Article Text

Abstract
Background Subacute sclerosing panencephalitis is a progressive neurodegenerative disorder caused by a latent and mutant measles virus which is extremely rare in developed countries. The lack of effective treatments leads to the research of other anti-inflammatory and neuroprotective treatments.
Case Here we present a case of a 17-year-old patient affected by subacute sclerosing panencephalitis who manifest a dramatic improvement in neurological and general clinical conditions, as well as an arrest in the progression of demyelinating process in the central nervous system, after the beginning of a high ratio ketogenic diet.
Conclusions Given its anti-inflammatory, antioxidant and metabolic effects, we believe that ketogenic diet utilisation could be a rational approach, can be considered a safe add-on therapy, carrying on with only a minimal risk of adverse effects or interactions.
- clinical neurology
- infectious diseases
- MR
Data availability statement
The data that support the findings of this short report are available on request from the corresponding author (IDN).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Subacute sclerosing panencephalitis (SSPE) is a progressive neurodegenerative disorder, occurring with a median latency of 9.5 years after measles infection and causing widespread demyelination of the central nervous system.1
SSPE are expected in 4–11 cases for every 100 000 cases of measles, increasing to 18 for every 100 000 cases if infection occurs in early childhood.2 In Italy, during 2017–2018, 8078 new cases of measles infection were ascertained, 1627 more in 2019.3
Although vaccination prevents SSPE and 30%–35% of patients may benefit from therapy4–6 in terms of slower progression, prolonged survival or clinical improvement,1 currently there is no definitive cure. Hence the need of further therapeutic options.
We report a case of SSPE, with typical electroencephalogram (EEG) and magnetic resonance (MR) patterns,7 8 treated with a ketogenic diet (KD) associated with antiviral medications and neurostimulation.
Case description
Clinical features
A 17-year-old girl experienced two loss of consciousness in September 2019, followed by progressive mood changes, irritability and a decline in her academic performance. In December 2019, she developed involuntary jerks in her upper limbs, widespread stiffness with abnormal limb postures, progressive decline in functional abilities, with the need of assistance to get dressed and climb stairs. She soon developed daily crying jags and insomnia. Her menstrual cycle was altered and amenorrhoea occurred.
Following this, she experienced a rapid decrease of visual acuity and was no longer able to read. At our first evaluation, in January 2020, we observed cognitive slowing, speech impoverishment, motor impairment and gait unsteadiness. She needed help when walking and changing position. Spasticity of the upper limbs, more severe in the right arm, cervical dystonia and dystonic posturing of right limb were present. Myoclonic jerks involving arms, especially the right one, occurred at regular intervals.
Laboratory analyses and neurophysiological assessment
Oligoclonal bands type III on cerebrospinal fluid (CSF) and increased anti-measles IgG antibody titre in CSF (10 589 UI) and serum (22 038 UI), were found. PCR for measles was negative in CSF, serum and nasopharyngeal swab.
The mother revealed that the patient had contracted measles infection at 2 months old, before the age of mandatory vaccination.
The EEG showed the characteristic periodic Radermecker complexes, in 1:1 relation with the myoclonic jerks. During sleep, Radermecker complexes were always present, but the associated jerks disappeared.
MRI
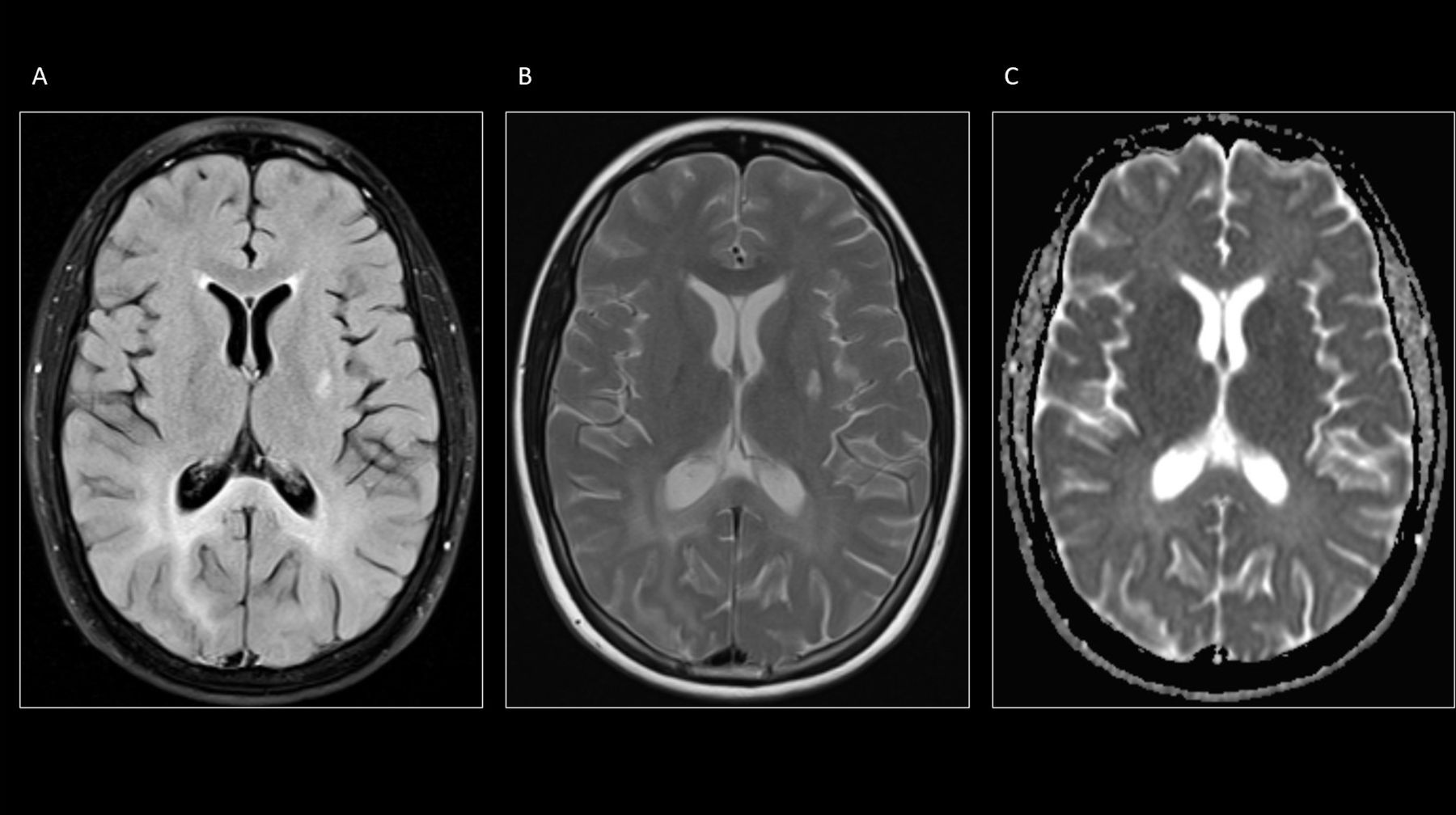
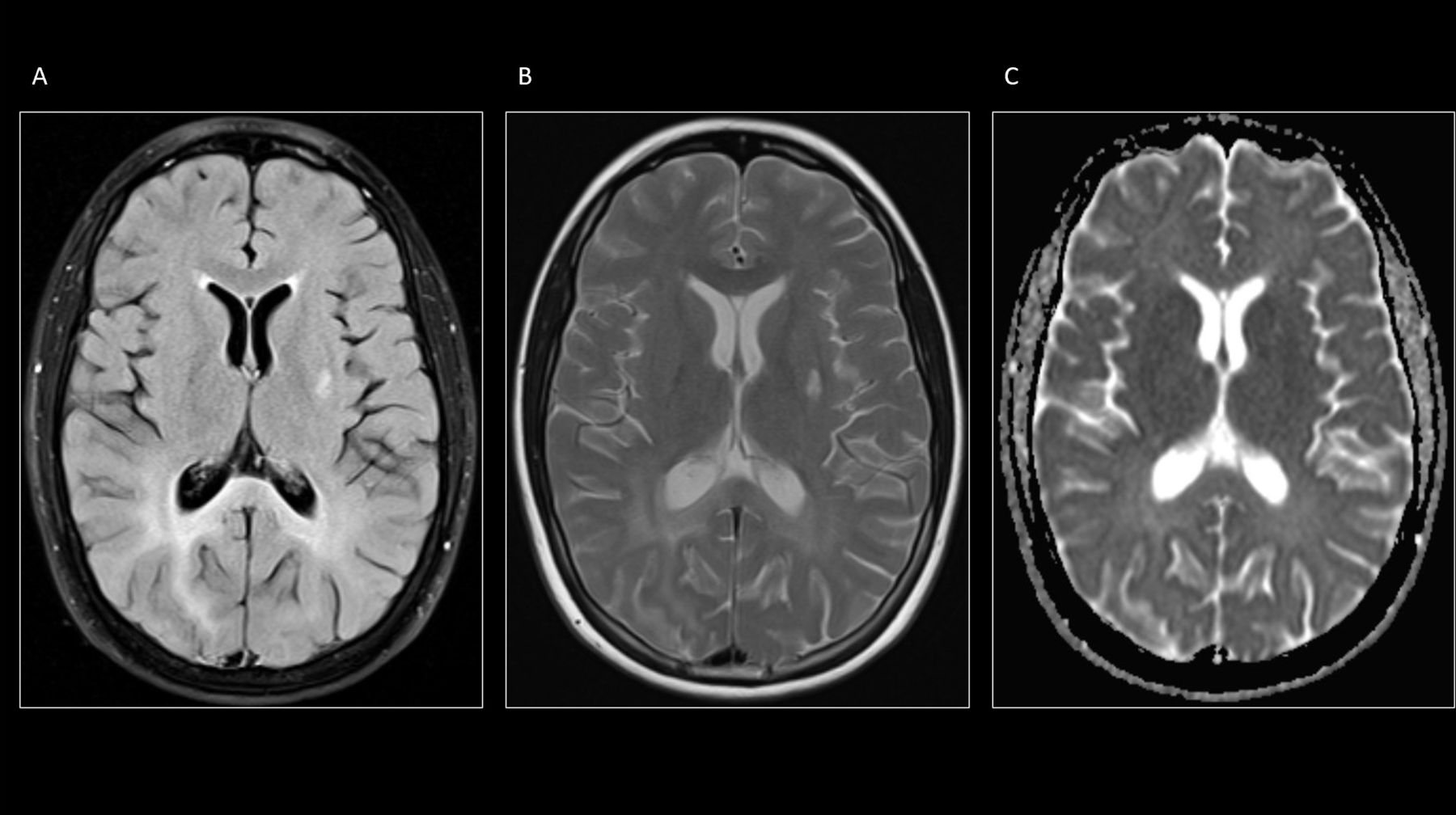
The patient underwent a brain MR examination with a 1.5-Tesla system, which revealed the presence of T2-weighted and fluid-attenuated inversion recovery (FLAIR) asymmetrical, confluent white matter hyperintensities (figure 1A,B) with high signal on apparent diffusion coefficient (ADC) maps of diffusion-weighted images sequence (figure 1C) involving both parietal lobes and the splenium of corpus callosum. A focal lesion characterised by diffusion restriction was detected in the left putamen. No contrast enhancement was seen. Magnetic resonance spectroscopy in the white matter of the right parietal lobe showed decreased N-acetyl-aspartate (NAA) with substantially normal Choline/Creatine (Cho/Cr) ratio.
{kind=link}
A-C show typical confluent and asymmetrical white matter hyperintensities on fluid-attenuated inversion recovery (FLAIR) (A) and turbo spin-echo-T2-weighted (TSE-T2W) (B) involving both parietal lobes with prevalence on the right side. The splenium of the corpus callosum is also involved. On the apparent diffusion coefficient maps (C) there is no evidence of diffusion restriction of the white matter.
Based on clinical history, neurological examination, EEG, MR images and anti-measles IgG antibody titres, the patient was diagnosed with SSPE.9
Treatments
Symptomatic treatment of the myoclonic jerks was attempted with administration of piracetam, levetiracetam, valproate, clonazepam, lacosamide and lamotrigine, all without clear effects.
Beneficial, although transient, effect on the intensity of jerks was observed with repetitive transcranial magnetic stimulation.
Cervical dystonia was treated with three botulinum neurotoxin injection sessions, in association with pharmacological treatment with trihexyphenidyl.
Antiviral therapy with methisoprinol 3000 mg/die and ribavirin 800 mg/die was immediately started after diagnosis, without significant results.
Ketogenic diet
In absence of any clinical improvement, at the end of February 2020, a normocaloric 3:1 ketogenic diet was started, with rapid induction through fasting and subsequent switch to 4:1 ketogenic ratio after 1 month. All the administered drugs were in sugar-free formulation. At the end of April, medium chain triglyceride oil was added (30 mL/die). Thereafter, the patient achieved stable levels of capillary β-hydroxybutyrate (3.8–4.6 mmol/L).
Dietary treatment was well tolerated and no side effects were observed, except for reduction of 11 kg in body weight, before stabilisation. Although globally reduced, the myoclonic jerks became prevalent in the right arm.
In May, after three administrations of steroids for retinal angiography, blood ketone level decreased to 1.8 mmol/L, with severe worsening of motor and behavioural symptoms.
A month later, ketosis reached stable levels of 4.5–5 mmol/L, with progressive improvement of cognitive and motor functions.
Clinical follow-up
After 1 year, the myoclonic jerks are still present especially in the upper left limb and inferior right limb, but they appear reduced in amplitude and frequency. Dystonic posturing is no longer present.
The patient is now able to dress and wash herself, walk and climb stairs without aid. Cognitive performance has improved and she is now able to read, follow classes and use a smartphone and notebook. Irritability and crying jags are now infrequent. Sleep quality has improved, insomnia has disappeared and night arm stiffness has been reduced. Finally, a regular menstrual cycle has resumed.
MR follow-up
The patient underwent five additional MR examinations: basal and 21, 38, 69 and 219 days after the first observation.
In April 2020, a small focal lesion appeared in the right putaminal nucleus while the left putaminal lesion resulted more hyperintense in T2W and FLAIR sequences.
For each brain MR examination, we have also calculated an ADC ratio of the white matter of the right parietal lobe using the homolateral frontal horn of the lateral ventricle as internal reference, with the following results in the five consecutive MR sessions: 0.37 – 0.39 – 0.41 – 0.48 – 0.42.
Discussion
In SSPE, an altered cellular response results in virus silent persistence and later reactivation in the central nervous system. Perivascular infiltration of inflammatory cells, demyelination and oxidative damage are described in the earlier phases of the disease.4
Glutamate transport alteration and lipid peroxidation follow this stage, in which inflammation becomes less evident and cortical atrophy ensues, with neurofibrillary tangles of abnormally hyperphosphorylated tau protein accumulation and neuronal loss.1
Considering the pathogenesis of SSPE, KD utilisation could be a rational approach, given its anti-inflammatory, antioxidant and metabolic effects.10 KD also modulates glutamatergic neurotransmission.11
Two cases of SSPE treated with KD have been previously described. In the first, utilisation of a 4:1 KD regimen in a young boy resulted in the resolution of the myoclonic jerks after 2 weeks of treatment, lasting for 3 months, before loss of effect and disease progression.12
In the second, a 2:1 ketogenic diet, with an average 2.2 mmol/L blood ketone level, caused improvement in cognition and physical abilities after 1 month of diet and resolution of the myoclonic jerks after 11 months. Moreover, in this case a dramatic improvement in EEG pattern was reported.13
Neither of them has been studied with ADC ratio.
In our case, we observed global clinical improvement, stability of EEG pattern and progressive reduction of myoclonus and dystonia after the achievement of stable ketosis (June 2020).
While motor improvements could be attributed also to the other treatments, the arrest of SSPE progression is more reasonably due to the anti-inflammatory and neuroprotective action of KD.
The worsening of both motor and behavioural symptoms during the transient loss of ketosis, caused by steroids, supports the significant role of KD.
Even if 5%–6% of patients may experience spontaneous prolonged remission,6 14 we think that the use of KD may have modified the natural course of disease in this patient. Considering the complete ineffectiveness of methisoprinol and ribavirin before KD and contradictory and scarce data regarding their efficacy in literature,1 5 6 we believe that their role has been very limited.
The bilateral, asymmetrical confluent T2W and FLAIR hyperintensities involving the white matter of both parietal lobes, splenium of corpus callosum as well as the abnormalities in the basal ganglia regions are in accordance with previous observations.8 15 The NAA/Cho and NAA/Cr ratios observed in the white matter are consistent with a severe neuronal loss.8
While the new right putaminal lesion appeared before stable ketosis, the hyperintensities of the occipital bilateral white matter manifested a considerable slowing in progression in ADC ratio between the fourth (April 2020) and the fifth (September 2020) MR examination, which was the period of time when our patient achieved and maintained stable and high levels of blood ketones.
Conclusions
These days, SSPE is very rare in developed countries. Due to the lack of effective treatment, the disease usually progresses to death, occurring mostly within 3 years.14 To the best of our knowledge, this is the first case in whom the effects of KD have been extensively described from a clinical, neurophysiological and neuroradiological point of view.
While vaccination remains fundamental in SSPE prevention, a multimodal treatment approach may be considered.
Ketogenic diet can be considered a safe add-on therapy, carrying on with only a minimal risk of adverse effects or interactions.
A longer period of observation is necessary to confirm if effects of KD on neuroinflammation and neurodegeneration are able to modify the course of this devastating disease.
Data availability statement
The data that support the findings of this short report are available on request from the corresponding author (IDN).
Ethics statements
Acknowledgments
The authors thanks all the investigators, collaborators and physicians of the University Hospital of Udine who take part in the management of the patient.
The CARE Guidelines checklist was used when writing our report.
Footnotes
Contributors MV, IDN, RG and GLG were involved in the management of the patient and drafting the manuscript. DB carried out the neuroradiological study. AB, AN and CL contributed to neurophysiological follow-up. DP was involved in patient’s treatment decisions. MRP supervised the ketogenic diet. MV and GLG were responsible for the final revision of the text.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.