Article Text

Abstract
Background In the PARADIGMS Study, fingolimod demonstrated superior efficacy versus interferon (IFN) β-1a and comparable overall incidence of adverse events but slightly higher rate of serious adverse events in patients with paediatric-onset multiple sclerosis (PoMS). Here, we report the health-related quality of life (HRQoL) outcomes from PARADIGMS.
Methods Patients with PoMS (N=215; aged 10–<18 years) were randomised to once-daily oral fingolimod (N=107) or once-weekly intramuscular IFN β-1a (N=108). HRQoL outcomes were assessed using the 23-item Pediatric Quality of Life (PedsQL) scale that comprises Physical and Psychosocial Health Summary Scores (including Emotional, Social and School Functioning). A post hoc inferential analysis evaluated changes in self-reported or parent-reported PedsQL scores from baseline up to 2 years between treatment groups using an analysis of covariance model.
Results Treatment with fingolimod showed improvements versus IFN β-1a on the PedsQL scale in both the self-reported and parent-reported Total Scale Scores (4.66 vs −1.16, p≤0.001 and 2.71 vs −1.02, p≤0.05, respectively). The proportion of patients achieving a clinically meaningful improvement in the PedsQL Total Scale Score was two times higher with fingolimod versus IFN β-1a per the self-reported scores (47.5% vs 24.2%, p=0.001), and fingolimod was favoured versus IFN β-1a per the parent-reported scores (37.8% vs 24.7%, p=non-significant). Group differences in self-reported Total Scale Scores in favour of fingolimod were most pronounced among patients who had ≥2 relapses in the year prior to study entry or who showed improving or stable Expanded Disability Status Scale scores during the study.
Conclusion Fingolimod improved HRQoL compared with IFN β-1a in patients with PoMS as evidenced by the self-reported and parent-reported PedsQL scores.
- multiple sclerosis
- quality of life
- paediatric neurology
Data availability statement
Data are available upon reasonable request. Once the 5-year open-label extension has been completed, the reader will be able to request the raw data (anonymised) and related documents (eg, protocol, reporting and analysis plan, clinical study report) that underlie the results reported in this article by connecting to https://www.clinicalstudydatarequest.com and signing a Data Sharing Agreement with Novartis. These will be made available to qualified external researchers with requests reviewed and approved by an independent review panel on the basis of scientific merit.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The global incidence of paediatric-onset multiple sclerosis (PoMS) ranges from 0.05 to 2.85 per 100 000 children1 and globally at least 30 000 children below the age of 18 years are living with MS.2 PoMS compared with adult-onset MS is associated with more frequent relapses3 4 and a higher MRI lesion burden,5 resulting in disability accumulation and a transition to a secondary progressive course at a younger age in adulthood.6 7
PoMS can adversely affect physical and psychosocial well-being, and is associated with fatigue, depression and cognitive impairment.8–10 Patients with PoMS may experience troubling behavioural symptoms,11 challenges in academic performance and social interactions, and a reduced quality of life (QoL) during the key formative years of education.8–10 12 Measuring and addressing health-related QoL (HRQoL) in PoMS informs patient management with respect to how the MS diagnosis and associated symptoms affect daily functioning in these young individuals. The importance of incorporating HRQoL measures into clinical research and treatment is highlighted by the US Food and Drug Administration and European Medicines Agency, which have emphasised that HRQoL is an essential patient-reported outcome (PRO) in the assessment of patients with chronic illnesses.13 14
The relative effects of PoMS on daily functioning and QoL are incompletely characterised, and the relative effects of HRQoL across different disease-modifying therapies are yet to be explored. Here, we report the HRQoL outcomes from PARADIGMS, the first completed clinical trial in PoMS that led to the approval of a disease-modifying therapy in several countries for paediatric patients aged 10 years and older.15 16 The PARADIGMS Study showed that oral once-daily fingolimod compared with intramuscular weekly interferon (IFN) β-1a had superior efficacy in relapse and new MRI lesion outcomes. We applied a well-validated instrument, the Pediatric Quality of Life (PedsQL) scale, and its Emotional, Social and School Functioning subscales17 to all study participants to compare HRQoL outcomes between treatment groups and better understand the factors underlying HRQoL in PoMS.
Methods
Study design and patient population
PARADIGMS was a randomised, double-blind, double-dummy, active-controlled, parallel-group, multicentre study of up to 2 years, followed by a 5-year open-label extension period.18 Patients (N=215) were randomised (1:1) to receive either oral fingolimod (N=107; 0.5 mg once daily for >40 kg body weight and 0.25 mg once daily for ≤40 kg body weight) or intramuscular IFN β-1a 30 µg once weekly (N=108). The study included patients aged 10–<18 years at randomisation with a diagnosis of MS; an Expanded Disability Status Scale (EDSS) score of 0–5.5 and ≥1 MS relapse in the past year; ≥2 MS relapses in the past 2 years; or evidence of ≥1 gadolinium-enhancing lesion on T1-weighted MRI within 6 months before randomisation (including the screening MRI). Further details of the study design and population have been reported in the primary publication (PARADIGMS ClinicalTrials.gov number, NCT01892722)18 in accordance with the Consolidated Standards of Reporting Trials guidelines.
HRQoL assessments and outcomes
The HRQoL measures have been demonstrated as predictors of health.19 Among the tools to assess HRQoL in the paediatric population with chronic illnesses, the PedsQL scale is an established, validated instrument for the measurement of HRQoL, and its Emotional, Social and School Functioning subscales may be used to examine functional domains.17 The PedsQL questionnaire requires little time for completion (less than 5 min) and assesses both the children’s (self-reported) and parent’s (parent-reported) views, providing invaluable information for the evaluation of the children’s HRQoL that may inform clinical decision-making and treatment plans. Moreover, this tool has been translated and validated in other languages and usefully applied in previous studies to evaluate QoL determinants in patients with PoMS and their parents.12 20
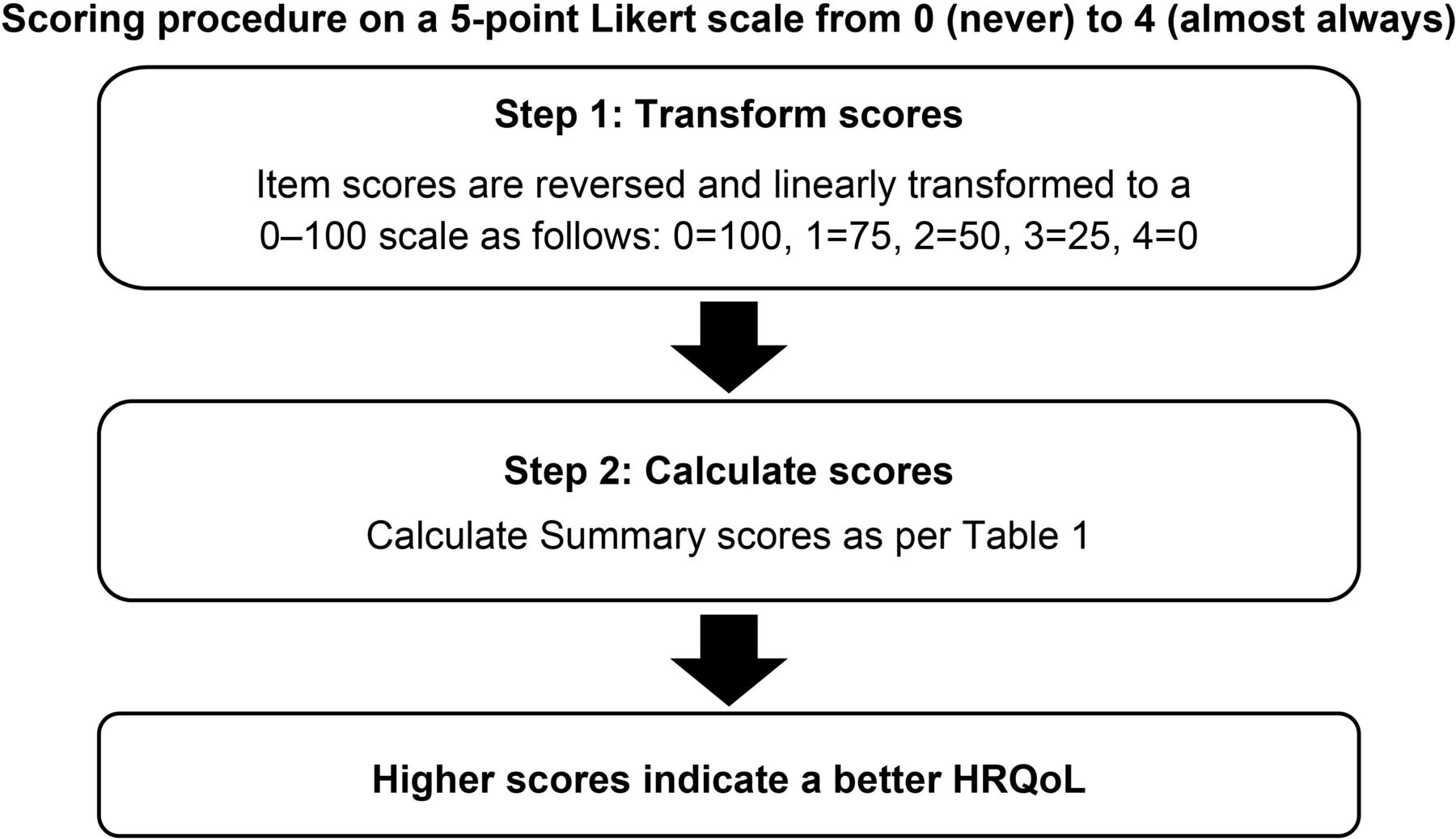
The PedsQL scale uses a modular approach to measure the core dimensions of health as delineated by the WHO, including school functioning. The 23-item PedsQL scale comprises the Physical Health Summary Score (8 items) and Psychosocial Health Summary Score (15 items; subdivided into 3 multidimensional scales: Emotional (5 items), Social (5 items) and School (5 items) Functioning), which together make up the Total Scale Score (table 1). The questionnaire was tailored to record responses by different age groups (8–12 years and 13–18 years) and included separate child self-reporting and parent proxy-reporting scales; the items for each form were essentially identical, differing in developmentally appropriate language (figure 1). The scoring was done on a 5-point Likert scale, with each item attributed a score from 0 (‘if it is never a problem’) to 4 (‘if it is almost always a problem’) based on how much of a problem each item had been during the past month. For ease of interpretability, item scores were reversed and linearly transformed to a 0–100 scale so that higher scores indicated better HRQoL (figure 2). PedsQL was administered in all patients at baseline, month 12, month 24 and at the end of study (EOS). The outcomes included changes in total and individual summary scores of the PedsQL scale from baseline to EOS per self-reporting and parent-reporting.
Dimensions of the PedsQL scales
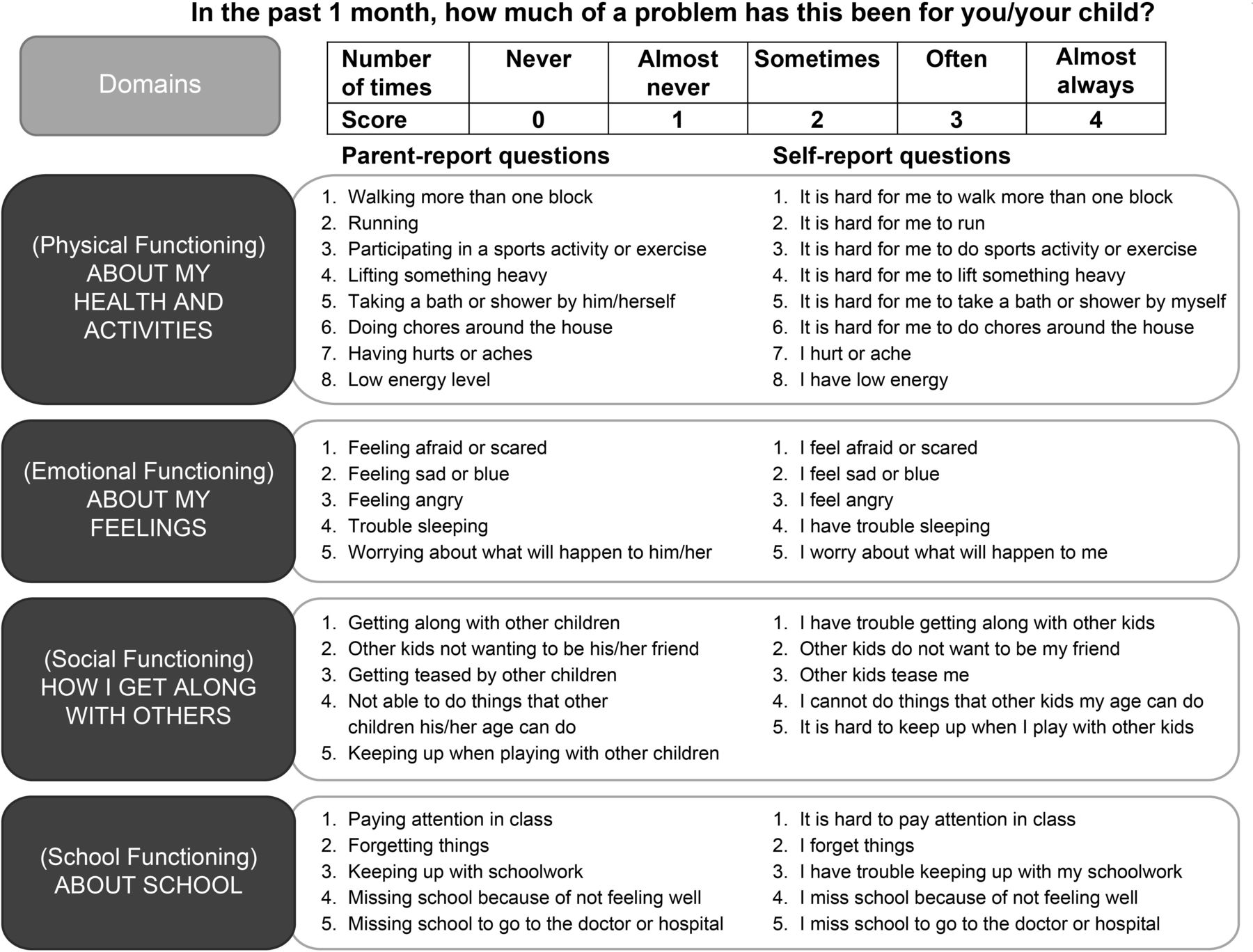
Examples of questions from the PedsQL parent-reporting and self-reporting scale. PedsQL, Pediatric Quality of Life.

Scoring procedure for the PedsQL scale. HRQoL, health-related quality of life; PedsQL, Pediatric Quality of Life.
Statistical analysis
The differences in PedsQL scores between the groups treated with fingolimod and IFN β-1a were determined by a post hoc inferential analysis. The least square (LS) mean changes from baseline in the Total Scale Score, Physical Health Summary Score and Psychosocial Health Summary Score (including Emotional, Social and School Functioning) were compared by visit for the self-reported and parent-reported PedsQL scores using a parametric analysis of covariance model. This model was adjusted for treatment (arm), pubertal status, sex, number of relapses in the 2 years prior to the study, EDSS at baseline and the corresponding baseline PedsQL scale score.
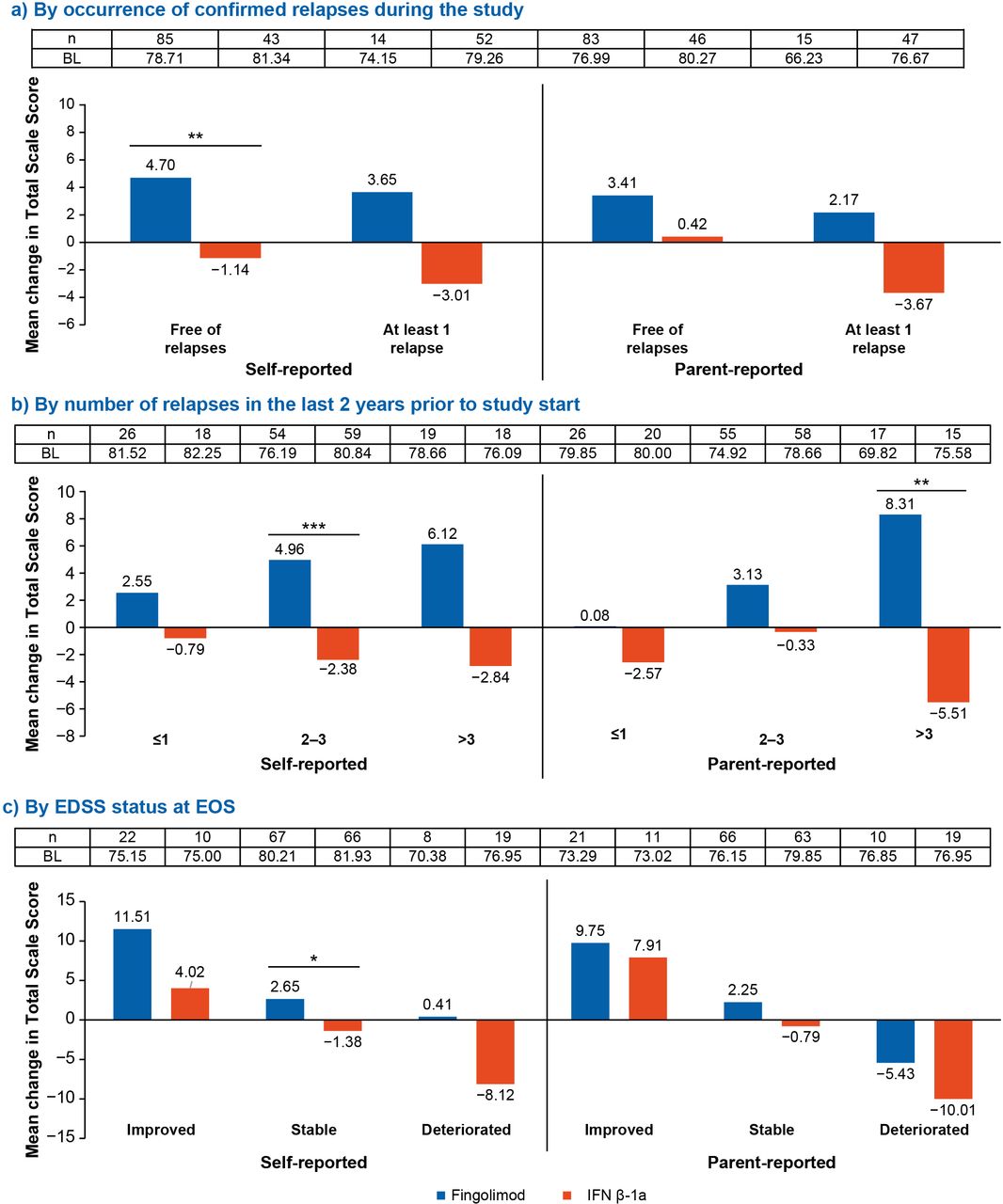
The mean changes in the PedsQL scale and subscale scores were also analysed in different subgroups of patients defined by the occurrence of confirmed relapses (free of confirmed relapses or at least one confirmed relapse before EOS) during the study, number of relapses (≤1 relapse, 2–3 relapses or >3 relapses) in the last 2 years prior to the start of the study and changes in the EDSS scores (stable, improved or deteriorated (refer to figure 3 for the definition of these categories)) at EOS. At each HRQoL assessment time point, only patients with a value at both baseline and the respective time point were included. The p value was determined from a Wilcoxon rank-sum test. In addition, the PedsQL scale and subscale scores at months 12 and 24 were also compared between the study arms based on the reported severity of the most severe adverse event (AE; mild, moderate and severe).
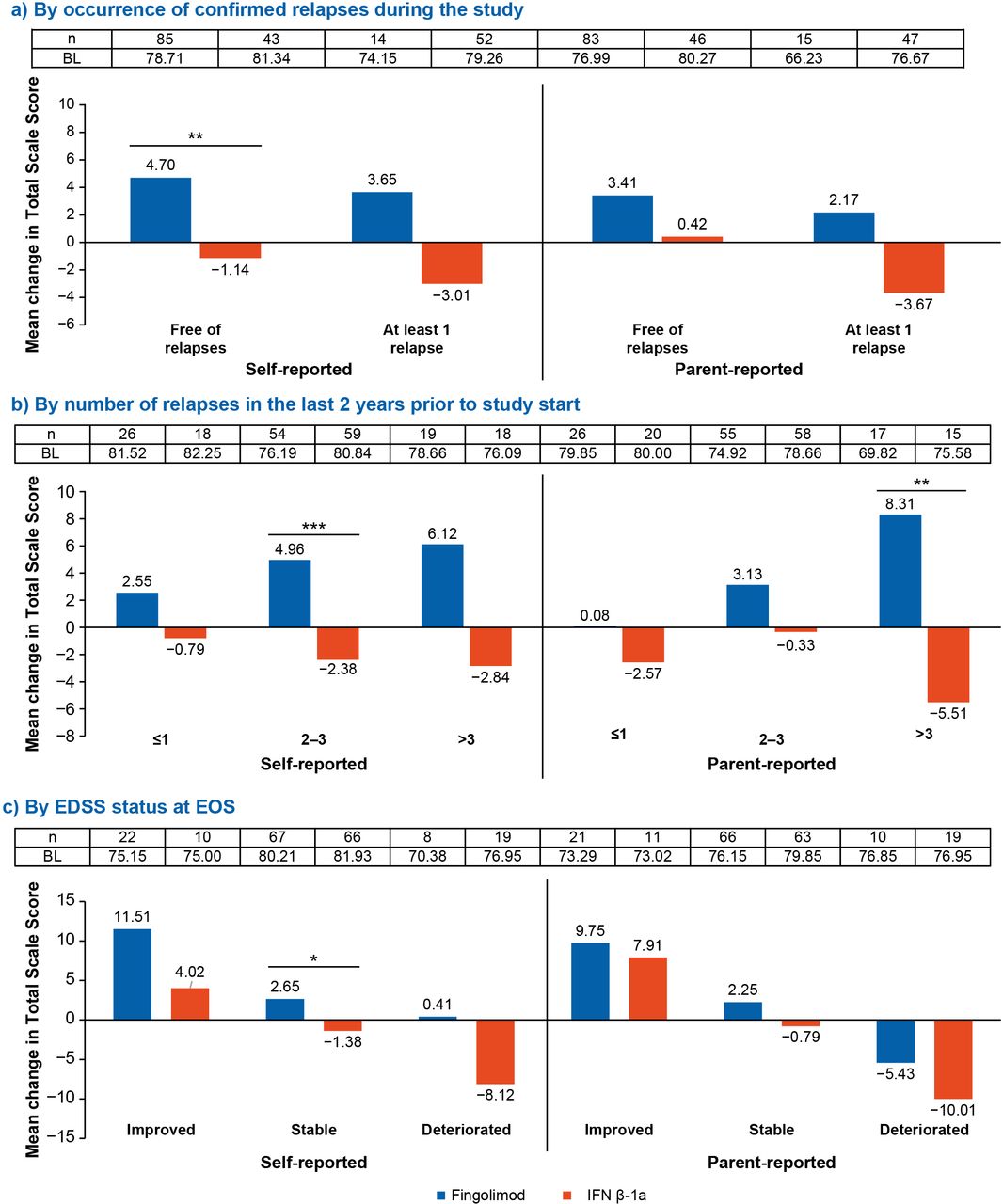
Mean change in total PedsQL scale score at EOS per the self-reports and parent-reports by (A) occurrence of confirmed relapses during the study, (B) number of relapses in the last 2 years prior to study start and (C) EDSS status at EOS. *p≤0.1; **p≤0.05; ***p≤0.01. The p values are from a Wilcoxon rank-sum test and represent the significant effect of fingolimod versus IFN β-1a. BL indicates the mean baseline PedsQL scale score. For patients with a baseline EDSS score of ≤5.0, a decrease of ≤1 point is defined as improvement, a change from –0.5 to 0.5 is defined as stable and an increase of ≥1 point is defined as deterioration; for patients with a baseline EDSS score of >5.0, a decrease of ≤0.5 point is defined as improvement, 0 change is defined as stable and an increase of ≥0.5 point is defined as deterioration. BL, baseline; EDSS, Expanded Disability Status Scale; EOS, end of study; IFN, interferon; n, number of subjects with a value at both baseline and EOS; PedsQL, Pediatric Quality of Life.
The proportion of patients with clinically meaningful improvement in the PedsQL Total Scale Scores and subscores was determined using the two-tailed Fisher’s exact test. Differences of 4.36 points for the child self-reported scores and 4.50 points for the parent proxy-reported scores from baseline are considered minimal clinically important changes; as such, greater differences were considered meaningful.21 22 In the current analysis, a more conservative approach of 5 points was considered to report clinically meaningful difference in PedsQL score.
Results
Patient disposition and baseline characteristics
Of the 215 randomised patients, 214 received study medication and were included in the full analysis set (fingolimod, n=107; IFN β-1a, n=107) and 188 completed the core phase (fingolimod, 100 (93.5%); IFN β-1a, 88 (81.5%), online supplemental table 1). The mean (SD) age of patients was 15.3 (1.81) years, ranging between 10 and <18 years at randomisation, and most were female (~62%). The baseline PedsQL scores were similar between the treatment groups (table 2). Further details on patient disposition and baseline characteristics are reported in the primary and secondary publications.18 22 23
Supplemental material
Mean baseline and end of study PedsQL scale scores (full analysis set)
Changes in the PedsQL scores
Overall population
The LS mean changes in PedsQL scales and subscales from baseline to EOS are presented in figure 4. Compared with IFN β-1a, fingolimod showed a significant effect (p≤0.05) on all of the self-reported PedsQL scale and subscale scores, except for Social Functioning (1.30 for fingolimod vs −1.27 for IFN β-1a). The Total Scale and Physical Health Summary Scores were greater for the fingolimod group (p≤0.05) in the parent-reported questionnaires, whereas the Psychosocial Health Summary Score (including Emotional, Social and School Functioning) favoured fingolimod but did not reach statistical significance.
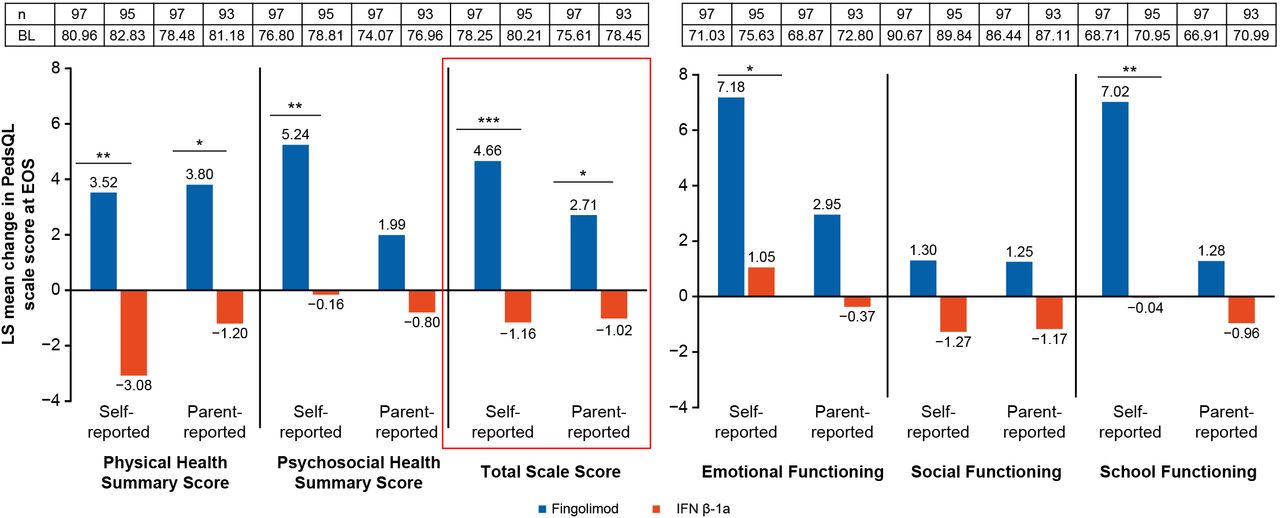
LS mean change in the PedsQL scale and subscale scores at EOS per the self-reports and parent-reports. *p≤0.05; **p≤0.01; ***p≤0.001. BL indicates the mean baseline PedsQL scale score. EOS is defined as the last assessment taken on or before the final study phase visit date. LS mean change is obtained from an ANCOVA model adjusted for treatment, pubertal status, sex, number of relapses in the 2 years prior to the study, EDSS at baseline and the baseline value of the respective PedsQL scale. ANCOVA, analysis of covariance; BL, baseline; EDSS, Expanded Disability Status Scale; EOS, end of study; IFN, interferon; LS, least square; n, total number of patients with available results for the corresponding time point or time window and included in the analysis; PedsQL, Pediatric Quality of Life.
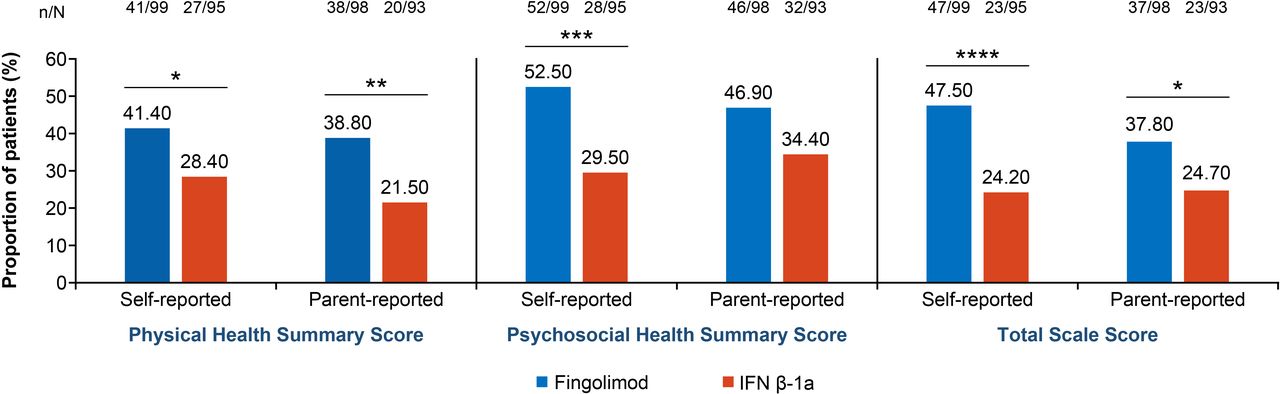
The proportion of patients achieving a clinically meaningful improvement in the PedsQL Total Scale Score was higher with fingolimod versus IFN β-1a per the self-reported scores (47.5% (fingolimod) vs 24.2% (IFN β-1a); p=0.001), and fingolimod was favoured per the parent-reported scores (37.8% (fingolimod) vs 24.7% (IFN β-1a); p=non-significant) (figure 5). Further, the self-reported Psychosocial Health Summary Score (52.5% (fingolimod) vs 29.5% (IFN β-1a); p≤0.01) and parent-reported Physical Health Summary Score (38.8% (fingolimod) vs 21.5% (IFN β-1a); p≤0.05) were found to contribute to the Total Scale Score of the PedsQL scale.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportion of patients with clinically meaningful improvement in the PedsQL scale scores at EOS per the self-reports and parent-reports. *p≤0.1; **p≤0.05; ***p≤0.01; ****p≤0.001. The p values for the treatment comparison are based on a two-tailed Fisher’s exact test. EOS, end of study; IFN, interferon; N, number of patients with an assessment; n, number of patients with at least a 5-point increase in the score; PedsQL, Pediatric Quality of Life.
Subgroups
Figure 3 summarises the mean changes in the PedsQL total scores for self-reported and parent-reported PedsQL scores on three subgroup analyses of patients defined by: (1) occurrence of confirmed relapses during the study (figure 3A), (2) number of relapses in the last 2 years prior to study start (figure 3B) and (3) EDSS status at EOS (figure 3C). Interestingly, among the self-reported Total Scale Scores, significantly greater improvement (p≤0.05) in the PedsQL score was noted with fingolimod versus IFN β-1a in the subgroup of patients who were free of relapse during the study. The subgroup of patients who had two to three relapses in the years prior to study start had greater improvement with fingolimod versus IFN β-1a (p≤0.01) in the Total Scale Scores as observed in the self-reported scores.
In the subgroup of patients whose EDSS remained stable or worsened, PedsQL scores were in favour of fingolimod versus IFN β-1a but the differences did not reach significance.
Further, for the PedsQL subscores, a significant effect was observed with fingolimod (n=85) versus IFN β-1a (n=43, both p≤0.05) for the self-reported Physical Health Summary and Psychosocial Health Summary Scores in the subgroup of patients who were free of relapses during the study (online supplemental table 2A). For the remaining subgroups, the changes in PedsQL scores were in favour of fingolimod treatment versus IFN β-1a.
When analysed by the number of relapses in the last 2 years prior to the start of the study (online supplemental table 2B), fingolimod (n=54) versus IFN β-1a (n=59) resulted in significant improvements in the self-reported Psychosocial Health Summary (p≤0.01), Emotional Functioning (p≤0.01), Social Functioning (p≤0.05) and School Functioning (p≤0.05) scores in the subgroup of patients who had two to three relapses (online supplemental table 2B). The parent-reported Physical Health Summary and School Functioning scores were significantly (both p≤0.05) improved with fingolimod (n=17) versus IFN β-1a (n=15) in patients who had experienced more than three relapses prior to study entry. The improvement in HRQoL in the remaining subscales of the PedsQL and in the subgroups by relapses favoured fingolimod but did not reach statistical significance for both self-reported and parent-reported scores.
When we analysed the mean change in PedsQL scales and subscales by EDSS status at EOS (online supplemental table 2C), fingolimod (n=22) showed an effect versus IFN β-1a (n=10) in the self-reported Physical Health Summary Score in patients who had an improved EDSS score (p≤0.05) and in the Psychosocial Health Summary (fingolimod, n=67 and IFN β-1a, n=66) and Emotional Functioning scores (fingolimod, n=67 and IFN β-1a, n=66) in patients who had a stable EDSS score (both p≤0.05).
The mean changes in the PedsQL scale and subscale scores in patients with any AE between baseline and month 12 and between month 12 and month 24 showed improvement with fingolimod versus IFN β-1a. All the AEs began before the last treatment dose. The improvement in the PedsQL scores in the fingolimod-treated patients was similar across the mild, moderate and severe subgroup AE categories, regardless of being self-reported or parent-reported (data not presented). The results are from a small sample size.
Discussion
In this post hoc inferential analysis of the PARADIGMS Study, treatment with fingolimod versus IFN β-1a showed improvements on the PedsQL scale for both the self-reported and parent-reported Total Scale Score.
Overall, a twofold higher proportion of patients achieved clinically meaningful improvement in the PedsQL Total Scale Score with fingolimod versus IFN β-1a per the self-reported scores, and fingolimod was favoured versus IFN β-1a per the parent-reported scores. These results reflect the positive impact of fingolimod treatment on HRQoL in paediatric patients while parents and children were blinded for the study. Among the subgroup analyses, patients who had ≥2 relapses in the year prior to study entry or who showed improving or stable EDSS scores showed pronounced improvement with fingolimod as reflected in the self-reported Total Scale Scores.
HRQoL has rarely been evaluated in paediatric MS therapeutic studies. In the single-arm observational FUTURE Study of IFN β-1a by intramuscular injection,24 the QoL of patients was slightly but not significantly improved with subcutaneous IFN β-1a, when compared with pretreatment. When compared with the self-reported scores, the parent-reported scores were higher with improvements of +5.90 in the ‘Psychosocial Health Summary Score’ and +7.84 in the ‘School Functioning Score’ versus baseline, suggesting that parents perceived more improvement in aspects of HRQoL than did the patients themselves. In contrast, in the current double-blind, double-dummy PARADIGMS Study, a consistent worsening was observed in the IFN β-1a-treated patients, as assessed by self-reported and parent-reported PedsQL scores. Lower QoL scores with IFN β-1a might have influenced patients’ decision to remain in the study, as 18.5% of the patients in the IFN β-1a arm discontinued the PARADIGMS Study mainly owing to an unsatisfactory therapeutic effect, AEs and withdrawal of consent.18 The different results of the two studies could depend on different study designs, differing clinical settings and the post hoc nature of data analysis in the PARADIGMS Study.
The present PARADIGMS Study showed that the LS mean change in the PedsQL scale and subscale scores was significant for all outcomes at EOS per the self-reported and parent-reported scores, except for the parent-reported Psychosocial Health Summary Score. This result corroborates literature that suggests that parents tend to be better at reporting their child’s observable behaviour (physical domains) rather than their children’s internal state of mind or feelings (emotional or social domains) considering that the child is the only person who can actually inform about their feelings.12 20 25 26 Proxy responses are not always equivalent to those provided by a patient,22 27 however, it is typically the parents' perception of their child’s symptoms and outcomes that influence healthcare utilisation.28 As such, the Food and Drug Administration industry guidance for PROs encourages observers (parents or proxy) to collect responses related to events or behaviours that can be observed versus psychosocial feelings that can only be known by the patient.14
Acute relapse or neurological disability has been consistently found to be associated with a lower QoL in adult and paediatric patients with MS assessed using EQ-5D or PedsQL instruments.22 29 30 In the PARADIGMS Study, fingolimod-treated patients showed improvement in the PedsQL scores, as reflected in the subgroup analysis of patients who had 2–3 or >3 relapses in the last 2 years prior to the start of the study; were free of confirmed relapses during the study; or (despite the narrow range in EDSS scores) had an improved or stable EDSS at EOS. The greater mean change in the self-reported Physical Health Summary, Psychosocial Health Summary and Total Scale Scores of the PedsQL scale favoured fingolimod over IFN β-1a. The improvements in PedsQL scores and HRQoL reinforce the benefits to patients with PoMS seen in the previously reported findings from the PARADIGMS (a greater reduction in relapses or higher number of relapse-free patients or an improved/stable EDSS).18
School performance and emotional well-being are key concerns in these young patients. Further, patients with paediatric MS have been shown to have a range of emotional and clinical problems11 and individuals with paediatric MS relative to monophasic inflammatory events have higher frequencies of depressive symptoms.31 Similar elevated levels of depressive symptoms and anxiety have been found for youth with other chronic illness such as type I diabetes32, epilepsy, allergies33 and Crohn’s disease.34 Hence, medical therapies which are associated with better self-reported and parent-reported QoL are critical to the patients’ well-being. Patients with PoMS may also experience reduced school performance as measured by failing grades or classes.35 Other studies show comparable performance of patients with PoMS relative to their peers but emphasise increased psychiatric comorbidity.36 Fingolimod-treated patients experienced clinically meaningful improvement in the Psychosocial Health Summary subscales, that is, emotional and school domains, versus increased worsening in IFN β-1a-treated patients.
Limitations
There were some limitations in the study that must be acknowledged. These include low number of people with PedsQL assessment at month 24, the post hoc nature of subgroup analysis and the QoL assessments being not the primary study endpoint of the core trial.
Conclusions
In conclusion, fingolimod significantly improved HRQoL compared with intramuscular IFN β-1a in patients with PoMS in the PARADIGMS Study. These results suggest that the therapies that have strong effects on relapse rates and are well tolerated also show positive effects on the QoL of patients with PoMS. Given that prior research has shown a low adherence rate for MS therapies in patients with PoMS,37 therapies that improve HRQoL are promising in their potential to promote medication adherence. Furthermore, improvement in psychosocial well-being of patients is also a key driver of improvement in PoMS. As MS is a chronic illness, these positive steps to improve patient experience are fundamental to QoL.
Data availability statement
Data are available upon reasonable request. Once the 5-year open-label extension has been completed, the reader will be able to request the raw data (anonymised) and related documents (eg, protocol, reporting and analysis plan, clinical study report) that underlie the results reported in this article by connecting to https://www.clinicalstudydatarequest.com and signing a Data Sharing Agreement with Novartis. These will be made available to qualified external researchers with requests reviewed and approved by an independent review panel on the basis of scientific merit.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol and amendments were approved by the independent ethics committees and institutional review boards for each centre per local regulations. All patients or legal guardians of paediatric patients provided written informed consent before study entry. The study was conducted in compliance with the ethical principles of the Declaration of Helsinki38 and the International Conference on Harmonisation Good Clinical Practice Guidelines.39
Acknowledgments
The authors acknowledge the patients, investigators and staff at participating sites for supporting the conduct of the study. They thank Arshjyoti Singh and Anuja Shah (Novartis Healthcare, Hyderabad, India) for providing medical writing support, which encompassed a literature search, writing of the manuscript, formatting, referencing, preparation of tables and figures per the journal guidelines and incorporating the authors’ revisions and finalising the draft for submission, all under the direction of the authors. The authors thank Gillipsie Minhas (Novartis Healthcare, Hyderabad, India) for providing technical assistance for submission of the manuscript and Rohit Bhandari (Novartis Healthcare, Hyderabad, India) for helping during the manuscript revisions.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LK contributed to the conception of the study, execution of the study, interpretation of the study data, outlining the manuscript content and critical revision of the manuscript for content. BB contributed to the conception of the study, interpretation of the study data, drafting the manuscript content and critical revision of the manuscript for content. TC contributed to the conception of the study, execution of the study, acquisition of the data, interpretation of the study data, outlining the manuscript content and critical revision of the manuscript for content. KD contributed to the acquisition of the data, analysis of the data, interpretation of the study data, outlining the manuscript content and critical revision of the manuscript for content. JG contributed to the conception of the study, acquisition of the data and critical revision of the manuscript for content. AG contributed to conception of the study, execution of the study, acquisition of the data, interpretation of the study data, outlining the manuscript content and critical revision of the manuscript for content. PH contributed to analysis of the data, interpretation of the study data, drafting of the manuscript content and critical revision of the manuscript for content. EW contributed to execution of the study, acquisition of the data, interpretation of the study data and critical revision of the manuscript for content. VD contributed to interpretation of the study data, drafting the manuscript content and critical revision of the manuscript for content. AA contributed to the statistical analysis, data analysis, interpretation of the study data, drafting the manuscript content and critical revision of the manuscript for content. RK contributed to the conception of the study, design of the study, execution of the study, acquisition of the data, analysis of the data, interpretation of the study data, drafting the manuscript content and critical revision of the manuscript for content. All named authors take responsibility for the integrity of the work as a whole and have given final approval for the version to be published. All authors are responsible for intellectual content and data accuracy. LK is the gurantor of this work.
Funding This work was supported by Novartis Pharma AG, Basel, Switzerland.
Competing interests LK received personal compensation for activities as a consultant and/or participant on advisory boards for Biogen, Eisai, Gerson Lehrman, Janssen, Medscape, NeuroLive, Novartis, Roche and Sanofi. She has received royalties for the Fatigue Severity Scale from pharmaceutical and biotechnology companies, grant support from the National Multiple Sclerosis Society, and Department of Defense and research support from Novartis, Biogen, Genentech, the Lourie Foundation. She was compensated for her role as a back-up central MRI reviewer for the PARADIGMS Study. BB served as a consultant for Biogen Idec, Novartis, Teva Neuroscience, Merck Serono, Canadian MS Society Scientific Research Foundation, Canadian Multiple Sclerosis Society, National Multiple Sclerosis Society and Canadian Institutes of Health Research. She served as a remunerated central MRI reviewer for the present study. TC received personal compensation for advisory boards/consulting from F Hoffman-La Roche, Biogen and Novartis and financial support for research activities from the National Multiple Sclerosis Society, NIH and Department of Defense, Biogen, Merck Serono, Verily and Novartis. KD received personal compensation for speaker activities from Novartis, Servier, Biogen and Sanofi. JG, in the last 3 years, received honoraria for lectures and consultancy fees from Bayer, Novartis and Sanofi as well as funding for a research project from Novartis. AG received honoraria for speaking from Almirall, Biogen Idec, Merck Serono, Novartis, Genzyme and Sanofi-Aventis and for consultancy from Merck Serono, Biogen Idec, Teva, F Hoffmann-La Roche and Novartis. PH received honoraria for lectures and consultancy fees from Bayer, Merck, Biogen and Novartis. EW is funded by the NIH, NMSS, PCORI and Race to Erase MS. She volunteers on an advisory board for a Novartis trial. She is a site PI for clinical trials with Roche and Novartis. She has received honoraria from MS@TheLimit and The Corpus for educational talks. VD, AA and RK are employees of Novartis.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.