Article Text

Abstract
Background In acute ischaemic stroke, endovascular thrombectomy (ET) significantly reduces disability compared with thrombolytic therapy, but access to ET is currently limited. Leveraging telerobotic technology to disseminate neurosurgical expertise could increase access to ET. This proof-of-concept evaluation was performed to determine whether remote robotic ET (RRET), wherein an offsite neurosurgeon and an onsite interventional cardiologist collaboratively use telerobotics to perform ET, is technically feasible.
Methods An ex vivo model of RRET was constructed by establishing a network connection between a robotic drive in a simulation laboratory and a robotic control unit 5 miles away. Using onsite assistance from an interventional cardiologist in the simulation laboratory, an offsite neurosurgeon used the robotic controls to attempt RRET on a fluid-filled silicone model of human vasculature containing simulated thrombus material in the left middle cerebral artery (MCA).
Results From the offsite location 5 miles away, the neurosurgeon used the robotic system to successfully navigate a guidewire from the carotid artery to simulated thrombus in the MCA. Under the direction of the neurosurgeon, the onsite interventional cardiologist then successfully manually advanced an aspiration catheter over the guidewire to the thrombus, removed the guidewire and performed aspiration.
Conclusions In this proof-of-concept evaluation, the technical feasibility of RRET was demonstrated in an ex vivo model and was collaboratively performed by an offsite neurosurgeon and an onsite interventional cardiologist. This report supports the design of future studies to determine if RRET could be used to increase access to ET for patients with acute ischaemic stroke.
- stroke
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
For patients with acute ischaemic stroke due to large vessel occlusion, endovascular thrombectomy (ET) significantly reduces disability and mortality compared with conventional thrombolytic therapy.1 2 Despite these benefits, it is estimated almost half the US population cannot reach an ET-capable centre within 1 hour of stroke onset,3 which is problematic as thrombectomy delays associate with increased stroke-related disability.4 In contrast to the shortage of ET-capable centres, hospitals performing primary percutaneous coronary intervention (PCI) for ST-segment elevation myocardial infarction are more prevalent. Many primary PCI hospitals serve as hubs in regional networks of care that increase access to primary PCI across large geographic areas.5 6 Leveraging primary PCI hospitals to also perform ET would likely increase access to ET, but would require dissemination of neurosurgical expertise to less specialised hospitals. Disseminating neurosurgical expertise may be possible using telerobotics if an off-site neurosurgeon remotely controlled a robot at the PCI hospital to perform ET with the bedside assistance of an interventional cardiologist (IC) who is adept in obtaining vascular access and manipulating endovascular devices. We conducted this proof-of-concept preclinical evaluation to determine whether remote robotic ET (RRET) collaboratively performed by an offsite neurosurgeon and an onsite IC is technically feasible.
Materials and methods
An ex vivo model of RRET was constructed using a robotic drive (CorPath GRX, Corindus, A Siemens Healthineers Company, Waltham, Massachusetts, USA) in a cardiovascular simulation laboratory (figure 1) and a robotic control unit in an office building approximately 5 miles away (figure 2). The robotic drive and control unit were connected over a virtual private network with hardware firewalls to secure and isolate device data within the network. The robotic drive was positioned adjacent to a fluid-filled ex vivo silicone model of human vasculature (United Biologics, Santa Ana, California, USA) with simulated thrombus material in the M2 segment of the left middle cerebral artery (MCA). A camera positioned over the silicone model captured live video to simulate fluoroscopy which was displayed on a bedside monitor and simultaneously transmitted over the network to a monitor in the office building.
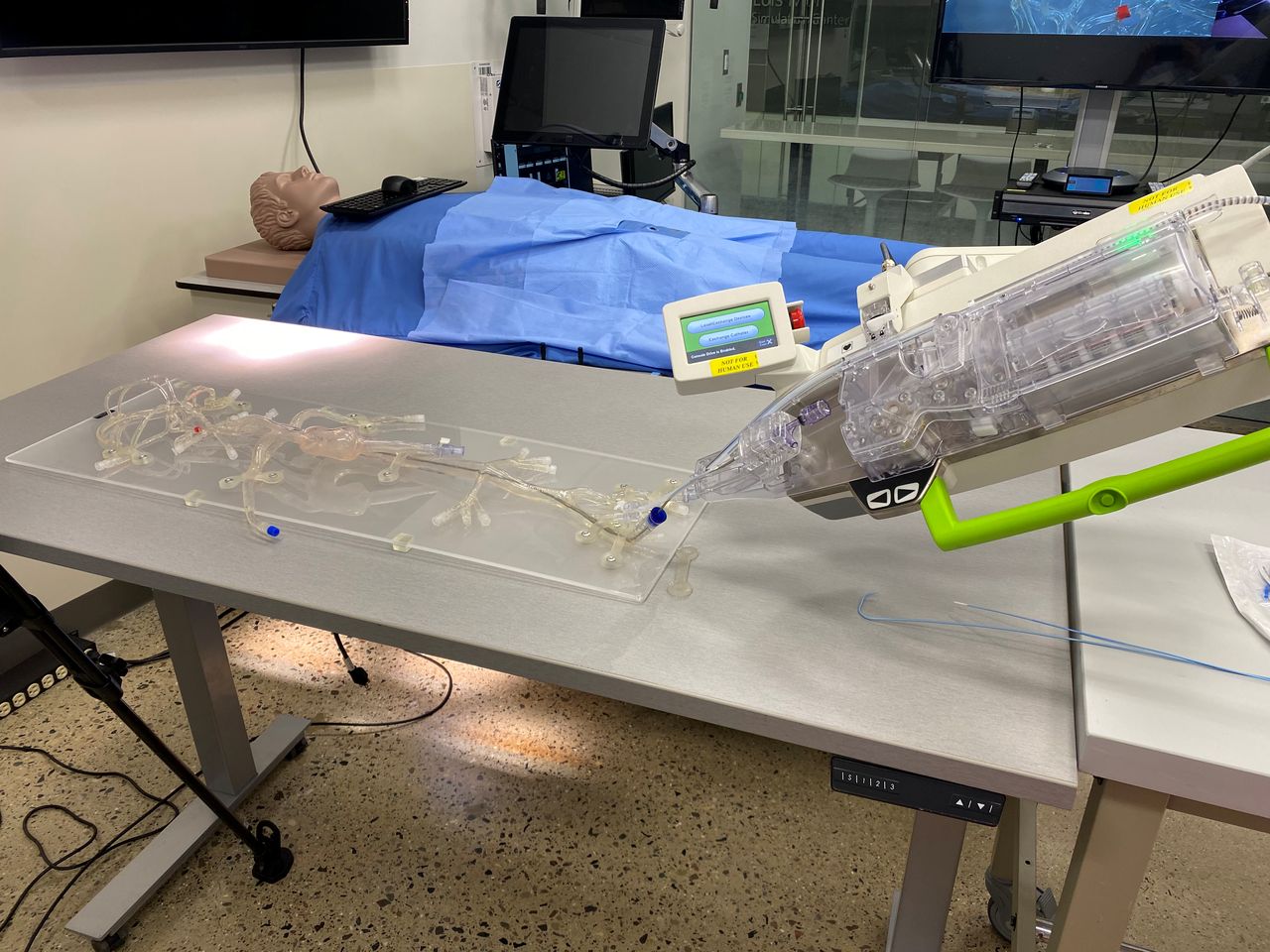
Cardiovascular simulation centre in ex vivo model of RRET. Shown is the cardiovascular simulation centre which housed the model of silicone vasculature (left), robotic drive (right) and interventional cardiologist (not shown). The mannequin seen in the background of the image was not used in this study. RRET, remote robotic endovascular thrombectomy.

{kind=link}
{kind=link}
Offsite robotic control unit shown is the robotic control unit located in an office building approximately 5 miles away from the cardiovascular simulation laboratory. The monitor on the left displayed live video transmitted from the simulation laboratory and was intended to simulate fluoroscopy. In this image, the neurosurgeon is using the controls to telerobotically advance a wire from the carotid artery to the location of thrombus in the middle cerebral artery in the silicone model 5 miles away. MCA, middle cerebral artery; RRET, remote robotic endovascular thrombectomy
A neurosurgeon was seated at the robotic controls in the office building and an IC was bedside in the simulation laboratory. In all attempted procedures, the IC manually advanced an 8 Fr x 90 cm sheath (AXS Infinity LS, Stryker Neurovascular, Fremont, California, USA) from the right femoral artery to the left carotid artery and an 0.014 inch × 300 cm guidewire (Synchro2 Support, Stryker Neurovascular, Fremont, California, USA) to the tip of the sheath. The IC loaded the guidewire into the robotic drive. All subsequent movements of the guidewire were performed robotically by the offsite neurosurgeon. Three variant methods of performing RRET were attempted: (1) RRET—aspiration. The neurosurgeon robotically navigated the guidewire and the IC manually advanced a 6 Fr aspiration catheter (AXS Catalyst 6, Stryker Neurovascular, Fremont, California) to the MCA thrombus; (2) RRET—stent retriever. The neurosurgeon robotically navigated the guidewire and a 2.7 Fr microcatheter (Trevo Trak21, Stryker Neurovascular, Fremont, California USA) to the MCA thrombus and the IC manually delivered and subsequently retrieved a 4.0×41 mm stent (Trevo NXT, Stryker Neurovascular, Fremont, California, USA); and (3) RRET—stent retriever and aspiration. The neurosurgeon robotically navigated the guidewire to the MCA thrombus and the IC manually delivered a 6 Fr aspiration catheter (AXS Catalyst 6, Stryker Neurovascular), a 2.7 Fr microcatheter (Trevo Trak21, Stryker Neurovascular), and a 4.0×41 mm stent (Trevo NXT, Stryker Neurovascular). The IC subsequently retrieved the stent while aspiration was simultaneously performed. The main outcome was technical feasibility, defined by the successful completion of the above procedural steps.
Results
On 19 November 2020, RRET was attempted in the ex vivo model. In all three variations, the neurosurgeon successfully used the robotic system to advance a guidewire from the carotid artery to the MCA. RRET—aspiration: After the neurosurgeon robotically delivered the guidewire, the IC manually advanced an aspiration catheter over the guidewire to the thrombus and performed manual aspiration (online supplemental video 1). RRET—stent retriever: The neurosurgeon robotically delivered both the guidewire and microcatheter to the target location in the MCA. The IC then manually advanced a stent through the microcatheter, unsheathed the stent at the site of thrombus, and subsequently retrieved the stent (online supplemental video 2). RRET—stent retriever and aspiration: After the neurosurgeon robotically delivered the guidewire, the IC manually delivered an aspiration catheter, microcatheter, and stent to the target site in the MCA and then manually retrieved the stent while aspiration was simultaneously performed (online supplemental video 3). Thus, technical feasibility was demonstrated in all three methodological variations of RRET.
Supplementary video
Supplementary video
Supplementary video
Discussion
To our knowledge, this proof-of-concept evaluation is the first to demonstrate the technical feasibility of RRET and was demonstrated in three procedural variants of RRET using aspiration, a stent retriever or both. Differing in the number of procedural steps performed by the onsite IC, none of the three approaches requires the IC to independently navigate a guidewire through the intracranial vessels, which would require an in-depth understanding of neurovascular anatomy, but rather only to manually advance interventional devices over a stationary guidewire already positioned in the desired anatomic location by the offsite neurosurgeon. Although most experienced IC likely possess sufficient skills to deliver endovascular devices over a stationary wire to a target location, further advancements in robotic technology will enable the neurosurgeon to perform more of the procedural steps required for RRET than is currently possible with the contemporary robotic system.
In this study, the technically feasible of RRET was demonstrated over a distance of 5 miles. Performing RRET over longer distances would be required to increase access to ET for stroke patients. Notably, telerobotic technology has been used to successfully perform PCI in vivo in animals and in humans over distances of 100 miles and 20 miles, respectively.7 8 Furthermore, the robotic system used in this study has been successfully operated over distances>3000 miles without perceptible latencies to the operating physician.9 These results suggest RRET may be similarly feasible over vast distances.
Finally, it should be noted that the current generation robotic system does not provide the operator with tactile feedback. Despite this limitation, the robotic system has been used to perform PCI with high technical and clinical success, even among complex interventions, without tactile feedback.10 It is possible that future generation robotic systems may be developed to provide detailed information regarding tactile forces present at the tip of endovascular devices that are well below the level of perception by humans.
Conclusions
In this proof-of-concept evaluation, the technical feasibility of RRET was demonstrated in an ex vivo model and was collaboratively performed by an offsite neurosurgeon and an onsite IC. This report supports the design of future in vivo studies to determine if RRET could be used to increase access to ET for patients with acute ischaemic stroke and thereby address the current shortage thrombectomy-capable centres.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @RyanMadderMD
Contributors All three authors of this manuscript made substantial contributions to the conception and design of the work. All three authors were involved with the acquisition, analysis and interpretation of data. RM drafted the work. JS and SV revised the manuscript critically for important intellectual content. All three authors gave final approval of the version published. All three authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This study was funded by the Frederik Meijer Heart & Vascular Institute. Material support for this study was provided in part by Stryker Neurovascular.
Competing interests JS: consulting fees, proctoring fees and speaker honoraria Stryker, proctoring fees Medtronic, speaker honoraria Ceronovus, speaker honoraria Penumbra, and educational fees Nico. RM: research support, speaker honoraria and consulting fees Corindus, A Siemens Healthineers Company.
Provenance and peer review Not commissioned; externally peer reviewed.