Article Text

Abstract
Introduction Epilepsy is closely related to daily rhythms, such as the sleep–wake cycle. The objective of this study was to evaluate the relationship between drug-resistant temporal lobe epilepsy (TLE) and the parameters related to the sleep–wake cycle, seizure time and epilepsy laterality.
Methods Consecutive patients admitted to the video electroencephalogram unit with a diagnosis of TLE were enrolled. Patients were divided into two groups: those with left TLE (LTLE) and those with right TLE (RTLE). They then remained in the conditions of 12-hour light, 12-hour darkness. Demographic data, treatment, number and time of seizure occurrence, sleep diary, morningness–eveningness questionnaire, Pittsburgh Sleep Quality Index and Epworth Sleepiness Scale were recorded.
Results In total, 74 patients with TLE, 43 with LTLE and 31 with RTLE, were studied. RTLE patients showed a significant preference for morningness. Patients treated with benzodiazepines showed worse sleep quality and greater daytime sleepiness. Patients who did not report any clear predominance and patients who reported seizures during wakefulness had significantly more seizures during wakefulness and patients who reported sleep predominance had more seizures during sleep (p>0.001). The LTLE group had a greater number of seizures from 8 to 16 hours, unlike the RTLE group, which had a uniform distribution (p=0.008).
Conclusions This was a prospective study of patients with drug-resistant TLE performed in a controlled environment to study the impact of daily rhythms, seizure frequency and seizure distribution. Laterality seems to be a key factor in seizure distribution.
- EPILEPSY
- SLEEP
- NEUROBIOLOGY
- NEUROPHYSIOLOGY
- NEUROPHARMACOLOGY
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Study of the rhythmicity of epilepsy is becoming more relevant, as well as its relationship with the sleep–wake rhythm. Most series report a peak occurrence of seizures during the day; however, laterality is a poorly studied factor.
WHAT THIS STUDY ADDS
Twenty-four-hour seizure distribution showed an increase in seizure frequency from 08:00 to 16:00 for all seizures. In patients with left temporal lobe epilepsy, the peak of seizures from 08:00 to 16:00 is significantly higher. Sleep-related parameters analysis showed that the most meaningful finding was that patients with right temporal lobe epilepsy significantly presented morning chronotypes. Antiseizure drugs analysis showed worst sleep quality in patients treated with benzodiazepines.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Understanding the rhythmicity of seizures could help establish chronotherapeutic strategies, prevention measures and changes in the schedule for taking antiseizure medication.
Introduction
Since the 18th century, the relationship between sleep and epilepsy has been described, specifically the impact of the sleep/wake cycle on the occurrence of epileptic seizures.1–5 Sleep is a reversible state in which one is unresponsive to the environment.6 Sleep consists of two phases: rapid eye movement (REM) and non-REM (NREM) sleep. NREM sleep is further divided into stages N1, N2 and N3 sleep based on electroencephalography (EEG) patterns. In adult humans, sleep consists of approximately 5% N1, 50% N2, 15% N3 and 25%–30% REM sleep.2 6
Epilepsy is a disease of the brain defined by any of the following conditions: (1) At least two unprovoked (or reflex) seizures occurring>24 hours apart. (2) One unprovoked (or reflex) seizure and a probability of further seizures similar to the general recurrence risk (at least 60%) after two unprovoked seizures, occurring over the next 10 years. (3) Diagnosis of epilepsy syndrome.7
The relationship between focal epilepsy and the time of seizure occurrence has been described previously. Temporal lobe seizures occur more frequently during the light period, whereas frontal lobe seizures occur mostly during the dark period, particularly during NREM sleep, stages N1 and N2, but not during REM sleep.2–4 Sleep has no significant effect on the seizure duration or ictal EEG changes in patients with focal onset epilepsy.8 Generalised onset epilepsy, mainly in juvenile myoclonic epilepsy, occurs more frequently during awakening.9
Epilepsy modifies sleep, causing sleep fragmentation and decreases the duration of REM sleep and the NREM stages N3.10 In relation to the laterality of epilepsy, patients with left temporal lobe epilepsy (LTLE) showed a lower percentage of REM sleep than those with right temporal lobe epilepsy (RTLE).11
Chronotype refers to the behavioural manifestation of the underlying circadian rhythms of numerous physical processes. A person’s chronotype is the propensity for the individual to sleep at a particular time during a 24-hour period. It reveals individual circadian phases.12 To date, some studies have reported that chronotype, sleep quality and daytime sleepiness do not differ between epilepsy patients and healthy controls.13–16 Chronotype has been studied in focal onset epilepsy; two studies have shown no differences in chronotype between patients with epilepsy and controls.13 14 However, Manni et al15 reported that patients with focal epilepsy tend to be morning oriented and perceive themselves as morning types, even though this was not reflected in their dim light melatonin onset values.
The hypotheses of this work are: Sleep quality, daytime sleepiness and chronotype are altered in patients with temporal lobe epilepsy (TLE), and also, 24 hours daily rhythms present their own characteristics according to the side of the epilepsy, in adult patients with refractory TLE.
In this study, we evaluated the relationship between right-sided and left-sided drug-resistant TLE,1,7 18 time of seizure occurrence and sleep–wake rhythm in hospitalised patients at the videoEEG unit for 5 consecutive days when subjected to a 12-hour light, 12-hour dark cycle.
We expect that the present study will contribute to the understanding of the daily rhythms of focal TLE and help in the development of therapeutic strategies based on the behavioural changes related to sleep habits and to establish chronopharmacological strategies.
Methods
Subjects
In this study, we prospectively included 74 consecutive patients diagnosed with drug-resistant TLE, who, given their clinical condition, were hospitalised from July 2016 to December 2019 in the video-electroencephalogram (VEEG) unit of Ramos Mejía Hospital (Ciudad Autónoma de Buenos Aires, Buenos Aires, Argentina) and El Cruce Dr. Nestor C. Kirchner Hospital (Ciudad de Florencio Varela, Buenos Aires, Argentina). The same professional team assisted the patients in both institutions.
Inclusion criteria: Patients of both sexes (16–50 years old) with a diagnosis of drug-resistant TLE.
Exclusion criteria: Patients with psychosis, dementia or bipolar disorder, progressive neurological conditions (dementia, high-grade brain tumours, encephalopathies), previous surgery for epilepsy, those on melatonin or corticosteroid treatment.
Diagnosis
Clinical and electrical semiology was analysed using video electroencephalogram (VEEG) records for a period that ranged from 4 to 5 days. Seizures were evaluated by two expert specialists who had received training on VEEG. Every seizure was examined 3–4 times to identify semiological signs. All patients were evaluated with at least 1.5 T MRI with epilepsy protocol. Clinical and EEG analysis, as well as MRI studies, allowed us to ascertain the epileptogenic zone in patients with epilepsy. Patients with TLE were classified into two groups: those with LTLE and those with RTLE. Laterality was confirmed with clinical evolution and epilepsy surgery outcome. Patients whose seizure laterality and localisation could not be determined were excluded. Patients with non-epileptics events were excluded.
Video electroencephalography
VEEG records were obtained from all patients using a digital device (Bioscience Vector and Stellate Harmonie, Pleasanton, CA, USA, and Micromed and Cervello, Veneto, Italy). For this, 32 electrodes were positioned on the scalp, as indicated by the International 10–20 system, and the sampling frequency was 200 Hz. A mean mastoid reference was used. VEEG recording were performed during 24 hours a day and supervised and stored by an EEG technician. Antiseizure drugs were tapered, if necessary, from second day of recording. No sleep deprivation or any extra EEG activation was performed.
Experimental procedure
The patients maintained their usual sleep/wake pattern the week before hospitalisation. Participants were hospitalised at 08:00 after signing informed consent forms. Electrodes were positioned on the scalp and the VEEG study was started.
On the first day, each patient completed the following: (a) chronotype questionnaire; (b) Pittsburgh Sleep Quality Scale; (c) Epworth Sleepiness Scale (ESS); and (d) sleep diary based on the week before hospitalisation. The room lighting conditions were 12-hour light, 12-hour dark. To facilitate darkness at 20:00, each patient was provided with an eye mask. On the second day, the eye mask was removed at 08:00. All electroclinical variables (VEEG data) were registered and recorded during the first and second days. The participants were asked not to consume stimulating substances, such as caffeine or theobromine, during the experiment.
Demographic and clinical questionnaire
The questionnaire included questions on the medical history, seizure semiology, sex, age, weekly seizure frequency (seizure diary), age at epilepsy onset, nocturnal or diurnal predominance of seizures, current antiseizure treatment, number of antiseizure drugs, pharmacological history and type of MRI lesions. We defined predominance as more than 50% of seizures occurring during day or night. No patient reported paroxysmal sleep disorders. Treatment with benzodiazepines and phenobarbital was analysed differentially.
Chronotype questionnaire
Patients’ chronotypes were determined using a modified version of the Horne and Ostberg questionnaire.19 This self-assessment questionnaire was used to determine morningness–eveningness (M/E) in human circadian rhythms. In this case, the language was adapted for Argentinian patients. The morningness–eveningness questionnaire (MEQ) is composed of 19 items on diurnal preferences for different activities. The total score obtained by adding the scores on all items was used to estimate the M/E. The score ranged from 16 to 86, and participants were classified into five categories: extreme evening, moderate evening, intermediate, moderate morning and extreme morning types. Higher MEQ scores indicated stronger morningness preference. We used the following cut-offs of MEQ scores: (1) 16–30 for evening preference, (2) 31–41 for moderate evening preference, (3) 42–58 for intermediate preference, (4) 59–69 for moderate morning preference and (5) 70–86 for morning preference. The translated version of the MEQ used in this study is included in the online supplemental appendix 1.
Supplemental material
Pittsburgh Sleep Quality Index (PSQI)
The PSQI is an instrument used to effectively measure the quality and patterns of sleep in adults,2,0 and we used its Spanish version.21 The PSQI differentiates ‘poor’ from ‘good’ sleep quality by measuring seven areas (components): subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medications and daytime dysfunction over the last month. The total score ranges from 0 to 21, with higher scores indicating poorer sleep quality (online supplemental appendix 2).
Epworth Sleepiness Scale
The evaluation of patients’ diurnal somnolence was carried out using the ESS,2,2 a Spanish version.23 24 The ESS is a self-reported questionnaire that evaluates the tendency to fall asleep in eight daily situations. Therefore, this tool allows for the classification of daytime sleepiness (DS) as no sleepiness=0–6, mild DS=7–13, moderate DS=14–19 and severe DS=20–24 (online supplemental appendix 3).
Sleep diary
Patients were required to have a sleep diary in which they recorded their sleep habits during the 7 days immediately prior to admission. The analysis of the sleep diary revealed the time of getting into bed, the time at which the individual attempted to fall asleep, sleep onset latency, number of awakenings, duration of awakenings, time of final awakening and final rise time.25
Electroclinical variables (VEEG data)
Electroclinical variables included the seizure semiology, total number of seizures, number of diurnal seizures, number of nocturnal seizures, number of seizures during sleep, number of seizures during wakefulness and number of seizures per 4-hour periods (24:00–04:00, 04:00–08:00, 08:00–12:00, 12:00–16:00, 16:00–20:00 and 20:00–24:00). For seizure semiology, seizures were classified for analysis in auras (focal aware non-motor), focal onset aware seizure, focal onset seizure with impaired awareness and focal to bilateral tonic–clonic.26 Wakefulness/sleep was determined by EEG signals according to the American Academy of Sleep Medicine criteria and video analysis.27
Statistical analyses
Clinical data were analysed using the Statistical Package for the Social Sciences software (StataCorp LP, College Station, Texas, USA), IBM SPSS software, accessed 28 September 2019. Non-parametric values were expressed as medians and IQRs. Parametric values were expressed as means and SD, and normal distribution was established using the Shapiro-Wilk test. The calculation of sample size was based on comparison of two groups of patients with distinctive TLE, with 80% power and α=0.05, needed 17 patients per group.
For comparisons between continuous variables, paired and unpaired t-tests were used. When indicated, χ2 test or Fisher’s exact test was used. Total seizure frequency was analysed first; in the second time, the analysis was performed by time blocks (24:00–04:00, 04:00–08:00, 08:00–12:00, 12:00–16:00, 16:00–20:00 and 20:00–24:00). We performed χ2 goodness of fit to study seizure time distribution. For correlation analysis simple and multiple linear regression was performed. In all cases, statistical significance was set at p<0.05. The results of the chronotype and sleep quality questionnaire were adjusted for age and sex.
Results
Clinic and demographic data
A total of 74 patients with TLE were studied: 43 had LTLE and 31 had RTLE (table 1). Their mean age was 34.4 years (SD 12). The mean age of epilepsy onset was 15.3 years (SD 10.7). The median seizure frequency was 1 (IQR 5–3) seizures per week. Regarding the self-reported seizure predominance (in relation to whether seizures occur during sleep or wakefulness), 56% of the patients did not report any clear predominance, 13.5% reported seizure predominance during sleep, 16.2% reported seizure predominance during wakefulness, 13.5% reported seizures only during wakefulness and there were no patients with seizures only during sleep (table 1).
Demographic and clinical parameters
Antiseizure treatment analysis showed that 45.9% of the patients were treated with two drugs and 32.4% with three drugs, 37.8% were treated with benzodiazepines and/or phenobarbital (table 1).
MRI data showed that the most frequent finding was mesial temporal sclerosis in 36.5% of the patients. Other findings included chronic brain injury in 16.2% of the patients, low-grade tumours in 13.5% of the patients, cortical dysplasia in 10.8% and normal MRI findings in 23%.
There were no statistically significant differences between left-sided and right-sided TLE.
Sleep-related parameter evaluation
The sleep quality (PSQI) mean score was 7.2 (SD 4.6) points (0–21 points), concordant with a slight alteration of sleep quality. The Epworth Scale mean was 7.2 (SD 4.4) points (0–24 points), with 47.3% of the patients having mild daytime sleepiness. Chronotype evaluation showed that 58.1% of the patients had the intermediate chronotype, 28.4% the morning chronotype and 13.5% the evening chronotype. The mean MEQ Score for all the patients was 51 (SD 12) points, 49 (SD 9.9) points in the LTLE group and 52 (SD 14.2) in the RTLE group (p=0.03), and patients with RTLE showed stronger morningness preference. Sleep diary evaluation showed that patients slept for an average of 69.7 hours per week (SD 15), corresponding to 15 hours of daytime sleep (SD 13) and 53 hours of night-time sleep (SD 14) per week (table 2). No differences were found in the PSQI, Epworth Scale and sleep diary evaluation between left-sided and right-sided TLE.
Scores and scales overview
We compared the chronotype, sleep quality and daytime sleepiness with the moment (day/night) from VEEG recorded seizure onset and the sleep or wake state and no correlation was observed. In the sleep diary analysis, patients with seizures during sleep reported sleeping fewer weekly hours than patients with no seizures during sleep (p=0.02).
We analysed the relationship between the different assessment tools used to evaluate the sleep/wake cycle. The PSQI and Epworth scales showed a positive correlation (rho=0.27, p=0.03), and the lower the quality of sleep was, the greater the daytime sleepiness was found to be. The Epworth Scale and MEQ were negatively correlated (rho=−0.26, p=0.04), patients with lower MEQ scores (evening type) had more daytime sleepiness.
Regarding the type of drugs, we separately analysed the patients treated with benzodiazepines and/or phenobarbital (37.8%). We found worse sleep quality (p=0.03) and an increase in daytime sleepiness in patients treated with benzodiazepines (p<0.05), although they were not observed to have more weekly sleep hours.
VEEG data results
Patients had a median of two seizures during the VEEG recording (see table 3). Seizure analysis in relation to daytime occurrence showed a total of 190 seizures: 121 (63.3%) diurnal seizures and 69 (36.6%) nocturnal seizures. A total of 131 (68.5%) seizures were observed during wakefulness and 59 (31.4%) seizures occurred during sleep. A total of 30 (40.5%) patients had seizures during only wakefulness, 8 (10.8%) patients had seizures only during sleep, 29 (39.1%) had only diurnal seizures and 13 (18.3%) had only nocturnal seizures (table 3). This analysis was performed for all seizures and we found no differences for patients with LTLE and RTLE.
VEEG overview
The distribution of seizure occurrence in 24 hours was studied according to time ranges of 4 hours (figures 1 and 2). In the LTLE group, the greatest number of seizures was recorded from 08:00 to 12:00 and from 12:00 to 16:00, representing 27.1% and 20.5% of 24-hour seizures, respectively. In the RTLE group, seizure distribution was more uniform, with 23.3% of seizures recorded from 12:00 to 16:00 and 14.4% of seizures recorded from 08:00 to 12:00 and 20:00 to 24:00. There were statistical differences between right-sided and left-sided TLE in the 24-hour distribution (p=0.008). We additionally performed a goodness of fit χ2 test, showing a different distribution than expected in LTLE (χ2=32; df=5; p<0.001) and a distribution similar to that expected in patients with RTLE (χ2=8.94; df=5; p=0.1). The maximum seizure frequency in all groups was observed from 12:00 to 16:00, the maximum seizure frequency recorded per hour block was 6 seizures per patient.
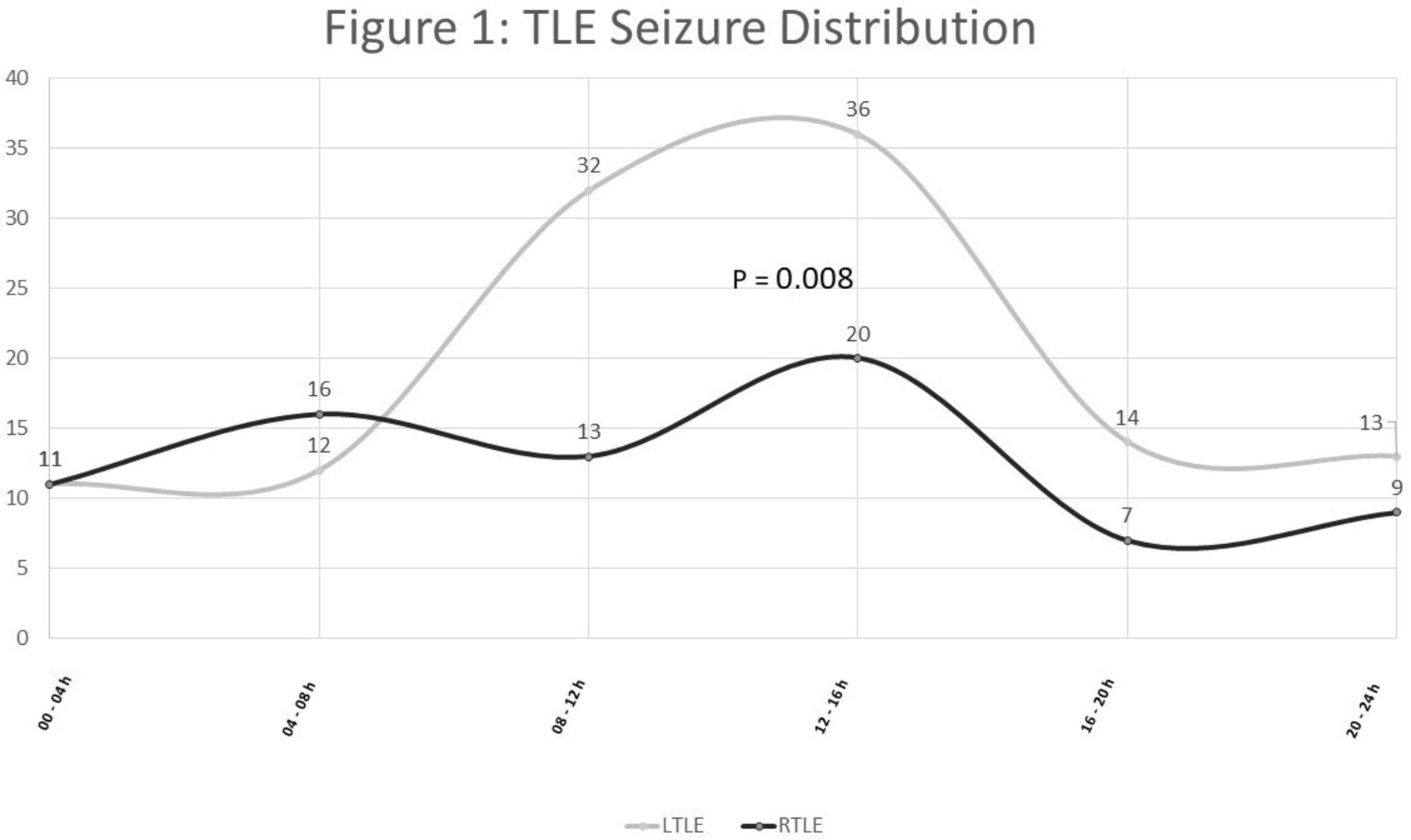
A different distribution of seizure frequency is observed, taking laterality into account, with a large peak between 08:00 and 16:00 for LTLE. LTLE, left temporal lobe epilepsy; RTLE, right temporal lobe epilepsy.
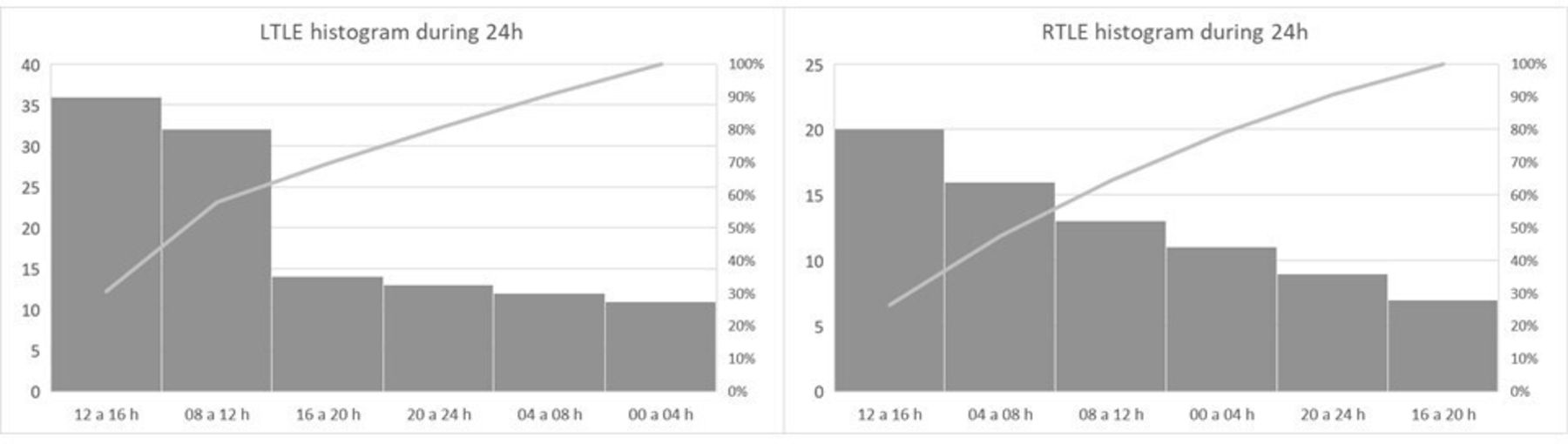
Seizure frequency analysis by time blocks. LTLE, left temporal lobe epilepsy; RTLE, right temporal lobe epilepsy.
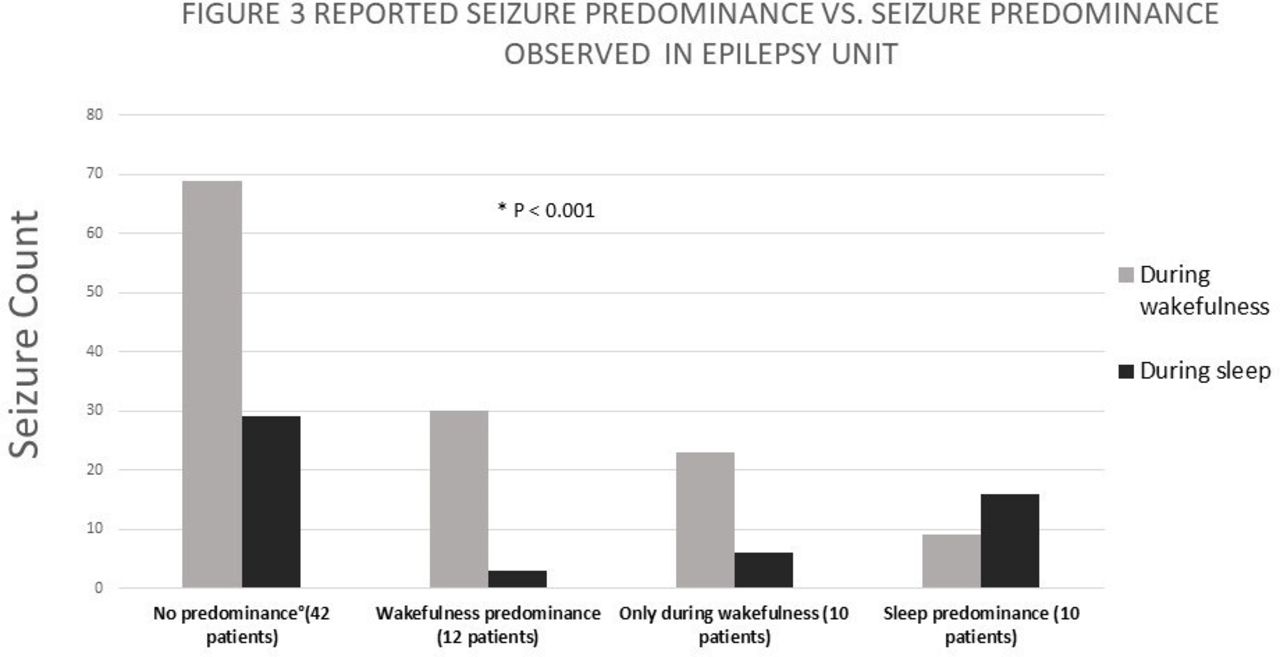
Seizure semiology analysis showed all seizures type were more frequent during wakefulness. Less than 10% of auras and focal aware seizures occurred during sleep, representing the T seizure types that least occur during sleep (table 4). There were no differences between right and left TLE. Four-hour period distribution showed less impaired awareness and focal to bilateral tonic–clonic seizures from 08:00 to 12:00 in RTLE patients (p=0.04). No other significative differences were found between right-sided and left-sided epilepsy (table 4). The relationship between the self-reported predominance of seizures and the results of VEEG recordings was also studied (see figure 3). Patients who did not report any clear predominance and patients who reported seizures during wakefulness had significantly more seizures during wakefulness (table 5) and patients who reported sleep predominance had more seizures during sleep (p>0.001).
{kind=link}
{kind=link}
{kind=link}
Comparison between the self-perception of patients about the moment of occurrence of seizures according to the sleep–wake cycle and seizures recorded in VEEG.
Seizure semiology analysis
Reported seizure predominance versus seizure occurrence observed in epilepsy unit
Discussion
This was a prospective study of adult patients with drug-resistant TLE carried out in a controlled environment to study the impact of the daily rhythms, seizure frequency and seizure occurrence over 24 hours. In summary, the 24-hour seizure distribution, during the VEEG, showed an increase in seizure frequency from 08:00 to 16:00 for all seizures. In patients with LTLE, the peak of seizures from 08:00 to 16:00 is significantly higher. Sleep-related parameters analysis showed that the most meaningful finding was that patients with RTLE significantly presented morning chronotypes. Antiseizure drugs analysis showed worst sleep quality in patients treated with benzodiazepines.
Regarding self-reported seizure occurrence, half of the patients could associate the occurrence of their seizures with a specific phase of the sleep–wake cycle. No patient or family reported seizures only during sleep, although during our study, eight patients (10.3%) only had seizures during sleep, which may have been due to hospitalisation.
Antiseizure treatment analysis showed that 45.9% of the patients were on two drugs and 32.4% were on three drugs. Drugs with known hypnotic effects, such as benzodiazepines and barbiturates, were considered, especially due to their effect on the sleep–wake cycle, as modifying the sleep architecture, and we observed the worst sleep quality (PSQI) in patients treated with benzodiazepines.6
PSQI showed a slight alteration in all patients, and the Epworth Scale showed that about half of the patients experienced mild daytime sleepiness. These observations are in agreement with another study that showed similar results in patients with epilepsy.13
Chronotype analysis (MEQ) revealed that more than half of the patients had an intermediate chronotype, followed by 22.2% with the evening type and 23.3% with the morning type; similar results have been previously reported.13 Laterality analysis showed a stronger preference for morningness in RTLE patients.
We analysed the relationship between nocturnal/diurnal seizures and sleep quality, daytime sleepiness and chronotype and found no differences between patients with nocturnal or diurnal seizures.
The PSQI and Epworth Scale showed a positive correlation, suggesting that the alteration in sleep quality contributes to daytime sleepiness; however, MEQ showed a negative correlation with Epworth, suggesting that patients with evening-type chronotypes had more daytime sleepiness.
Regarding the time of seizure occurrence, most patients experienced seizures during day hours, between 08:00 and 16:00 (rush hour near noon). Our findings are consistent with other authors, all series describing a day peak in TLE.2–4 28 29 One of them describes a peak incidence at 15:00,3 the second one shows a higher frequency of seizure occurrence between 15:00 and 19:00,28 while an observational study reported TLE peak incidence from 11:00 to 17:00, and seizure distribution in TLE patients had a higher frequency of seizure occurrence in the afternoon.30 Other authors describe two peaks, one is the primary peak from 16:00 to 19:00 and the secondary peak is from 07:00 to 10:00.31 A study carried out on the paediatric population, which also analyses different types of seizures, found that temporal lobe seizures occur during wakefulness regardless of the time of day.32 Seizure types have been previously analysed in relation to time distribution, showing that auras, dyscognitive and hypomotor seizures occurred more often in wakefulness,3,2 results comparable to our findings. Patients with RTLE showed less impaired awareness and focal to bilateral tonic–clonic seizures from 08:00 to 12:00, we attribute this difference to the higher degree of altered consciousness described in patients with LTLE.33
Laterality analysis showed different seizure distributions between the LTLE and RTLE groups, LTLE patients had a daytime peak from 08:00 to 16:00 and the RTLE group had a more uniform distribution. Rhythms in epilepsy are complex factors for analysis because of the large number of variables that can modify internal oscillators. Studies of infradian and ultradian rhythms have gained relevance due to their long-term seizure records, and the use of the word ‘multidien’ has been suggested for rhythms that do not respect calendar frequencies.34 It has been hypothesised that differences in the functioning of clock genes (BMAL/CLOCK/Per/Cry) in several regions of the central nervous system could explain the differences in seizure timing in focal epilepsy.32 35 Li et al propose that CLOCK transcription factor is decreased in epileptogenic brain tissue samples, resulting in hyperexcitability of pyramidal neurons, specifying that rhythmicity of clock genes may vary in different brain tissues.36
Chronic EEG recording has allowed to study ultradian, multidien and circannual rhythms,3,7–39 however this technology is not the first option in patients with drug-resistant TLE, therefore there may be patient selection biases.
A recent distribution study performed in VEEG patients showed wakefulness predominance in mesial and lateral TLE, with different distribution and no laterality analysis,4,0 we think laterality must be further studied in seizure distribution with chronic EEG implantation and molecular testing.
Possible weaknesses of this work include the difficulty to study circadian rhythms in patients hospitalised for clinical reasons. We could not analyse circadian rhythms because we lacked some of the necessary resources to study it, we limited ourselves to study the 24-hour daily rhythm, since we could control light and darkness. VEEG unit is an unnatural environment that can influence habitual sleep and wake habits; however, our protocol explores several parameters related to the sleep–wake cycle and the relationship with epilepsy. However, the prolonged VEEG is still the study that best allows locating focal epilepsies, since the observation of the clinical and electroencephalographic characteristics is irreplaceable for the moment. Even though patients or their relatives referred no sleep disorders and during the evaluation in VEEG unit we have not observed paroxysmal sleep disorders, we have not performed polysomnography studies in this population, therefore is a limitation to our work. We have not been able to rule out confounding effect of coexisting sleep disorders.
Our findings could serve as a basis for therapeutic interventions, since understanding the rhythmicity of seizures could help establish chronotherapeutic strategies, prevention measures knowing the time of greatest seizure frequency, changes in the schedule for taking antiseizure medication, and improve the quality of life of patients. In conclusion, our population experienced mild alterations in sleep quality and mild daytime sleepiness, unrelated to the epilepsy type or seizure frequency. Those who were on treatment with benzodiazepines had the worst sleep quality and more daytime sleepiness. Patients with LTLE had more seizures between 08:00 and 16:00, while patients with RTLE had a uniform 24-hour distribution, showing a distinctive temporal seizure pattern for each group.
We expect that the present study will help clarify the occurrence of epileptic seizures over 24 hours in patients with drug-resistant epilepsy and contribute to the understanding of the daily rhythms in focal epilepsy.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by ethics committees of Ramos Mejía Hospital (Ciudad Autónoma de Buenos Aires, Buenos Aires, Argentina) and El Cruce Dr. Nestor C. Kirchner Hospital, Dictamen Fecha 29.08.2014. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank Dr Forcato Cecilia, ENyS, Consejo Nacional de Investigaciones Científicas y Técnicas, for reviewing the manuscript. The authors would also like to thank Editage (www.editage.com) for English language editing.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @manusefir
Contributors MFL, SK and ACA conceived of and planned the paper. MFL carried out analysis of the results and wrote of the manuscript, with input from SK And SO. All authors discussed the analysis and commented on the manuscript. MFL acts as guarantor for this work.
Funding This work was supported by the Consejo Nacional de Investigaciones Científicas y Técnicas (National Council for Scientific and Technical Research).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.