Article Text

Abstract
Background Optic neuritis is recognised by the international classification of headache disorders as a painful cranial nerve lesion. A lumbar puncture may be performed in the investigation of optic neuritis. Postdural puncture headache (PDPH) due to intracranial hypotension is a frequent complication of this procedure. In contrast, cerebral venous thrombosis (CVT) is a rare but potentially fatal complication of dural puncture. A few studies have identified an association between iron deficiency anaemia and venous thrombosis. There are no reports linking CVT with lumbar puncture and iron deficiency anaemia.
Methods and results We present a 32-year-old woman with optic neuritis and iron deficiency anaemia complicated by a PDPH and CVT.
Conclusion CVT should be considered in a patient with persistent headache, recent lumbar puncture and iron deficiency anaemia. Early recognition and treatment of this condition are vital to avoiding mortality and morbidity.
- sinus thrombosis
- stroke
- headache
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Case
A 32-year-old woman with optic neuritis confirmed on MRI underwent a lumbar puncture and 1 day later, developed a diffuse headache and hyperacusis. The headache was exacerbated when upright and resolved when recumbent. There was a background history of miscarriage and bariatric surgery 6 years ago. She was taking no regular medications. Her body mass index was 36.8. Initial blood tests demonstrated microcytic hypochromic anaemia (haemoglobin 102 g/L, mean corpuscular volume 62.8 fL, mean corpuscular haemoglobin 19.8 pg) consistent with iron deficiency (ferritin 9 mg/L, transferrin 3.1 g/L, transferrin saturation 12%). B12 level was also reduced at 103 pmol/L (range: 150–750 pmol/L) and serum folate was normal. Antinuclear antibodies were elevated at 1:1280 with a negative extractable nuclear antigen and double-stranded DNA profile. Complement C3 was 0.12 g/L (range: 0.16–0.38) and C4 was 0.86 (range: 0.79–1.52). Cerebrospinal fluid (CSF) was normal. Neuromyelitis optica and antimyelin oligodendrocyte glycoprotein antibodies were negative.
She was treated with 5 days of intravenous methylprednisolone (1 g daily) for the optic neuritis and presumptively for a postdural puncture headache (PDPH) with bedrest, intravenous hydration and regular caffeine tablets. She experienced gradual improvement without full resolution of headache and was discharged home. At home, her symptoms evolved and she developed a continuous right frontal headache unchanged by posture.
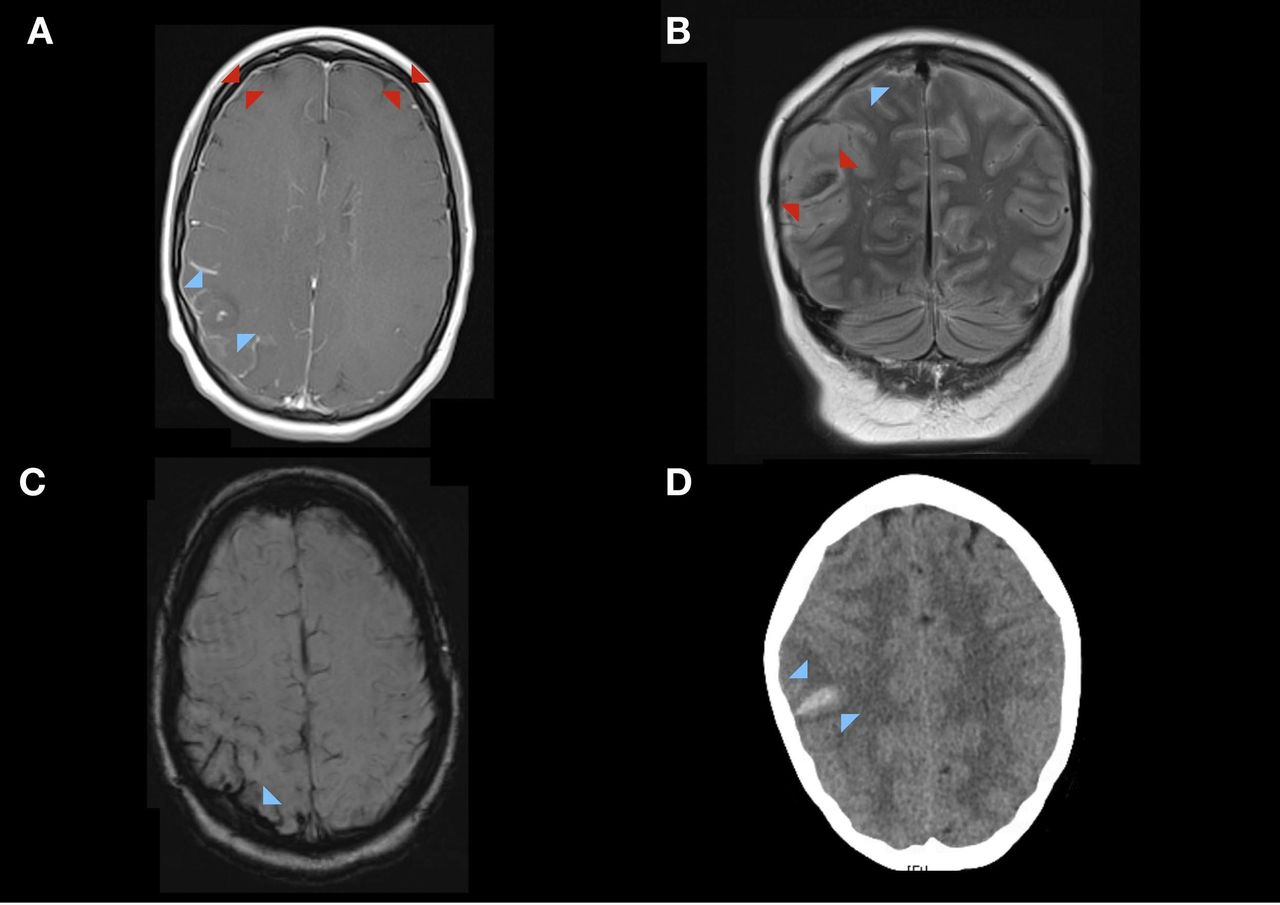
Five days after dural puncture, she re-presented to the hospital with a cluster of three witnessed generalised tonic–clonic seizures. Repeat MRI brain confirmed pachymeningeal enhancement consistent with intracranial hypotension (figure 1A), a right parietal cortical vein thrombosis (figure 1B) and small associated intraparenchymal haematoma (figure 1C,D). Antiphospholipid antibodies, thrombophilic and vasculitic screens were negative. Treatment with levetiracetam, intravenous heparin and warfarin was given. An iron infusion and vitamin B12 were replaced for nutritional deficiency related to the previous bariatric surgery. The seizures terminated and the headache resolved. She was discharged 7 days after admission. At follow-up, 8 weeks after discharge, she has returned to work and remains headache and seizure free. Progress MRI brain shows the evolution of the right parietal cortical vein thrombosis and surrounding haemorrhage and oedema.
{kind=link}
(A–D) MRI brain (day 5 post-dural puncture) T1-weighted post contrast axial sequences show (A) pachymeningeal enhancement (red arrows), hypointense area (blue arrows) with a focal area of enhancement and prominent surrounding cortical vein enhancement (B) abnormal flow in the right cortical vein (blue arrow) with intraparenchymal haematoma and surrounding oedema (red arrows). (C) Area of prominent signal hypointensity (blue arrow) on susceptibility-weighted imaging sequence with (D) corresponding hyperdensity (blue arrows) on non-contrast CT brain consistent with acute intraparenchymal haematoma.
Discussion
PDPH is a common complication following a dural puncture. The international classification of headache disorder stratifies PDPH as a subtype of headache due to low cerebrospinal fluid pressure.1 The pathophysiology of this condition remains poorly understood. Studies have failed to demonstrate a consistent relationship of PDPH symptoms with opening or closing pressure.2 Incidence varies between 4.2% and 11%3 depending on the presence of various risk factors. The main modifiable risk factors include technique and needle type.
Cerebral venous thrombosis (CVT) is a rare but important cause of stroke in young people associated with significant morbidity and mortality.4 A predisposing condition is identified in the majority of CVT.4 Widely accepted risk factors include gender, obesity, genetic thrombophilia, inflammatory disorders (as in our patient) and malignancy. There is a lesser-known association between anaemia and CVT.5 In particular, several studies have linked the subtype of iron deficiency anaemia to venous thromboembolism including CVT.6 7 The mechanism for this association is unclear. Iron deficiency has been linked to thrombocytosis and increased levels of factor 8, both of which have been associated with thrombosis. Similarly, CVT following dural puncture is a rare but recognised complication. It has been described mostly in small retrospective studies and case reports.7 8 These studies report between 16% and 19.6% of patients with CVT had a preceding dural puncture.9 10 Importantly, all patients in the study by Guner et al had an additional predisposing risk factor for CVT including inherited thrombophilia or malignancy.9 The pathogenesis of CVT after a dural puncture is poorly understood. Several mechanisms have been proposed including damage to venous endothelium due to stretch from negative spinal–cranial pressure, decreased venous velocity and reduced absorption of CSF in the sinuses. This is the first reported case of CVT in the context of iron deficiency anaemia and recent dural puncture.
Conclusion
Our case highlights the importance of early investigation for an evolving headache postdural puncture. Additional caution should be exercised in the presence of iron deficiency anaemia. CT and MR venography are easily accessible non-invasive methods for rapid and accurate diagnosis of CVT. Early recognition of this condition facilitates timely management with anticoagulation.
Footnotes
Contributors LSE was the principle author of the manuscript. RC provided expert advise on image interpretation and selection. CC-S was involved in conception, drafting and revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data sharing not applicable as no datasets generated and/or analysed for this study.