routine neurological presentations like seizures, minor strokes, headaches and neuromuscular disorders were designed by each subspecialty and distributed to the emergency department (ED) staff. The goal was to emphasise provision of emergent care in the ER and limit admissions by expediting discharges from the ER when appropriate. An electronic report using analytic reporting tools was run each morning on all ER discharges to identify all patients with neurological symptoms and facilitate follow-up continuity of care within a few days of discharge through an urgent outpatient teleneurology clinic.
As a tertiary referral centre, our 16 bed semi-closed NICU is regularly occupied by an array of complex neurological and neurosurgical cases. When our volume of COVID-19 cases requiring ICU level care started to climb, temporary measures were put in place to reduce the number of outside transfers into the system. With the ensuing reduction in our NICU census and ever-increasing demand to staff COVID-19 medical units, we volunteered a lean rounding model in our unit, allowing our rotating trainees to be deployed to the ED or COVID-19 ICUs. The NICU was preferentially designated as a non-COVID-19 due to its open design, with less than half the unit having private rooms. Critically-ill patients with medical or neurological illnesses who tested negative for COVID-19 or were of lower suspicion, were transferred to the NICU under our primary care. Our patient census grew to be dominated by medical cases intermixed with our routine admissions.
A major focus was to keep our medical personnel safe. In early March 2020, the Chair, GLB, sent home a few staff who had informed him of medical conditions that would put them at risk for adverse outcome. When the huddles started on 15 March 2020, he asked anyone with health risks to voluntarily self-identify. Those who did were deployed off the front lines, as was anyone over the age of 60 years since this was identified to be the inflection point of increasing risk for adverse outcomes. Proactive steps were taken to provide PPE by ordering respirator masks for frontline providers in early March. To foster good sleep and reduce infection risk, a stroke staff was assigned to do a 12 hours night float, 6 days a week, taking everyone else off call. This night staff has worked on improving telemedicine consults at our six ERs and on wards at HFH. All staff were encouraged to wear scrubs and changing rooms were established in the neurophysiology labs at HFH and HFWBH.
Neurophysiological procedures and redeployment of technologists
Most outpatient electroencephalography (EEG), electromyography, transcranial doppler (TCD) and evoked potential studies were postponed. Triaging protocols for inpatient studies were created, prioritising studies deemed essential after discussion with the primary teams. In general, we saw a dramatic reduction in the number of all neurophysiological procedures performed within the healthcare system, both inpatient and outpatient (figure 2). In the case of EEGs, the protocol emphasised treating clinical seizures without monitoring and limiting EEGs to non-convulsive seizures and status epilepticus. Long-term EEGs were favoured over routine studies to decrease repeated exposures. In addition, alterations to the EEG procedure were made to ensure safety of our technologists. This included the use of paste and head wrap to fix the EEG leads instead of collodion and air gun. All provocative manoeuvres (eg, hyperventilation) were also limited to reduce aerosolisation. Long-term EEGs were monitored from home by technologists using hospital-issued laptops. Many neurophysiology technologists were redeployed to other duties wherever help was needed, ranging from pharmacy runners to environmental service duties.

Neurophysiology tests performed in the outpatient and inpatient settings at Henry Ford Health System from 6 January 2020 to 8 May 2020. Neurophysiology tests refer to electroencephalography, electromyography, evoked potential and transcranial doppler. 16 March represents the implementation date of the triaging policy for inpatient studies and the postponement of outpatient studies.
Outpatient neurology services
On 16 March 2020, with the first confirmed COVID-19 case in our hospital, outpatient neurology clinics closed at all seven locations. Procedures, such as biopsies, onabotulinum toxin injections and nerve blocks were postponed in order to limit exposure to patients and medical staff.
Telemedicine was implemented for new and follow-up visits. Of note, telemedicine in the outpatient setting had been very sparsely used in the neurology department prior to the COVID-19 pandemic (figure 3). A contributing factor to the slow adoption of telemedicine in neurology has been the traditional reliance on the neurological examination (strength quantification, sensation and reflex examination) for localisation and diagnosis.1 2

Video and telephone visits at Henry Ford Health System neurology department pre-COVID-19 and during the first month of COVID-19 pandemic.
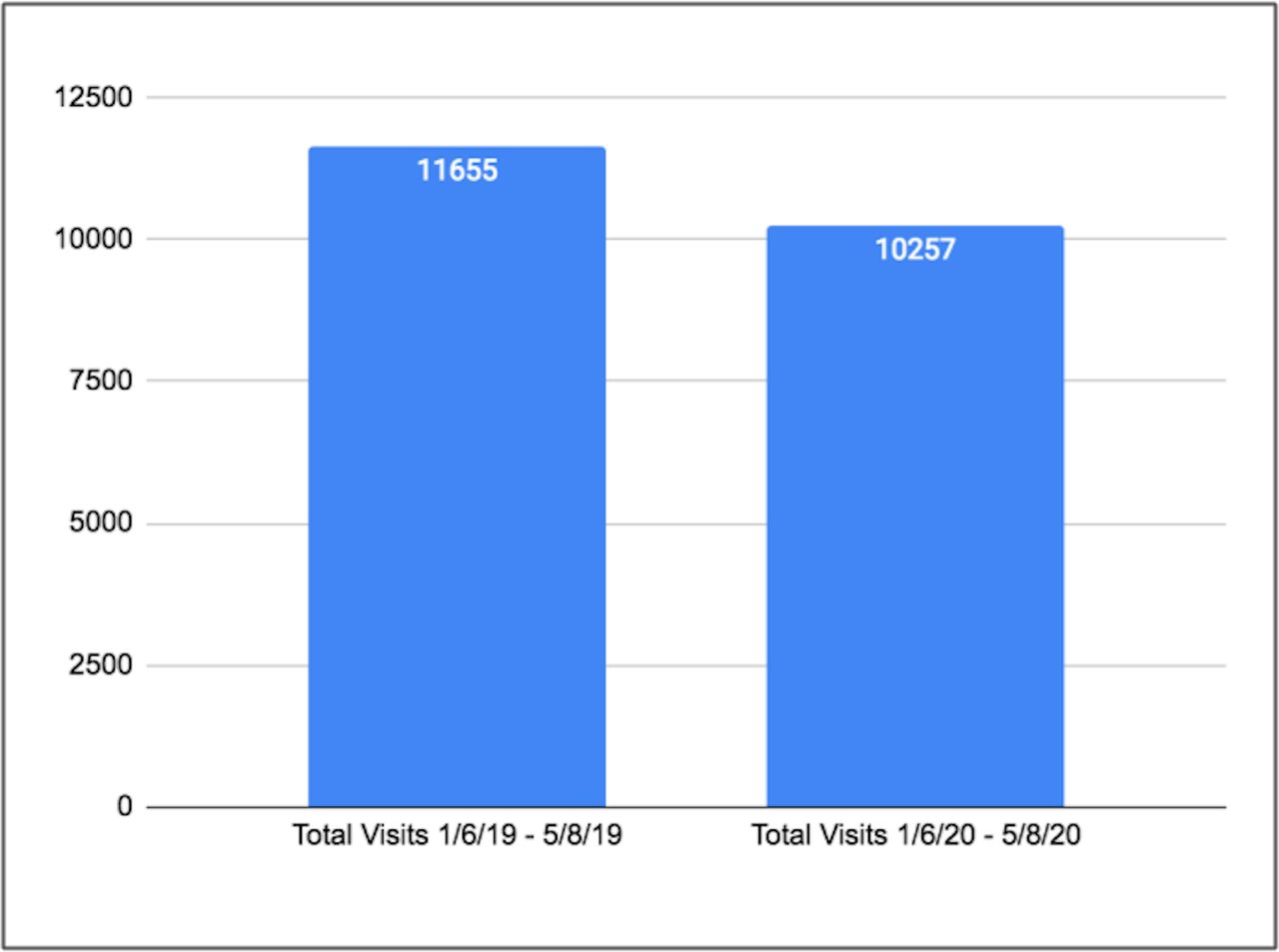
Enhanced information technology, billing department support and the daily departmental virtual huddles facilitated the nearly ‘overnight’ transition in the way ambulatory care became delivered. These efforts markedly increased the number of telemedicine visits compared with pre-COVID-19 period (figure 3). Ambulatory staff and call centre personnel worked remotely with our patients during this transition to provide guidance and instructions on how to engage in telemedicine visits. For patients who were unable or reluctant to use video visits, telephone visits were offered (figure 3). As a result, we were able to continue providing care to our patients at levels similar to the pre-COVID-19 period (figure 4). This also benefited residents who acquired significant telemedicine exposure.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of outpatient visits for 6 January 2019 to 8 May 2019 and the corresponding epoch in 2020 at Henry Ford Health System neurology department. A 12% decrease in outpatient visits was recorded in the 2020 epoch compared with the same epoch a year ago.
Nurses living in Canada were provided with the same corporate cell phones used by physicians, residents and APPs. Remote HIPAA-compliant access to the electronic health record was enabled for all so that in-basket work, prescribing and messaging were maintained without disruption. Provisional plans for hotels should the border be closed were developed but not used.
Residency response and medical education
All institutional residency and fellowships were deemed to be in a state of emergency and a contingency plan was established, preserving the 80 hours work week rules. Clinical rotations were divided into essential and non-essential rotations, taking into account programme requirements as well as service duties. Non-essential rotations were put on hold to decrease unnecessary resident exposure and to maintain a backup pool of providers. In addition, innovative solutions were used to decrease exposure on essential rotations. For instance, residents rotating in the NICU only covered on their call days, while residents on inpatient services alternated day coverage when patient census was low. External visiting rotators and medical students no longer participated in clinical rotations.
Several neurology residents were redeployed to provide care for patients admitted to the COVID-19 unit under the supervision of an IM staff. A coverage system was created to provide five neurology residents during the daytime, and one resident at night. Residents worked under supervision at all times and had all the needed PPE to perform their duties safely. They also had 10 days off between COVID-19 unit rotations to recuperate.
In order to facilitate teaching, all lectures were virtualised and uploaded to our internal website along with important guidelines from various societies (eg, American Academy of Neurology, American Academy of Neuromuscular & Electrodiagnostic Medicine) and links to electronic modules shared in the neurology community (eg, EEG modules, movement disorder videos). An online question bank was also used, and quizzes were assigned to residents to assist in their learning.
Research initiatives
In the face of rapidly accumulating COVID-19-related data, the department created a Scientific Advisory Board (SAB) in the early stages of the pandemic. Two committees came out of this initiative: an editorial board tasked with informing the department about COVID-19 and its neurological implications and a research committee responsible to study the impact of the pandemic on various aspects of neurological care.
The SAB Editorial Board consisted of 30 members from the neurology and research departments. All neurological subspecialties were represented and the interest spanned from medical students to faculty. The board’s first priority was to rapidly disseminate knowledge about the virus and its effects on the nervous system. The decision was therefore to issue a weekly scientific newsletter covering the latest on prevention guidelines, neuropathogenesis, diagnostic testing, neurological syndromes, the care of specific neurological patient populations during the pandemic and therapeutics. The newsletters were shared on Henry Ford’s social media outlets and website after obtaining approval from the media relations department.3
The research committee brought together medical students, scientists, neurology residents, fellows and faculty. The group was organised in teams who worked on several projects that investigated topics such as neurological manifestations encountered in our patients with COVID-19 and the pandemic’s impact on the care of specific neurological conditions such as epilepsy or stroke. Collaborations were created with other groups from medical centres in the area to share the experience and data. All research meetings were held via teleconferencing.
Phase I (shelter in place) research operations were declared on 1 March 2020. This allowed only critical activities needed to preserve the health and safety of human and animal subjects. With the scaled down operations of the institutional research enterprise, we were faced with the uncertainty of retaining our clinical research staff. Leadership placed a call for deployment of ambulatory and clinical research personnel to assist with the staffing needs of the health system’s EDs and inpatient units. Three neurology research nurses and one clinical research assistant were assigned to work in the MICU and ED. Many of the remaining clinical research staff were deployed to work on COVID-19-related research studies.
The very sudden and harrowing onset of COVID-19 generated a need by our neurology research laboratory to assure the survival of critical assets, including animal and cell resources. On 15 March 2020, after a potential exposure of an animal handler to COVID-19, researchers were informed that a cull of about 75% of the research animals was urgently needed due to a shortage of animal handlers. GLB was contacted by our research scientists and he in turn talked with Steven Kalkanis, CEO of the HFMG and Chief Academic Officer. After discussion with the research administration and the head veterinarian, a reasonable accommodation was reached by 18 March 2020. The accommodation, led by MC, was sensitive to the bioresources infrastructure issues as well as the needs of the scientists to preserve animal lines and ongoing research. A nuanced approach was reached which was acceptable to all parties. Research animals at HFH were moved to a secondary bioresource facility minimising the need to cull the animal colonies. Laboratory managers worked out a schedule to come to the laboratory to oversee maintenance of resources, and to monitor incubators, equipment, storage devices and manage outgoing and incoming orders to sustain the lab. Meetings and scientific presentations were maintained virtually. Meanwhile, key personnel were physically working in the laboratory to develop novel therapies for the treatment of COVID-19. A partial return of human and animal research activities began on 29 May 2020 with phase II Research Guidelines.
Challenges and learnings
By 15 June, 60 064 individuals in Michigan had tested positive for the virus and 5772 had died as a result of COVID-19 (case fatality rate of 9.6%). In the same time period, HFHS had registered a total of 7460 confirmed cases (12.4% of Michigan case volume) and 527-related deaths (9.1% of Michigan COVID-19 deaths) throughout its hospitals. Among the 5571 HFHS employees who were tested for SARS-CoV-2, 1031 (2.71% of HFHS employees) were found to be positive, including about a dozen staff members in the Department of Neurology, all of whom recovered without hospitalisation and returned to work. To counter the spread of infection to employees and patients, and in accordance with the Centers for Disease Control and Prevention (CDC) Infection Prevention and Control Recommendations for Healthcare Personnel During the COVID-19 Pandemic, HFHS instituted daily symptom and temperature screens for all incoming personnel, limited access to the buildings to select monitored entrances, provided face masks to all personnel at checkpoints and mandated that everyone wore them at all time while on Henry Ford premises.4 In addition, social distancing measures were adopted inside the facilities by limiting the number of people in elevators, maintaining the physical ‘6-feet’ distance between individuals in offices, lobbies, waiting rooms, cafeterias and break rooms. Employees who had to work in direct contact with patients were trained on how to don and doff PPE, and these measures were overseen by Infection Control representatives on a regular basis. Employee infections plummeted after the mandatory mask policy at all facilities was adopted on 7 April 2020.
During the months of March through May, visitation by family members was limited to specific instances such as end-of-life situations or surgeries, and the number of allowed visitors was also reduced. During the peak of the pandemic, waiting rooms were essentially closed to the public. To remediate these restrictions, in the NICU for instance, families were updated by nurses and providers on a daily basis via phone. An HFHS corporate smartphone was also made available for family members who wished to video-conference with their hospitalised loved ones.
Stress levels among HCPs reached unprecedented heights during the pandemic. Initially, there was great concern about supplies of PPE. Fortunately, one author, AMK, presciently started ordering PPE supplies in mid-February, succeeding in about 30% of his orders, so we were able to secure a few dozen 3M respirator masks which were distributed to those at the most risk of COVID-19. We also had an outpouring of PPE donations from friends and families of department members. We received enough donations that we were able to pass on the extra supplies to the central PPE command centre that had been set up for coordinating donations and purchases. So, while there were some tenuous days in the first couple weeks, our department members were able to work with adequate PPE throughout the surge.
HFHS created ‘The COVID-19 Emotional Support Team’ which made several interventions and resources available to employees. These included a virtual psychological first aid class, in-person or virtual peer processing support groups, and leaders conversation groups. The existing Employee Assistance Programme hotline was also in place for employees to reach therapists 24/7. An Institutional Review Board (IRB)-approved study conducted by several authors of the present paper, is currently underway to report on the stress level experienced by neurology residents and fellows during the pandemic. This study will also shed light on residents’ perception of other aspects of their training during the crisis, such as their medical education and redeployment experience.
The financial burden and losses incurred by the health system led to the difficult decision by the administration to furlough four dozen employees either full time or part time. This painful news was delivered to the department on the huddle call of 18 April 2020. The furlough mechanism allowed employees to keep their benefits including health insurance. For those employees making less than US$53 000 annually, the combination of the US$300 weekly state unemployment payment and the US$600 weekly federal unemployment payment from the Coronavirus Aid, Relief, and Economic Security (CARES) Act meant that their weekly pay was higher than they were getting from their usual work. Regular updates were sent systemwide to provide guidance during the furloughing process including access to special psychological support services. All Henry Ford Medical Group chairs began a voluntary contribution of 25% of their post-tax salary to a COVID-19 emergency needs fund to provide financial assistance to employees suffering financial hardship. This will continue until the time of hardship has ended. Most of the HFHS administrative leadership have also volunteered to contribute from 10% to 25% of their salaries to the same fund. There has been an outpouring of community support for this fund as well. By mid-June, all but a handful of neurology employees have been recalled back to work and nearly everyone else is expected back in July 2020.
Conclusion
Notwithstanding the associated health and financial hurdles, the COVID-19 pandemic underscored the indispensable roles of tight interdepartmental/intradepartmental collaboration, adaptability, cohesiveness and creativity in mitigating a health crisis of such magnitude. These qualities led our health system to undergo a rapid and targeted reorganisation of clinical care delivery. Our neurology department actively contributed its academic and clinical workforce and its infrastructure to this organised response, expanded its academic horizons and made an important transition to the much-needed teleneurology. At the time of writing, 7 weeks have elapsed since the first confirmed COVID-19 case in our health system and, although the epidemic peak may be behind us, much remains to be done to plan for the gradual return to normalcy, and to reflect on what was done right and what could have been done better.
Acknowledgments
We would like to acknowledge James Brachulis and Craig Brunskole for their work on the Henry Ford Hospital COVID-19 dashboard; Alex Bou Chebl, MD, for his input and drafting of policies; Cynthia Lang, Renee Krebs, Adelina Orejel and Donna McLaren for their help with data acquisition. Special thanks to the leadership and support of Steven Kalkanis, MD, CEO of the Henry Ford Medical Group (HFMG), Linda Gifford, COO of the HFMG for her efforts, and John Deledda, MD for his leadership of the Incident Command.
Footnotes
Twitter @RiadRmdn
Contributors ARR is the guarantor for the article. ARR and GLB had the original idea for the article. ARR, GLB and AMK reviewed the entirety of the article. ARR, OKA, MCerghet, MChopp, OD, KMG, MI, AMK, GAM, CBM, DSN, GO, JR, YS, IFZ and GLB contributed to the writing of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All data generated or analysed during this study are included in this published article.