Article Text

Abstract
Objective Subtle cognitive deficits can occur during the prodromal phase of Parkinson’s disease (PD), commonly in conjunction with hyposmia. However, little is known about the association between cognitive function and other features suggestive of prodromal PD. We evaluated the association of non-motor prodromal PD features, including hyposmia, constipation and probable REM sleep behaviour disorder (pRBD), with objective measures of cognitive function and self-reported cognitive decline.
Methods The study population comprised 804 men who responded to a telephone cognitive interview in 2016–2017. Participants included 680 individuals with hyposmia, of whom 45 had confirmed PD, and 124 men without hyposmia. Among these men, we evaluated objective cognitive function and subjective cognitive decline to determine whether the presence of non-motor features of prodromal PD was associated with cognitive functioning. Analyses were adjusted for age, physical activity, body mass index, smoking status and coffee consumption.
Results Individuals with non-motor features of prodromal PD had worse objective and subjective cognitive performance relative to men without non-motor features. Cognitive impairment was particularly prevalent among individuals with concurrent hyposmia, pRBD and constipation (multivariate-adjusted OR=3.80; 95% CI 1.52 to 9.47 for objective poor cognitive function; OR=8.71; 95% CI 3.18 to 23.83 for subjective cognitive decline). As expected, both objective (OR=7.91) and subjective (OR=17.42) cognitive impairment were also more common among men with confirmed PD.
Conclusions Our study suggests that cognition is commonly affected in individuals with non-motor prodromal PD features, particularly when multiple of these features are present.
- cognition
- parkinson's disease
Data availability statement
Data are available on reasonable request. Data, methods and materials used to conduct this research article were carefully documented. Data will be shared at the request of other investigators for purposes of replicating procedures and results.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Subtle cognitive deficits are often present at the time of diagnosis of Parkinson’s disease (PD),1 and affect over 80% of patients 20 years after diagnosis.2 More recently, it has been reported that, in some individuals, cognitive deficits can be detected during the prodromal phase.3 However, data on cognitive function in prodromal PD (ProPD) are scarce, and cognitive function in this prodromal stage remains poorly characterised.
Existing studies have been limited by small samples sizes,4 non-comprehensive assessments of cognitive function,5 6 or have assessed cognitive function in isolation or in association with a single feature of ProPD.4 6 7 As such, evidence for the value of cognitive function as an individual predictive marker of ProPD remains limited.3 A recent study reported that a higher probability of ProPD was associated with lower cognitive performance in a Greek cohort.8 Although informative, probability scores do not differentiate specific prodromal features, and olfactory loss, a marker of PD and cognitive decline, was not assessed in this study. Further, previous studies have primarily focused on objective measures of cognitive performance and little is known about subjective cognitive performance in the course of PD.9 Tests of objective measures have limited clinical applicability in the general population and studying subjective cognition might therefore be useful for screening of large populations.
Here, we present the first investigation of objective and subjective cognitive performance among men with and without non-motor features of ProPD. More specifically, we describe how experiencing combinations of hyposmia, constipation and probable REM sleep behaviour disorder (pRBD), common non-motor features of ProPD, are related to objective and subjective measures of cognitive function.
Methods
Population
This study was conducted in the Health Professionals Follow-up Study (HPFS), a cohort of 51 529 male health professionals (including dentists, pharmacists, optometrists, osteopath physicians, podiatrists and veterinarians) who were recruited in 1986 and have been actively followed over time for the incidence of numerous health-related conditions, such as cancer, heart disease and PD. In 2012, we started an investigation of ProPD among participants in this cohort (HPFS-ProPD). As part of this investigation, all HPFS participants were asked about bowel movement frequency, use of laxatives and pRBD in 2012. Then, in 2014, a subset of 6479 men without PD (including 4172 with either pRBD or constipation, and 2307 without pRBD or constipation) and 120 PD cases completed an olfactory test and supplementary questionnaire to update constipation and pRBD.
Assessment of non-motor features of PD
Olfaction was assessed using the Brief Smell Identification Test, a standardised, self-administered forced choice test consisting of a booklet containing 12 odorants; participants are asked to identify each odorant from a list of four alternatives.10 Each participant’s olfactory score was calculated by summing the number of correctly identified odours, and hyposmia was defined as an olfactory score in the bottom 10% of individuals who screened negative for pRBD and constipation (score ≤7). Constipation was defined as a bowel movement every other day or less frequently, and/or laxative use at least weekly. To assess pRBD, we used an RBD screening question that investigated dream enactment behaviour and violent or excessive movement during sleep (‘Has your spouse [or sleep partner] told you that you appear to ‘act out your dreams’ while sleeping [punched or flailed arms in the air, shouted or screamed], which has occurred at least three times?’, adapted from the validated Mayo Sleep Questionnaire.11 This question, but without the specification of dream enactment having occurred at least three times, has been reported to have a high sensitivity specificity (100% and 95%, respectively) for the diagnosis of polysomnography-confirmed RBD in a community-based sample.11
Telephone cognitive interviews
In 2016–2017, a telephone-based cognitive assessment was administered to a subset of the 6599 HPFS-ProPD participants. All men with hyposmia in the HPFS-ProPD substudy (1180 men), and a random sample of 197 PD-free men without hyposmia, pRBD, or constipation from the substudy were invited to participate in the cognitive interviews. Because having multiple prodromal features is strongly associated with PD in this cohort,12 the combination of selection into the ProPD substudy, based on constipation and pRBD, and then into the cognitive interview group, based on hyposmia, was designed to purposefully select men with key prodromal features who were most likely to be in the prodromal phase of PD. The telephone-based cognitive assessment was completed by 693 individuals with hyposmia (59% of those eligible), of whom 46 had confirmed PD, and 125 without hyposmia (63% of those eligible). Overall, characteristics were similar between responders and non-responders, but non-responders appeared to be more obese and less physically active (table 1). Fourteen responders with a history of stroke were excluded, resulting in a final sample size of 804.
Age-adjusted characteristics of all participants selected for cognitive testing according to response status
Trained interviewers who were unaware of the study hypothesis and of participants’ disease status completed the telephone-based cognitive assessments. The interview included the following cognitive tests: Telephone Interview for Cognitive Status (TICS),13 delayed recall of the TICS 10-word list, East Boston Memory Test (immediate and delayed recall),14 animal naming test of verbal fluency,15 the digit span backward test16 and the Oral Trail Making Test A and B.17 This assessment has been previously used among HPFS participants.18 A correlation of 0.81 was found when comparing the global score from the telephone-administered interview to the global score from an in-person interview.19 Further description of these tests is provided in online supplemental table 1.
Supplemental material
A list of seven yes/no questions was included at the beginning of the interview to assess subjective cognitive decline (SCD).20 These seven items enquire about recent change in memory and a recent change in ability to: remember recent events; remember a short list of items; remember things from one second to the next; understand or follow spoken instructions; follow a group conversation or plot of a television programme; and find one’s way on familiar streets.
Ascertainment of PD cases
Our procedure for identifying PD cases has been previously described.21 Briefly, PD cases are initially identified via biennial self-report questionnaires sent to the entire HPFS cohort in which participants are asked to report new disease diagnoses. The self-reports are then validated by a medical record review conducted by a neurologist specialising in movement disorders. Cases are confirmed if the medical record included either a final diagnosis of PD by a neurologist, or evidence of at least two of the three cardinal signs (rest tremor, rigidity, bradykinesia) in the absence of features suggesting other diagnoses.
Statistical analysis
To evaluate objective cognitive function, scores for each cognitive test were reversed, if needed, so that higher scores would indicate better performance, and then converted to z-scores, defined as the difference between the participant’s score on that test and the mean score among all participants, divided by the SD. Our primary outcome was a global score of cognitive function calculated by averaging the z-scores for all tests. An additional measure of global cognition was based on the TICS. Domain scores were also created by averaging z-scores for all tests pertaining to a specific cognitive domain; attention and language were assessed by using a single test (online supplemental table 1). Due to the nature of our cognitive interview, we were unable to assess visuospatial function. To identify groups with or without relative cognitive impairment, dichotomised variables were calculated based on a score more than 1 SD below the group standardised mean, within the range recommended to identify mild cognitive impairment in PD.5 22 For the TICS, an established cut-off score of less than 31 points was used to define relative cognitive impairment.23
An SCD score was created by giving 1 point for every ‘yes’ answer and then categorised as ‘good’ (0 points), ‘moderate’ (1–3 points) and ‘poor’ (4–7 points), based on the distribution in the study population.
The following six distinct groups were defined for comparison: (1) individuals with no signs of ProPD, (2) individuals with hyposmia only, (3) individuals with hyposmia and pRBD (no constipation), (4) individuals with hyposmia and constipation (no pRBD), (5) individuals with hyposmia, pRBD and constipation and (6) individuals with confirmed PD. Group 1 was used as reference.12
In our analyses, we considered the following potential confounding variables: age at time of assessment (years, continuous); physical activity (metabolic equivalent-hour/week, quartiles); body mass index (normal weight <25 kg/m2, overweight 25 to <30 kg/m2 and obese ≥30 kg/m2); smoking status (never, ever, unknown); alcohol consumption (g/day, continuous); and coffee consumption (servings/day, continuous). Information on these variables was obtained from the most recent HPFS questionnaire at the time of analysis (2010 and 2012). Depressive symptoms (Mental Health Inventory24 score in the bottom 10% of the study population; score ≤21), assessed in the 2014 supplementary questionnaire, were considered in models of SCD. Analyses were not adjusted for education as participants were all health professionals with postgraduate educations and 94% of them reported having a doctorate-level degree in the cognitive interview.
For analyses of objective cognitive function, age-adjusted and multivariate-adjusted linear regression models were used to estimate mean z-score differences and 95% CI in global and domain-specific scores between the comparison groups. Logistic regression models were used to estimate age-adjusted and multivariate-adjusted ORs and 95% CI of cognitive impairment.
For analyses of subjective cognitive performance, age-adjusted and multivariate-adjusted Poisson regression models were used to assess the SCD score as a count variable. Overdispersion was accounted for by scaling the deviance parameter. Age-adjusted and multivariate-adjusted multinomial logistic regression were used to further estimate the relative odds for moderate and poor subjective cognition versus good subjective cognition.
All participants provided informed consent. Statistical analyses were performed in SAS V.9.4 (SAS Institute). P values were considered significant at the alpha <0.05 level.
Results
Age-adjusted characteristics of participants according to PD status are presented in table 2. Depressive symptoms were more prevalent in men with co-occurring constipation, pRBD and hyposmia and in those with confirmed PD; men in these categories were also less physically active.
Age-adjusted characteristics of the study population (n=804) according to presence of prodromal features and confirmed PD
Objective cognitive function
Men in all groups defined by the presence of prodromal features had significantly lower global cognitive mean z-scores than those in the reference group in multivariable-adjusted analyses (figure 1); mean score differences indicating worse cognitive performance were particularly pronounced among men with co-occurring constipation, pRBD and hyposmia (z-score difference=−0.46; 95% CI −0.70 to –0.23) and those with confirmed PD (z-score difference=−0.81; 95% CI −1.15 to –0.47). For the TICS (figure 1), mean score differences were statistically significant for participants with hyposmia and constipation (z-score difference=−0.26; 95% CI −0.48 to –0.03), constipation, pRBD and hyposmia (z-score difference=−0.29; 95% CI −0.52 to –0.05) and those with confirmed PD (z-score difference=−0.75; 95% CI −1.03 to –0.43). When we looked at differences in specific domains (figure 1), we found that performance was worse in men with constipation, pRBD and hyposmia and those with confirmed PD, particularly with respect language/verbal fluency but also for memory and executive function. In contrast, men with only hyposmia performed significantly worse on the memory score exclusively. Results for specific cognitive tests are provided in online supplemental table 2. As expected, individuals with PD had worse cognitive scores for all tests (online supplemental table 1). The results of analyses modelling the odds of cognitive impairment were consistent with those above. Using men without prodromal features as reference, the OR for cognitive impairment increased with the number of prodromal features and was highest for men with diagnosed PD (table 3). In analyses of the individual cognitive domains (table 3), having only hyposmia was significantly associated with memory impairment; having hyposmia and either constipation or pRBD but not both was significantly associated with language domain impairment; having hyposmia, constipation, and pRBD was significantly associated with impaired memory, executive function, and language; and having confirmed PD was associated with impaired executive function and language.
Adjusted ORs of relative cognitive impairment according to presence of prodromal features and confirmed PD

Multivariate-adjusted cognitive score differences and 95% CI according to presence of prodromal features and confirmed Parkinson’s disease (PD). pRBD, probable REM sleep behaviour disorder; TICS, Telephone Interview for Cognitive Status.
Subjective cognitive decline
Of the subjective cognitive complaints we assessed, the most common cognitive concern was having experienced a change in ability to remember things (47.2%) and the least common concern was having experience trouble finding one’s way around familiar streets (5.4%). Among study participants, 32.5% reported no cognitive concerns (good subjective cognition), 54.6% reported 1–3 concerns (moderate subjective cognition), and 13.0% reported ≥4 concerns (poor subjective cognition).
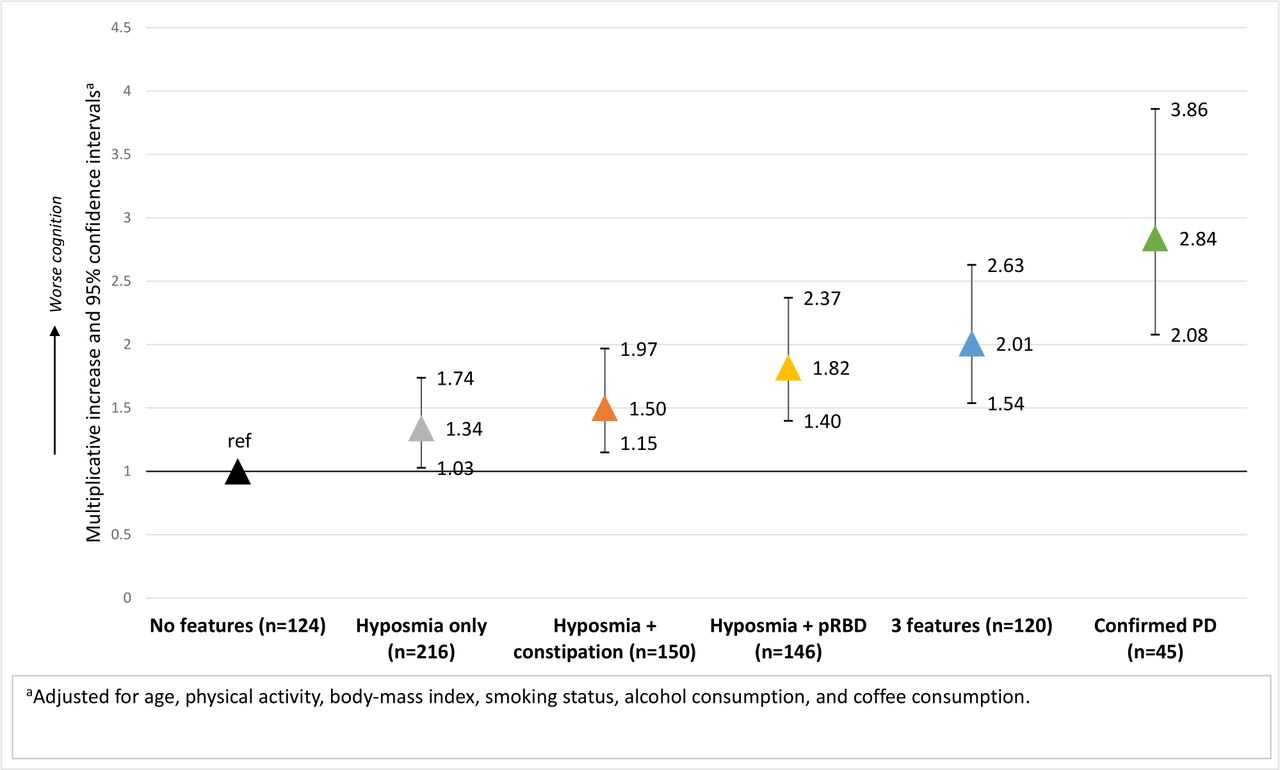
In multivariate Poisson regression models, we found that men with only hyposmia, hyposmia and either constipation or pRBD, men with all three features, and men with confirmed PD had significantly worse SCD scores compared with those with no PD features (figure 2). As in the analyses of objective cognition, the difference in mean SCD scores were greatest in men with co-occurring constipation, pRBD, and hyposmia and in those with confirmed PD, compared with those with no features. Consistent results were obtained in multinomial logistic regression models of subjective cognitive performance (table 4). The odds of poor as compared with good subjective cognition were significantly higher for all hyposmic individuals with at least one additional prodromal feature and men with confirmed PD. Exploratory analysis suggested that this association could be driven by the items corresponding to perceived change in ability to remember recent events, follow a group conversation and find one’s way on familiar streets (online supplemental table 3). Adjusting for depressive symptoms did not change the results in either linear or logistic regression models (table 4).
Adjusted ORs of subjective cognition categories according to presence of prodromal features and confirmed PD
{kind=link}
{kind=link}
Multivariate-adjusted multiplicative increase in the mean subjective cognitive decline score and 95% CI according to presence of prodromal features and confirmed Parkinson’s disease (PD) (n=801). pRBD, probable REM sleep behaviour disorder
Discussion
In this cross-sectional study of men from the HPFS-ProPD study, we found that individuals with non-motor features suggestive of ProPD had worse global cognitive performance than men without these signs. Impairment was particularly pronounced for those with concurrent hyposmia, pRBD and constipation, who are at higher risk of PD. In addition, hyposmic individuals without other prodromal features performed worse on memory tests, whereas individuals with at least one feature in addition to hyposmia were particularly affected in language/verbal fluency, and, to a lesser extent, in executive function and memory. Hyposmia combined with at least one additional sign was associated with higher odds of poor SCD. Finally, as expected, individuals with confirmed PD performed worse than the rest of the groups in both objective and subjective assessments.
The results of our objective cognitive function analyses provide important insight to further characterise cognitive function in ProPD and its relationship with constipation, pRBD, and hyposmia, key non-motor features of ProPD. A recent population-based study in Greece found that higher probability of ProPD was associated with lower cognitive performance in all cognitive domains, and higher probability of mild cognitive impairment.8 Another prospective study of 468 participants in Germany showed that future PD converters had lower global cognition scores compared with non-converters years before clinical diagnosis.25 Similarly, in a case–control study nested in the Rotterdam Study, a subtle decline in executive cognitive functions was found to be present up to 7 years before PD diagnosis26 and an association between poor cognitive functioning and increased risk of incident parkinsonism, including probable PD, was confirmed in a longitudinal analysis of the same cohort.6 Our study builds on these findings by describing the relationship between specific non-motor features of ProPD with poor cognitive function. Similar to our study, results from the PARS study showed that cognitive performance on global cognition, executive function and memory was worse in individuals who were free of PD but had hyposmia and impaired dopamine transporter binding reduction (important predictors of PD).7 Results from the same study found that individuals who converted to PD during follow-up, had worse cognitive function at baseline compared with non-converters.27 Results from the Tübinger Evaluation of Risk Factors for Early Detection of Neurodegeneration (TREND) study showed that self-reported forgetfulness and word-finding difficulty were more common in individuals with hyposmia and RBD.28 Our study expands on these studies by assessing hyposmia, RBD and constipation in the same population and exploring their co-occurrence. In sum, the observations of these studies are consistent with our findings; global cognitive dysfunction or impairment in one of several cognitive domains may be a sign of ProPD when occurring in the presence of other relevant non-motor features. Our study addressed some of the limitations of these previous studies by using more extensive measures of cognitive function and robustly assessing some of the most common non-motor ProPD features individually and in combination.
Our subjective cognitive performance results are consistent with those based on objective cognitive assessments and with the few studies that have subjectively assessed cognition in ProPD. A previous nested case–control study evaluated SCD in ProPD and found that patients with PD started reporting memory complaints 1.5 years before diagnosis.26 Another study using a primary care database found that memory problems reported by a clinician were more common in patients with PD compared with those without PD at 2 years before diagnosis.29 Using a more detailed assessment of current functional abilities, we provide further evidence that SCD might be present in individuals with features suggestive of ProPD, particularly in individuals with concurrent hyposmia, constipation and pRBD. Our results are also in line with previous studies on cognitive function in patients with PD. Robust evidence indicates that, in comparison with age-matched groups without PD, individuals with PD exhibit more rapid decline in many cognitive domains; these are particularly pronounced in the executive, attentional and visuospatial domains, and, to a lesser extent, memory.9 In addition, olfactory dysfunction in patients with PD has been associated with cognitive impairment30 and dementia conversion.31 Because all participants with confirmed PD in our investigation were hyposmic, we could not determine whether hyposmia in PD is associated with more severe cognitive impairment.
Olfactory dysfunction and cognitive impairment are common features not only of ProPD but also of early Alzheimer disease (AD)32 and diffuse Lewy body disease (DLB)33; hyposmic individuals in our study might therefore be at higher risk of cognitive decline and it is possible that some of them may develop AD or DLB. The combination of hyposmia, constipation and pRBD, however, has been strongly associated with PD in this cohort,12 which suggests that men with these features are more likely to be in the prodromal phase of PD rather than AD. In addition, a few studies have suggested a link between cognitive impairment in RBD and the subsequent development of PD or DLB.34 35 RBD patients with cognitive impairment are more likely to exhibit non-amnestic cognitive impairment rather than an amnesic phenotype, which seems to be more typical in AD.36 Therefore, since DLB is notably less common than PD,37 the presence of additional prodromal features such as RBD in hyposmic individuals and the specific nature of their cognitive impairment might help to differentiate those who will potentially develop AD from those who will potentially develop PD.
The evolution and heterogeneity of cognitive impairment in PD mirrors the complexity of the disease process.38 39 In addition to α-synuclein, tau and amyloid pathologies, many other mechanisms are likely to contribute to cognitive decline, including different neurotransmitter systems, early synaptic changes, inflammation and mitochondrial dysfunction.9 The roles of these and other potentially relevant mechanisms need to be explored further.
Limitations of the current analysis should be considered. First, results reported here are cross-sectional; prospective follow-up of our cohort will be necessary to better characterise the role of cognitive performance in predicting conversion to PD and the development of further cognitive decline, particularly in individuals with additional prodromal features. Second, due to the observational nature of the investigation and use of questionnaires (and/or cognitive test batteries), it is possible that unmeasured or residual confounding and measurement error may be biasing our results. For instance, the performance of individuals with diagnosed PD could have been affected by PD medications, and our assessment of the language domain was based on a single test which may also capture elements of executive function and processing speed. Third, the average age of our cohort at assessment for prodromal features was somewhat older than the average age of onset of PD, and our study was conducted among a homogeneous, mostly white male population of health professionals, which could affect the generalisability of the results. Finally, the response rate for the cognitive interviews was relatively low in both hyposmic and non-hyposmic individuals. However, characteristics between responders and non-responders were similar, indicating that non-response likely caused minimal bias in the results.
Strengths of our study are its population-based design and the assessment of multiple prodromal features of PD and their co-occurrence. In addition, potential confounders were robustly assessed, which allowed for careful control of confounding, and well-validated instruments were used to assess both objective and a subjective cognitive performance. The consistency of the results obtained suggests that SCD might have a role in screening of large populations due to its simplicity, low cost and short application time. Considerable evidence demonstrates that SCD predicts future cognitive decline in the general population,40 so it might be a harbinger of further cognitive decline in PD.
In conclusion, our study suggests that cognitive impairment is common in individuals with hyposmia, particularly when additional non-motor features of PD, such as constipation and pRBD, are present. The prognostic significance of both subjective and objective measures of cognitive performance and their utility in clinical practice will be determined through longitudinal follow-up currently underway.
Data availability statement
Data are available on reasonable request. Data, methods and materials used to conduct this research article were carefully documented. Data will be shared at the request of other investigators for purposes of replicating procedures and results.
Ethics statements
Ethics approval
This study was approved by the Human Research Committee at the Brigham and Women’s Hospital and Harvard T. H. Chan School of Public Health.
Acknowledgments
The authors would like to thank participants of the Health Professionals Follow-up Study for their participation. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Research project. Conception: AA, XG, JHK and MS. Organisation: KCH, SM, XG, JHK, MS and AA. Execution: KCH, SM, XG, JHK, MS and AA. Statistical analysis. Design: MF and AA. Execution: MF. Review and Critique: MF, KCH, SM, XG, JHK, MS and AA. Manuscript preparation. Writing of the first draft: MF. Review and critique: MF, KCH, SM, XG, JHK, MS and AA.
Funding This study was supported by Department of Defense grant W81XWH-14-0131 (PI: AA). The HPFS cohort is funded by NIH grant UM1 CA167552.
Competing interests MF received a scholarship from Fundación México en Harvard, A. C; KCH reports no disclosures; SM reports no disclosures; XG received research grants from the National Institutes of Health, outside of this work; AA received a research grant from the Department of Defense related to this work. He has also received research grants from the National Institutes of Health, the Michael J. Fox Foundation, and the National Multiple Sclerosis Society, outside of this work; MS served on the scientific advisory board for CBD Solutions (foundation), has served as a consultant for New Beta Innovation (company) and Harvard University, and is funded by NIH grants NS090259, NS098746, U13NS103523, Department of Defense W81XWH-11-1-0150, the Michael J. Fox Foundation, the Parkinson’s Alliance, the Parkinson’s Foundation, Target ALS Foundation; JHK has received research grants from the National Institutes of Health outside of this work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.