Article Text

Abstract
Background The severity of Parkinson’s disease (PD) is difficult to assess objectively owing to the lack of a robust biological marker of underlying disease status, with consequent implications for diagnosis, treatment and prognosis. The current standard tool is the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS), but this is hampered by variability between observers and within subjects. Postural sway has been shown to correlate with complex brain functioning in other conditions. This study aimed to investigate the relationship between postural sway, MDS-UPDRS and other non-motor measures of disease severity in patients with PD.
Method 25 patients with PD and 18 age-matched controls participated in the study. All participants underwent assessment of postural sway using a force plate, with eyes open and closed. In addition, participants underwent tests of cognition and quality of life: Montreal Cognitive Assessment (MoCA), Neuropsychiatry Unit Cognitive Assessment (NUCOG) and, for the patients, the Parkinson’s Disease Questionnaire (PDQ-39–1), and assessment of clinical status using the motor component of the MDS-UPDRS.
Results Patients swayed significantly more than controls. This was most obvious in the eyes-closed condition. Sway path length showed strong correlations with PDQ-39–1, MoCA and the verbal fluency component of the NUCOG, and, to a lesser degree, with the UPDRS-III in patients with PD.
Conclusion These results suggest that motor and non-motor symptoms of PD are associated in patients, and, in particular, that postural sway shows potential as a possible measure of underlying disease status in PD, either alone or in combination with other measures.
- Parkinson's disease
- cognition
- motor physiology
- cognitive neuropsychology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Parkinson’s disease (PD) is associated with deficits in dopaminergic pathways in the brain, most notably those arising from the substantia nigra, though many other areas are involved. PD is characterised by tremor, rigidity, slowness of movement (bradykinesia) and postural imbalance. Potential non-motor symptoms include cognitive impairment, depression, fatigue, apathy, loss of smell and taste, and other sensory disturbances.1
The Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) is the tool most widely used to measure disease status in PD. However, the MDS-UPDRS is problematic in that it is subjective, shows day-to-day fluctuation and inter-observer variability, and does not provide a clinically useful estimate of disease prognosis.2 PD progression rates are very variable across patients,3 and there is therefore an urgent need to identify sensitive, reliable and objective markers to increase diagnostic specificity, determine the current stage of disease, and provide prognostic information.4 One potential marker is measurement of postural control, which shows some promise in identifying and tracking disease progression in early PD.5
A cardinal feature of all forms of Parkinsonism is impairment of posture and balance. Clinically, this manifests as abnormalities of gait and righting reflexes, though abnormalities can be subtle in the early stages.6 7 Postural adjustments made while standing still are easily measured, yielding a sophisticated set of measures of postural sway.8 9 Assessment of postural sway may therefore have a possible role in tracking disease progression and, perhaps, in informing diagnosis and providing prognostic information about patients with PD, either on its own or in combination with other measures.
Postural sway is defined as the movement of the body’s centre of mass (CoM) in the horizontal plane while standing.10 This can be measured by standing subjects on a force plate and detecting movement of the centre of pressure (CoP) in real time. Sway can be evaluated either while subjects are standing still or while they are moving.11 There is evidence that concurrent performance of cognitive tasks affects the pattern of sway in PD,12 even in the prodromal stages of the disease. A study of patients with idiopathic rapid eye movement (REM) sleep behaviour disorder (many of whom went on to develop PD) showed that sway patterns during cognitively challenging conditions could distinguish patients from controls.13 This is consistent with the notion that patients with impaired postural control invoke more conscious, cognitive mechanisms to compensate for their underlying deficit.14
Postural control is a complex neurological process requiring integration of visual, proprioceptive, and vestibular information to ensure that the CoM stays within the base of support.15 Deviation of the centre of mass is detected by proprioceptive and kinaesthetic systems which lead to compensatory motor mechanisms that prevent falling and generate anticipatory mechanisms to prepare the body for upcoming changes in the CoM and/or base of support. These compensatory motor mechanisms require constant updating of motor programmes and corresponding muscle activity over short periods of time. Neurological or musculoskeletal disorders may interfere with rapid updating of these programmes and can therefore result in falls or a highly unstable stance. Impairment in proprioception and kinaesthesia may also prevent detection of small postural fluctuations, leading to a delayed or incorrect motor response.
Postural instability in PD is likely to arise from a combination of disordered proprioception and impaired motor control.16 There is substantial evidence that patients with PD have abnormal proprioception under both passive and active conditions.17 18 The abnormal proprioception exacerbates postural instability,19 but patients appear to be able to compensate by using visual information.20
In addition, patients with PD are often unable to generate appropriately-sized long-latency postural reflexes in response to postural perturbation, consistently underestimating the appropriate muscular response.21 This leads to insufficient postural correction in response to a destabilising stimulus and so increases the risk of falling. In order to compensate for both sensory and motor impairment, patients may employ more cognitive strategies to maintain stable posture. Progressive failure of these strategies as the disease deteriorates would, in turn, result in worsening of postural control. In support of this hypothesis, previous studies have found that cognitive function and mood (anxiety and depression) were correlated with measures of gait and balance in PD.22 23
Another consideration is that the increased muscular rigidity which occurs in PD could reduce spontaneous sway while, on the other hand, dopaminergic therapy might increase sway by reducing rigidity.24 The effects of dopaminergic medication on postural sway are therefore potentially complex.25
This study aimed to investigate the combined use of postural sway, cognition and quality of life to assess disease severity in PD with the ultimate aim of developing a valid, reliable, quantifiable and objective measure of disease status. The tests involved were selected to be robust and time-efficient so that they would translate easily into a clinical setting, thereby having the potential to assist clinicians with diagnosis, measurement of response to treatment, and determination of prognosis. We hypothesised that patients would exhibit increased postural sway in comparison to controls, and that this increase in sway might also be related to cognitive functioning in patients.
Methods
Participants were recruited through the neurology, aged care and movement disorders clinics at The Canberra Hospital and through the Parkinson’s ACT Association. Patients had to be English-speaking, over 18 years of age, and have mild-to-moderate PD without other significant medical or surgical condition which could interfere with postural control. Exclusion criteria included a history of any other movement disorder, a diagnosis of cognitive impairment, a history of developmental disability, alcohol or substance abuse, or a psychiatric disorder not arising from PD. Age-matched and sex-matched controls without PD were recruited from partners of patients and via community advertisement. The same exclusion criteria applied to the controls. In this study, patients could be studied at any time relative to timing of medication, but had to be ON at the time of the study. This was done in order to facilitate patients’ journeys to the hospital.
Clinical measures
Clinical information was obtained regarding demographic features, medical history, dates of PD symptom onset and diagnosis, medication history including current medication regimen and session-specific information including time of last medication dose. Patients underwent neurological examination and assessment using MDS-UPDRS.26 The MDS-UPDRS was administered to all patients by a single, trained clinician, and these scores were calibrated with another clinician’s score on the first few patients, and several times during the course of data collection. All patients were diagnosed by a qualified neurologist, and clinical notes confirmed they fulfilled the Queen Square diagnostic criteria for PD.
Neuropsychiatric and cognitive assessments
These included: (1) the Montreal Cognitive Assessment (MoCA27) for staging cognitive impairment; (2) the Neuropsychiatry Unit Cognitive Assessment Tool (NUCOG28) to provide a domain-specific profile of cognitive function (attention, executive function, language, memory and visuospatial); (3) the Parkinson’s Anxiety Scale, specifically validated to assess anxiety in PD (PAS29); and (4) the Hamilton Depression Rating Scale, the standard tool used in PD (HAM-D-2430). The Parkinson’s disease Questionnaire (PDQ-39–131) was used to assess quality of life for the Parkinson’s patients.
Postural sway data collection
Postural sway data were collected using a Bertec Balance plate (Bertec, Columbus, Ohio, USA). Participants were asked to stand in a comfortable position with their feet within marker guides on the plate. Participants were asked to stand for 90 s with eyes open and then 90 s with eyes closed. All patients were in the ‘ON’ state when tested.
Sway data processing and statistical analysis
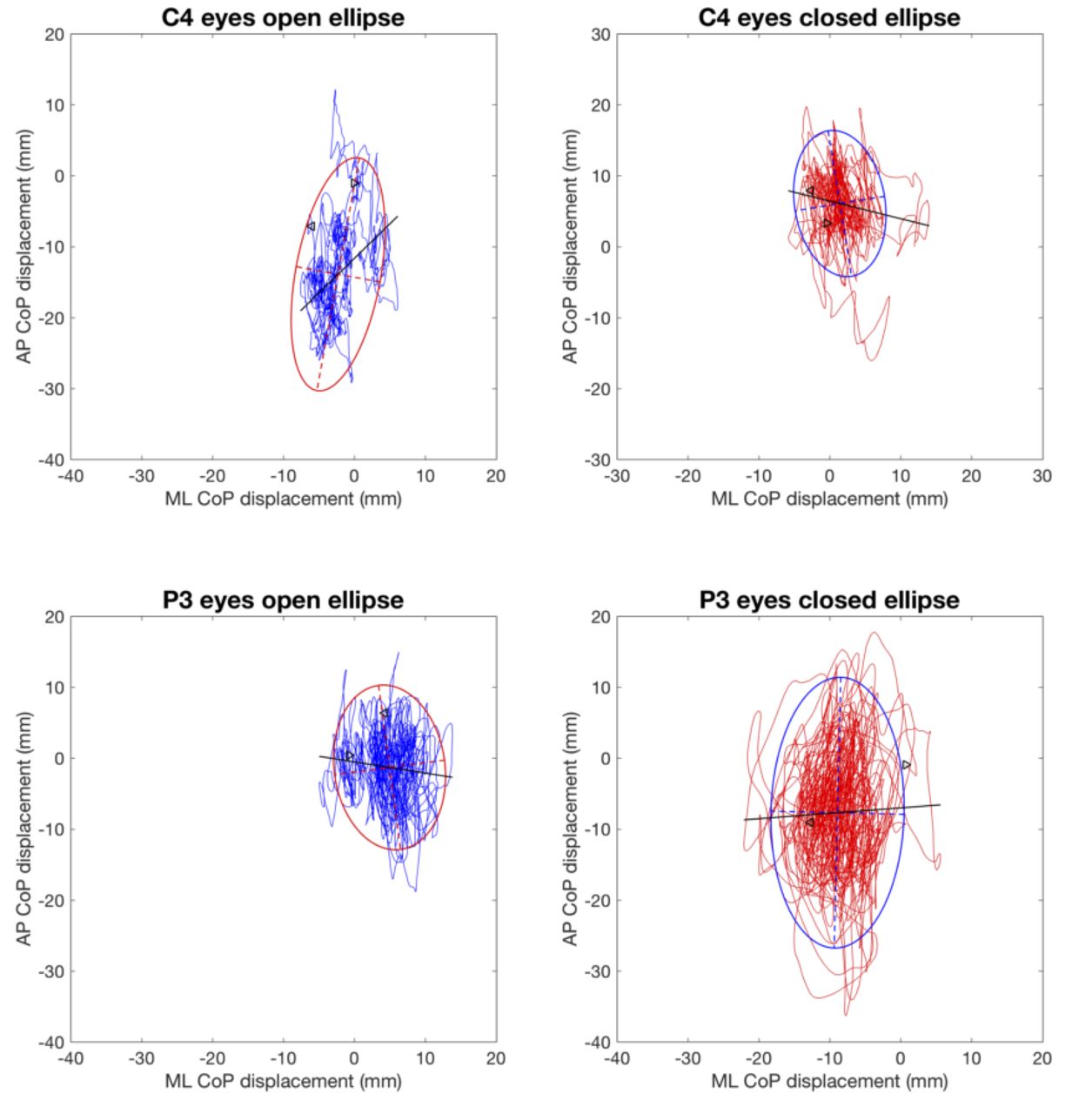
Examples from individual subjects are shown in figure 1. Analysis of postural sway data was carried out using custom MATLAB software designed specifically for this analysis.9 Each 90 s recording was assessed by selecting three consecutive 20 s segments after discarding the first 10 s, and then averaging the results of the three segments to generate a single value which was subsequently used for further analysis. Four measures were used to assess sway: sway area,32 sway path length,33 and the SD of CoP fluctuation in both the anteroposterior (AP) and mediolateral (ML) planes.34 A log transformation was performed where appropriate to correct for skew in the data. Mixed two-way analyses of variance examining the effects of group (PD versus controls) and eye condition (eyes open versus eyes closed within subjects) were performed. When comparing sway with the MDS-UPDRS and tests of cognitive function, a Spearman’s Rho was used to take account of non-normal distributions.
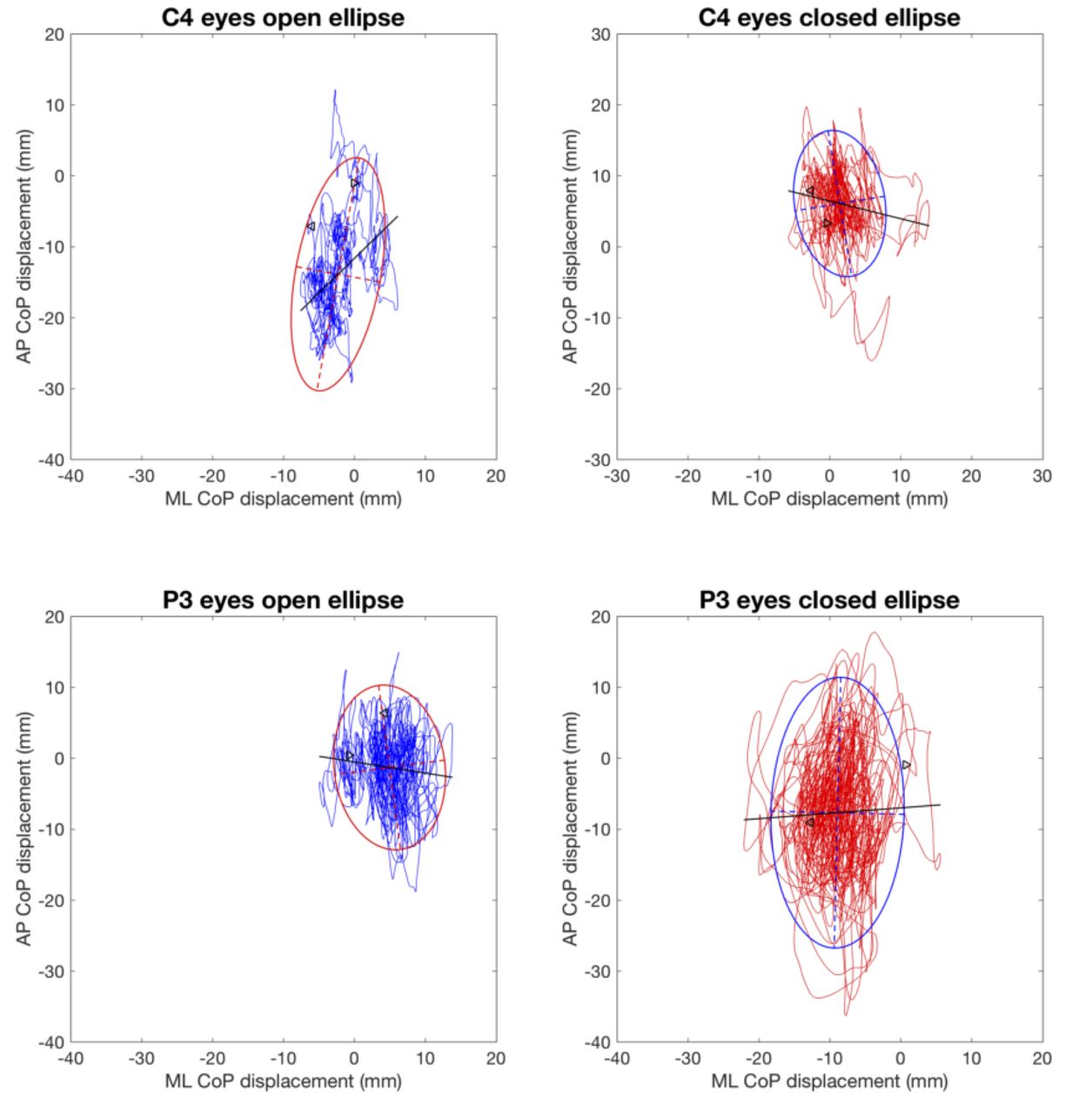
Example of data from two individual subjects (control on top and PD below) showing ellipse fits (sway area) with eyes open (blue) and eyes closed (red). CoP, centre of pressure; ML, mediolateral; PD, Parkinson’s disease.
Results
Demographics
A total of 27 patients and 18 age-matched controls were recruited. One patient was subsequently excluded when the diagnosis was changed to progressive supranuclear palsy, and one due to having insufficient clinical information on file, leaving 25 patients for further analysis. Descriptive statistics are reported in table 1. There was no significant difference between groups for either age or weight. There was also no significant difference between groups for handedness or gender. There were, however, significantly higher levels of depression in PD compared with controls, as measured by the HAM-D, as well as higher levels of anxiety (HAM-A). In addition, patients with PD scored slightly lower on the MoCA, although this difference was not significant.
Demographic variables for patients and controls
Sway: PD versus controls
Patients with PD demonstrated different sway patterns compared with age-matched controls as demonstrated by sway area, sway path length, and SD of postural sway. As shown in figure 2, there was a significant main effect of group on sway area (patients’ sway extended over a greater area than that of controls,  ,
,  ,
,  ,
,  ) and a marginally significant effect of eye condition (sway area was greater with eyes closed,
) and a marginally significant effect of eye condition (sway area was greater with eyes closed,  ,
,  ,
,  ,
,  ), but there was no interaction between group and eye condition,
), but there was no interaction between group and eye condition,  ,
,  ,
,  ,
,  .
.

Log-transformed sway area (left) and sway path length (right) for all participants. Means are shown by black horizontal bars. Individual scores are represented by circles, slightly jittered for clarity; coloured areas represent 95% highest density intervals, calculated using R’s BEST package, and vertical bars represent the 10th and 90th quantiles. The thin grey-lined envelopes show the full densities for each group. BEST, Bayesian estimation supersedes the t-test; PD, Parkinson’s disease.
For sway path length, patients with PD demonstrated greater average sway path length with eyes closed compared with eyes open. Similar to sway area, there was a significant effect of group,  ,
,  ,
,  ,
,  , and eye condition,
, and eye condition,  ,
,  ,
,  ,
,  , but, unlike sway area, there was a significant interaction between group and eye condition,
, but, unlike sway area, there was a significant interaction between group and eye condition,  ,
,  ,
,  ,
,  . As shown in figure 2 (right), this was mainly attributable to the greater overall difference between the eyes open and closed conditions for PD.
. As shown in figure 2 (right), this was mainly attributable to the greater overall difference between the eyes open and closed conditions for PD.
The SD of postural sway showed a significant difference between patients and controls in the AP axis,  ,
,  ,
,  ,
,  , but there was no significant interaction between group and eye condition,
, but there was no significant interaction between group and eye condition,  ,
,  ,
,  ,
,  (see figure 3, left). ML SD again showed a significant effect of group,
(see figure 3, left). ML SD again showed a significant effect of group,  ,
,  ,
,  ,
,  , but no significant effect of eye condition,
, but no significant effect of eye condition,  ,
,  ,
,  ,
,  , or interaction,
, or interaction,  ,
,  ,
,  ,
,  (see figure 3, right).
(see figure 3, right).

Log-transformed SD of AP sway (SD_AP, left) and mediolateral sway (SD_AP, right) for all participants. Means are shown by black horizontal bars. Individual scores are represented by circles, slightly jittered for clarity; coloured areas represent 95% highest density intervals, calculated using R’s BEST package, and vertical bars represent the 10th and 90th quantiles. The thin grey-lined envelopes show the full densities for each group. AP, anteroposterior; BEST, Bayesian estimation supersedes the t-test; PD, Parkinson’s disease.
Sway in PD versus clinical measures
Our exploratory analyses indicated that both sway path length and sway area correlated with clinical measures of movement (MDS-UPDRS), cognition (MoCA, NUCOG) and quality of life (PDQ-39–1). Because the correlations with sway path length were somewhat stronger, these will be presented here. Similarly, while both eyes-closed and eyes-open measures correlated with clinical and cognitive measures in PD, only eyes-closed measures are provided in the following section. The full dataset is available on Figshare (https://doi.org/10.6084/m9.figshare.7716614). There was no significant correlation between any measure of sway and any clinical measure in control subjects.
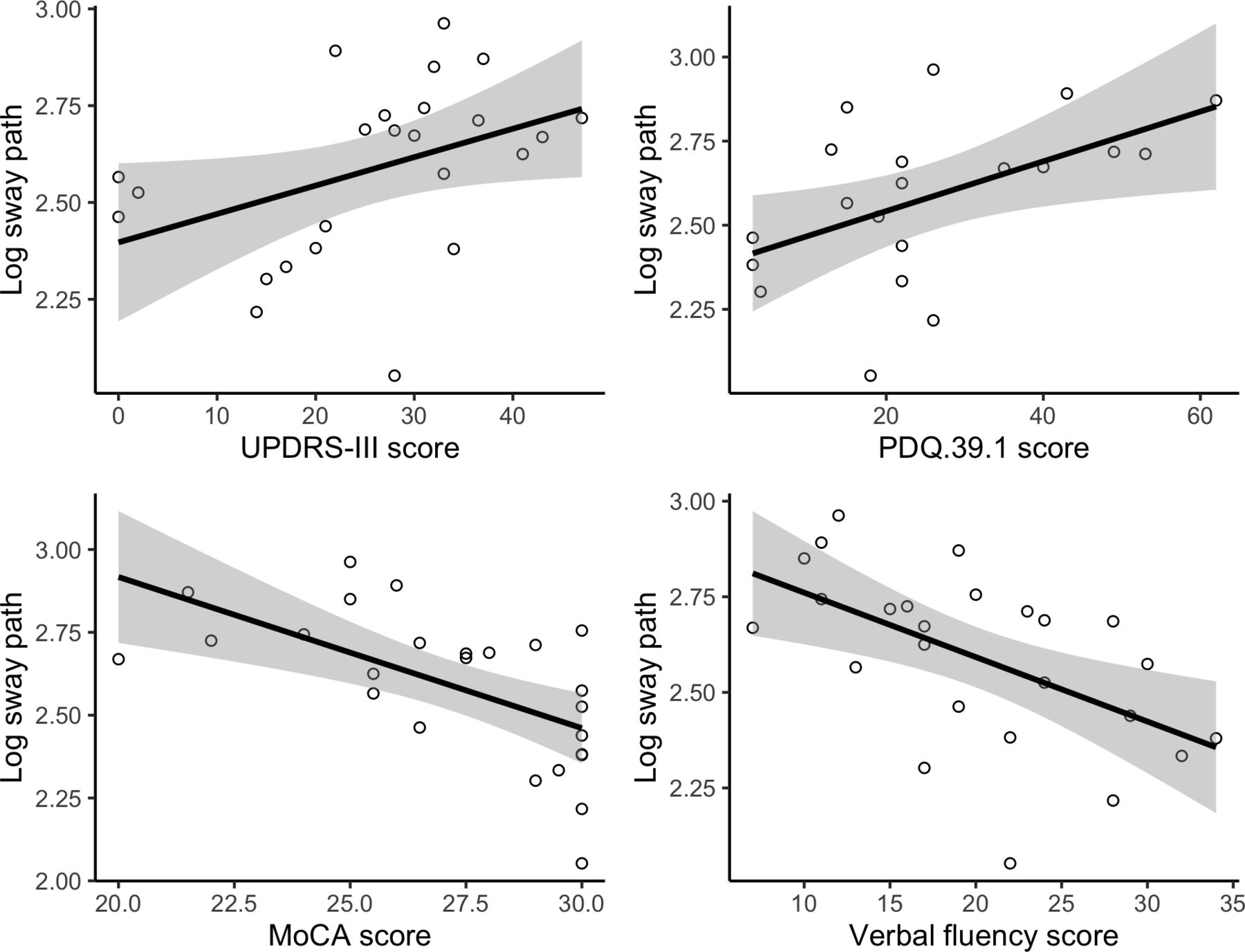
In patients with PD, there were strong correlations between sway path length (eyes closed) and UPDRS-III,  ,
,  ,
,  , MoCA,
, MoCA,  ,
,  ,
,  , verbal fluency/executive function subscale of the NUCOG,
, verbal fluency/executive function subscale of the NUCOG,  ,
,  ,
,  , and PDQ-39–1,
, and PDQ-39–1,  ,
,  ,
,  , as shown in figure 4.
, as shown in figure 4.

Scatter plot matrix showing the correlations between log-transformed sway path and the UPDRS-III, PDQ-39–1, MoCA and the verbal fluency/executive function subscale of the NUCOG (Animals test). MoCA, Montreal Cognitive Assessment; NUCOG, Neuropsychiatry Unit Cognitive Assessment; PDQ-39–1, Parkinson’s Disease Questionnaire; UPDRS, Unified Parkinson’s Disease Rating Scale.
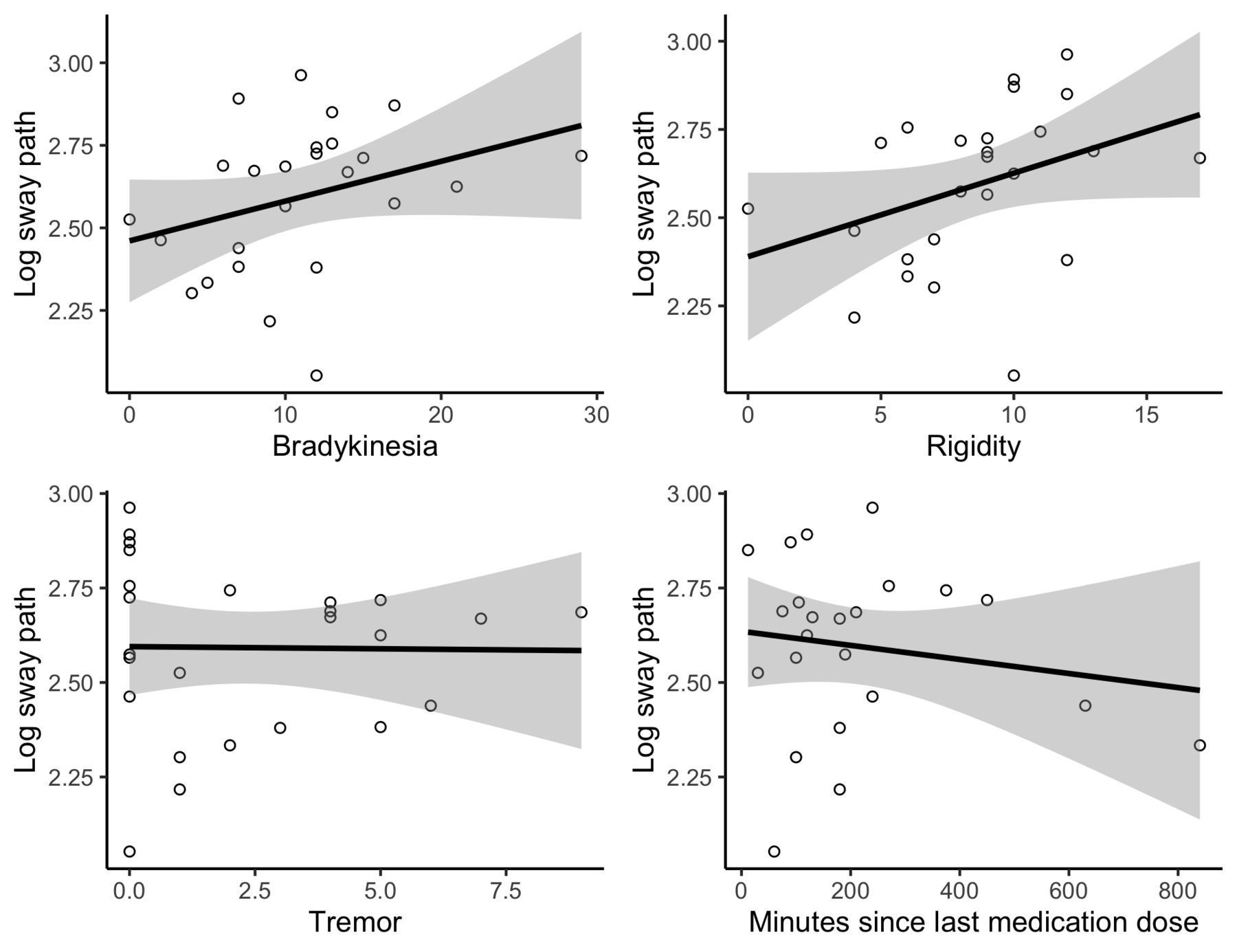
Since the MDS-UPDRS-III has separate items to assess bradykinesia, rigidity and tremor, we thought it would be useful to examine these separately in terms of their relationships with sway magnitude, since bradykinesia and rigidity might be considered more likely to affect sway than tremor. We also examined whether there was any relationship with the amount of time since last medication, since all patients were examined in the ‘ON’ condition, but some may have been more affected by medication than others.
Interestingly, there was a significant correlation between bradykinesia scores and sway path length (eyes closed),  ,
,  ,
,  , and also a moderate correlation with rigidity scores,
, and also a moderate correlation with rigidity scores,  ,
,  ,
,  , but no correlation with tremor scores,
, but no correlation with tremor scores,  ,
,  ,
,  , and also no relationship between path length and the number of minutes since last medication dose,
, and also no relationship between path length and the number of minutes since last medication dose,  ,
,  ,
,  , as shown in figure 5. There was also, not unexpectedly, a significant correlation between sway and the number of years since diagnosis,
, as shown in figure 5. There was also, not unexpectedly, a significant correlation between sway and the number of years since diagnosis,  ,
,  ,
,  . Note, however, that these are exploratory correlations which have not been corrected for multiple testing, and thus should ideally be explored in a new, higher-powered sample.
. Note, however, that these are exploratory correlations which have not been corrected for multiple testing, and thus should ideally be explored in a new, higher-powered sample.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scatter plot matrix showing the correlations between log-transformed sway path and the subscales of the UPDRS-III, as well as time since last dose of medication (in minutes). UPDRS, Unified Parkinson’s Disease Rating Scale.
Discussion
Sway: PD versus controls
As a group, patients with PD showed significantly greater sway compared with age-matched controls for all measures tested. Eye closure in controls was associated with increased sway, as expected, but the difference did not reach significance. However, there was a significant effect of eye closure in patients with PD.
The group differences were most obvious for sway area and SD in the AP axis, but differences were also present (particularly in the eyes closed condition) for sway path length, and SD in the ML axis. Interaction between group and eye condition was most evident for sway path length, but it was also seen in SD in the AP axis. Interestingly, this pattern differs from that seen in schizophrenia and schizotypy, where increased sway is also a feature, but there is no interaction between group and eye condition, and no correlations are seen with cognitive measures;8 in the current study, interactions with group were seen, suggesting that relationships between different sensory conditions may be important in differentiating sway results.
Sway in PD versus clinical measures
There was a significant negative correlation between postural sway path length and the total MoCA score, that is, increased sway path length was associated with poorer overall cognitive function. This effect was only found in patients with PD and is consistent with previous results from a study comparing body-mounted monitor measures of postural sway and general cognitive function assessed using the total Mattis Dementia Rating Scale.35 The fact that a correlation was not found in controls is consistent with studies of static balance and sway in the general older population which have found no correlation between the MoCA and measures of sway.13 36
There was also a significant negative correlation between postural sway path length and verbal fluency/executive function (NUCOG), that is, increased sway path length was associated with poorer executive cognitive function. This result is similar to that of a previous study which found an interaction between executive function (Trail-making task and components of Addenbrookes Cognitive Examination) and postural sway in persons with mild cognitive impairment.37 Similarly, sway was negatively correlated with executive function on animal-naming and trail-making tasks in community-dwelling elderly subjects.38
Postural sway path length correlated positively with PDQ-39–1 scores, that is, increased sway path length was correlated with poorer quality of life. This relationship is consistent with a previous study of patients with PD showing a significant correlation between measures of sway and the PDQ-39-mobility.39
As expected, there was also a positive correlation between postural sway path length and the UPDRS-III, that is, increased sway path length was correlated with poorer motor function, again consistent with previous studies using body mounted monitor measures of postural sway (iSway).39 Interestingly, postural sway path correlated more strongly with the MoCA, the verbal fluency component of NUCOG, and the PDQ-39–1 than with the MDS-UPDRS motor summary score (UPDRS-III). This suggests that the MDS-UPDRS may be less indicative of underlying global brain function than other measures such as postural sway, a finding which is consistent with the original purpose of the MDS-UPDRS which was designed as a tool to measure response to medication rather than to assess overall disease progression.2
Strengths and limitations
This is, to our knowledge, the first paper to specifically examine the relationships between sway magnitude and specific cognitive and quality-of-life measures in patients with PD. Although preliminary and purely correlational, it provides compelling evidence for further exploration of the relationship between motor and non-motor symptoms in PD, often conceptualised as progressing separately. A future study should examine these longitudinally in the same patients and expand the sample to include enough patients to enable examination of PD subtypes. If these relationships differ between PD subtypes, this could aid differential diagnosis in the future.
In terms of practical application, it may not be feasible for all clinicians to routinely include force-plate assessment, but simple force plates are relatively inexpensive and, indeed, some researchers have used the commonly available Nintendo Wii Balance Board. The measurement itself takes very little time (90 s each for eyes open and eyes closed conditions), and simple analysis software is commercially available.
While the power of this study is relatively low, and the correlational analysis is exploratory rather than confirmatory, the results suggest that it is important to follow up this study in larger, more diverse samples.
Conclusion
The results presented in this study suggest that postural sway has excellent potential to be used as a sensitive measure of disease severity and global brain function in PD. It also suggests that motor and non-motor features of PD may progress concurrently, something which is worthy of further investigation. Postural sway may prove particularly useful as a measure of disease severity if combined with other measures.
Further analysis using machine learning and imaging studies is currently underway in this and other research groups. This raises the exciting possibility that we may be moving towards the development of a better gold standard for diagnosis, measuring disease progression, and prognosis in PD.
References
Footnotes
Twitter @deborahapthorp
Contributors DA, CJL, CD and JCLL designed the study. AS and SI collected the data. DA, RV and AS analysed the data. RV and CJL performed additional clinical record checks. DA and JCLL drafted the manuscript. All authors were involved in writing and revising the manuscript.
Funding This study was funded by The Harry Secomb Foundation (IPAP201600839).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the ACT Health Human Research Ethics Committee (approval no. ETH.4.16.060).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. All data and code for producing the figures, statistics and manuscript are publicly available on Figshare. Apthorp, Deborah; Looi, Jeffrey; Lueck, Christian; Ilschner, Susanne; Smith, Alex; Das, Chandi (2019): Postural sway correlates with cognition and quality of life in Parkinson’s Disease: Data and R Markdown Code. figshare. Dataset. https://doi.org/10.6084/m9.figshare.7716614.