Article Text

Abstract
Introduction Haycocknema perplexum is an exceedingly rare cause of parasitic myositis endemic to Australia, more specifically, Tasmania and North Queensland. There is a paucity of literature regarding this diagnosis, with only nine previously described cases.
Diagnosis This report details two cases of biopsy-confirmed H. perplexum myositis from Townsville University Hospital and describes the first-ever case of subclinical infection. There is limited known information regarding the H. perplexum life cycle and a definitive host which has hindered the development of a non-invasive diagnostic test. A review of the previously described cases has identified the hallmark features of this enigmatic condition: a triad of serological markers including deranged hepatic function, persistent eosinophilia and an elevated creatine kinase.
Conclusions This report aimed to raise awareness of H. perplexum myositis and the possibility of subclinical infection, which suggests a protracted disease course. Further research is required to identify a non-invasive diagnostic test, given that early diagnosis and timely initiation of albendazole treatment may drastically limit patient disability.
- NEUROPATHOLOGY, MUSCLE
- NEUROMUSCULAR
- TROPICAL NEUROLOGY
- INFECTIOUS DISEASES
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Haycocknema perplexum is an exceedingly rare cause of parasitic myositis endemic to Australia with nine previously reported cases.
WHAT THIS STUDY ADDS
This report details two cases of biopsy-confirmed H. perplexum myositis from Townsville University Hospital and describes the first-ever case of subclinical infection. A review of the previously described cases has identified the hallmark features of this enigmatic condition: a triad of serological markers including deranged hepatic function, persistent eosinophilia and an elevated creatine kinase.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
This report aimed to raise awareness of H. perplexum myositis and the possibility of subclinical infection, which suggests a protracted disease course. Further research is required to identify a non-invasive diagnostic test, given that early diagnosis and timely initiation of albendazole treatment may drastically limit patient disability.
Case Presentation
Case 1
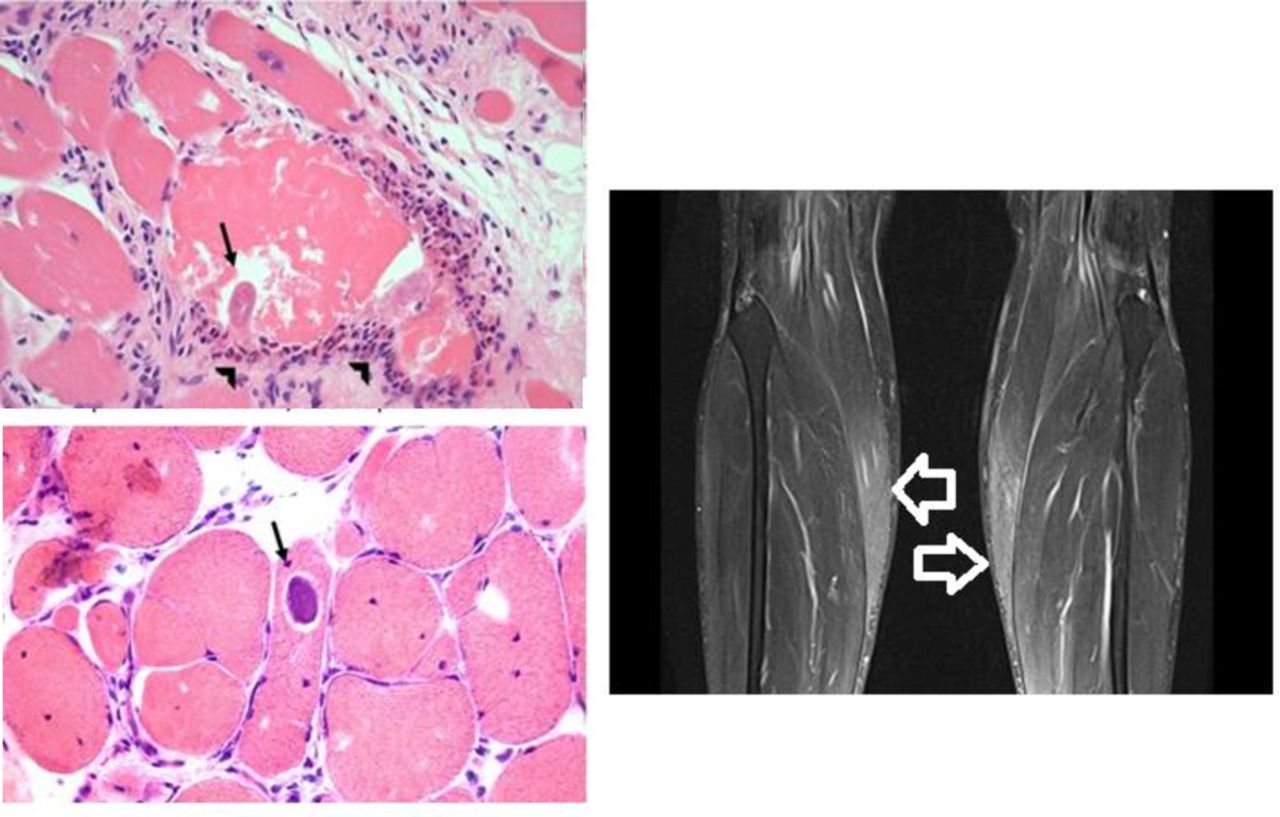
A man in his early 40s presented to the neurologist for assessment of musculoskeletal lower back pain following a workplace incident. The patient had no significant medical history and was taking no regular medications. He was found to have an elevated creatine kinase (CK) level of 2300 (normal range 45–250 U/L), mildly deranged liver function tests (LFTs) depicting a transaminitis with an aspartate aminotransferase (AST) of 65 (normal range 10–40 U/L) and alanine aminotransferase (ALT) of 94 (normal range 5–40 U/L), and a persistent eosinophilia between 2 and 3 (normal range 0–0.6 10∧9 /L), dating back to 2017. He had previously seen a dermatologist and an immunologist for investigation of his raised eosinophil count with ultimately no confirmation of the cause for his raised eosinophils. Strongyloides is another nematode endemic to North Queensland that causes a peripheral eosinophilia but has no association with myositis or reported muscular invasion; notably, faecal testing was performed in this patient and the results were negative. There were no constitutional symptoms, weakness, muscle pain or bulbar dysfunction. With regard to exposure history, the patient had travelled to Tasmania in his youth but otherwise lived in North Queensland with no overseas travel. He had consumed bush meat a few years previously on a deer hunting trip but otherwise was not an avid bushwalker and had no other history of wildlife exposure. Clinical examination of the cranial nerves and upper and lower limbs was normal. Repeat review with further serological testing confirmed ongoing raised CK levels despite avoiding strenuous activity over the preceding week. The myositis antibody panel and 3-hydroxy-3-methylglutaryl-CoA reductase antibody tests were negative. Needle electromyography was performed and demonstrated increased spontaneous muscle activity in the lower limb muscles bilaterally. MRI displayed bilateral, symmetric, calf muscle signal change without fatty atrophy. The patient proceeded to have a quadriceps muscle biopsy which confirmed H. perplexum myositis, demonstrating the visualisation of the sarcoplasmic parasite in cross-section along with the infiltrate of eosinophils, macrophages and multinucleated giant cells (figure 1). The patient was commenced on oral albendazole 400 mg two times per day and remained asymptomatic with no adverse affects to therapy. Notably, within 1 month of albendazole commencement, there was normalisation of the patient’s CK level, LFT derangement and eosinophilia.
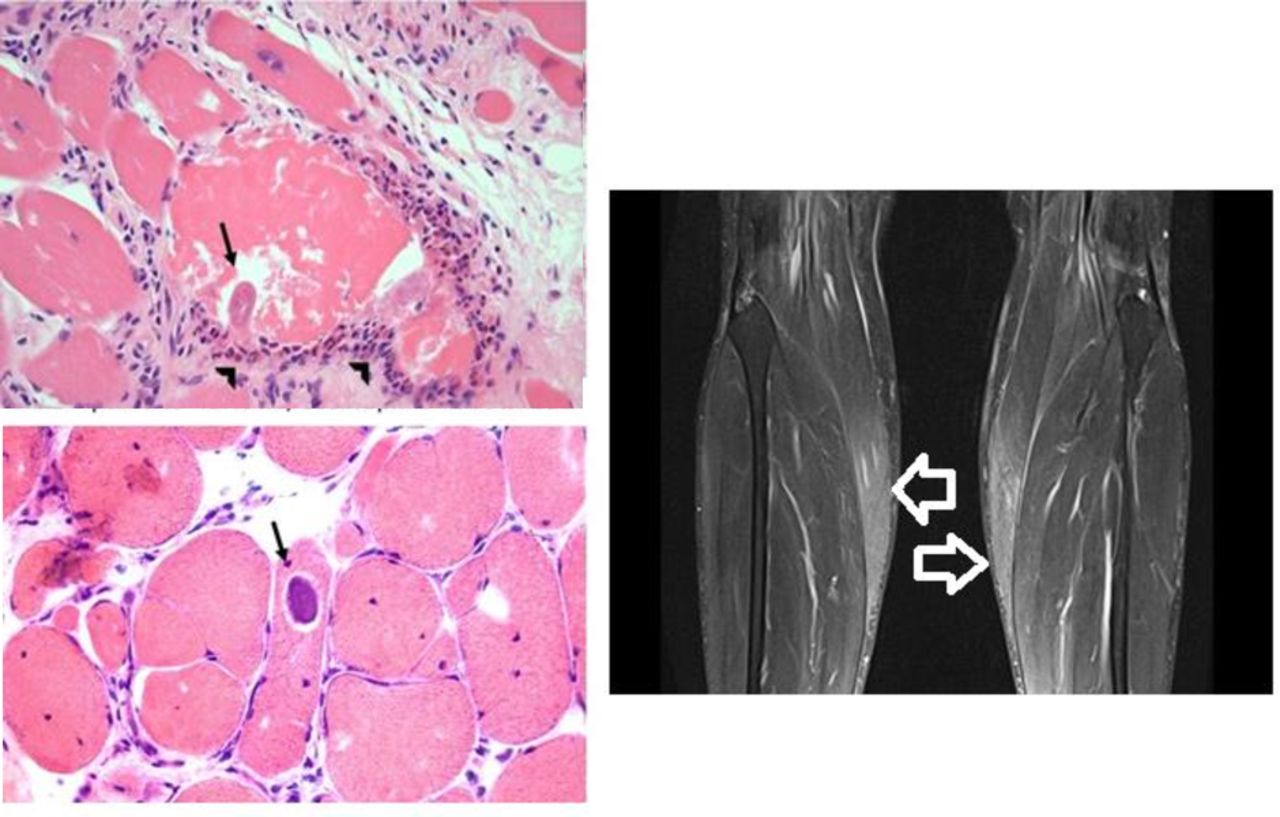
Intrasarcoplasmic parasites with interstitial eosinophilic infiltration evidenced on H&E staining (left; parasite depicted with arrows and eosinophils with arrowheads). MRI shows oedema characterised by high T2 signal in calf muscles bilaterally (signal change indicated with white arrows).
Case 2
A woman in her late 20s in her first trimester of pregnancy presented to the neurologist with a 3-year history of progressive symmetrical muscle weakness. The patient was premorbidly active and physically fit, her new progressive weakness causing her to withdraw from Muay Thai combat. The patient had no other significant medical history apart from long-standing hepatic dysfunction dating back a decade with a stagnant transaminitis; AST 50–80 (normal range 10–40 U/L) and ALT 45–95 (normal range 5–40 U/L). She had undergone previous extensive gastrointestinal investigations including hepatic biopsy, which failed to yield a diagnosis. The patient was noted by the treating neurologist to have a raised CK level of 3162 (normal range 45–250 U/L), along with an eosinophilia of 1.9 (normal range 0–0.6×109/L), which dated back to 2012. There was a history of 5 kg unintentional weight loss over the preceding 6 months with no other constitutional symptoms. There was no history of bush meat consumption or wildlife exposures. The patient had lived in North Queensland for most of their life with a few years spent in Brisbane and no interstate travel; the only overseas destination was Thailand 3 years ago. Clinical examination revealed normal cranial nerve function with neck flexion weakness and symmetrical proximal upper limb weakness and distal lower limb weakness. The neurological assessment was otherwise normal with no fatiguability nor evidence of bulbar dysfunction. Repeat review with serological testing confirmed a persistently raised CK level and eosinophilia. Myositis antibody panel was negative, along with genetic testing for facioscapulohumeral dystrophy, acid maltase testing and a second-generation neuromuscular genetic screening panel. Electrodiagnostic testing, neuroimaging and muscle biopsy were pursued with a conscious decision to avoid steroid use, common practice for empirical treatment of inflammatory myositis. Neurophysiological testing demonstrated evidence of myopathy with diffuse spontaneous activity on needle electromyography (EMG). There were no MRI features of myositis on imaging of the neck and upper limb girdle. Muscle biopsy of the quadriceps was undertaken and the diagnosis of H. perplexum myositis was confirmed with visualisation of the nematode on microscopy and evidence of an eosinophilic predominant inflammatory myositis (figure 2). The patient has been commenced on albendazole therapy, which has been deemed safe in her first trimester of pregnancy and at the point of this report’s submission remains stable with no adverse effects to therapy.

Intrasarcoplasmic parasites on H&E, acid phosphatase and PAS staining. Brown haemozoin-like pigment that is sometimes encountered in transverse sections of parasites is visible in the acid phosphase preparation. PAS, periodic acid–Schiff.
Discussion
Parasitic myositis is typically reported to be associated with protists, flatworms or roundworms (nematodes).1 2 Common nematodes recognised for causing myositis are the Toxocara and Trichinella species. Recently, H. perplexum, a nematode endemic to Australia, has been recognised as an exceedingly rare cause of parasitic myositis, which can be severely disabling and even life-threatening.3 A parasitic myositis is suggested by an appropriate geographical and pathogen exposure history in the presence of a peripheral eosinophilia. Despite some variability in the clinical presentation among the different parasites, a definite diagnosis ultimately depends on the specific pathogen diagnostic test; for example, this would be the demonstration of the characteristic microscopic parasite size and intra-sarcoplasmic location without encysted tissue forms in H. perplexum myositis or a positive ELISA for anti-Trichinella antibodies in trichinosis. H. perplexum myositis poses a significant diagnostic challenge, given the lack of physician awareness and literature surrounding its existence along with the absence of a non-invasive diagnostic test. H. perplexum myositis also clinically mimics polymyositis, often resulting in delayed diagnoses and inappropriate initiation of corticosteroid treatment.1 Steroids propagate parasitic reproduction and result in clinical deterioration.3 This report suggests that H. perplexum myositis has a subclinical infective state, which suggests a protracted disease course. We aimed to increase awareness of this enigmatic condition to prompt further research into H. perplexum with the goal to improve patient outcomes through early diagnosis and timely, appropriate therapy.
H. perplexum is a minute muspiceoid nematode of vertebrates which was first described by Dennett et al in 1998, when it was identified as the cause of human parasitic myositis.1 H. perplexum human infection has only ever occurred in Australia, more precisely, in Northern Australia and Tasmania.1–9 The zoonotic potential of H. perplexum remains a topic of speculation, with some literature supporting the theory that it is acquired through consumption of poorly cooked bush meats, as seen with other parasitic myopathies such as trichinosis and cysticercosis.2 Cutaneous penetration has also been considered as a means of human H. perplexum contraction, given there is evidence suggesting this mechanism of infection by other muspiceoid in koalas, mice, bats, kangaroos and wallabies.2 H. perplexum is a suspected human zoonosis, but the natural host remains unknown. H. perplexum reproduces efficiently hatching 8–12 infective larvae at a time which invade muscle cells and causes an eosinophilic polymyositis.1 2 7 Recent studies have suggested genetic markers with PCR-based DNA sequencing and next-generation DNA sequence analysis to assist with the diagnosis of H. perplexum, but speculation remains over the accuracy of this, given the limited case references.8 9 The gold standard of diagnosis remains the identification of the H. perplexum nematode on muscle biopsy8 (figure 3). The biopsy often demonstrates a patchy upregulation of major histocompatibility complex (MHC) class II in myofibre sarcoplasm and sarcolemma, as part of the inflammation. It is thought that the increased acid phosphatase is due to the lysosomes being overwhelmed by parasite proteins. Mild inflammation and eosinophil infiltration may also be seen in conditions such as calpainopathy (LGMD R1). Hence, histological identification of the parasite is crucial. The limited knowledge of the transmission and life cycle of H. perplexum hinders the development of a diagnostic serological assay and appropriate infection prevention guidelines, identifying a clear need for further research regarding this curious pathogen.

{kind=link}
{kind=link}
{kind=link}
Haycocknema perplexum demonstrated on skeletal muscle histology with acid phosphatase and MHC class I IHC. IHC, immunohistochemistry.
Although there is limited literature regarding this rare condition, we have reviewed the previous nine cases to determine the typical presentation and clinical features of H. perplexum myositis. An insidious onset of slowly progressive diffuse limb weakness is reflected in most cases with bulbar dysfunction presenting as dysarthria and dysphagia seen in 4/11 previously reported cases.1–9 Often, these are accompanied by constitutional symptoms, most notably, weight loss up to 18 kg.2 6 7 There are four described cases from Tasmania and seven from North Queensland.1–3 5–9 Some cases had extensive exposure to animals and wildlife (4/11), and others had consumption of bush meat (4/11), but no consistent exposure has been identified among the patient cohort.1–3 5–9 Along with an elevated CK, which was seen in all 11 cases, the other hallmark feature is a persistent eosinophilia that in most cases precedes the diagnosis, some by up to 10 years.1–3 5–9 The eosinophilia preceding clinical symptoms supports the suggestion of a subclinical infective period. Eosinophilia was absent in only one described case from Tasmania in 2011.6 Many cases also reported mild LFT derangements as seen with our patient, although not all case reports commented on the hepatic function and notably the transaminitis seen was disproportionate to the CK level.1–3 5–9
The recommended treatment, based off outcomes in the previous nine cases, is 3 months of albendazole (400 mg two times per day) therapy.1–3 5–9 Shorter duration of therapy was shown to result in progressive disease and need for treatment continuation.8 In most cases, there is moderate improvement with a persistent weakness likely reflective of the initial severity of infection and degree of established muscle damage and fibrosis. Five of 11 cases were initially treated with steroids for presumed polymyositis with a notable clinical deterioration and a fatal outcome, as in the case reported by Basuroy et al.5 This emphasises the importance of increasing awareness of H. perplexum myositis to prevent inappropriate steroid initiation and ensure early diagnosis to prevent severe disability.
Ultimately, the diagnosis of H. perplexum myositis is confirmed by muscle biopsy with microscopic identification of the non-encysted nematode. Each nematode is approximately 350 μm in length and 20 μm in width with a sharply tapered tail. Female worms within the muscle are often gravid.1 2 Table 1 details the clinical presentation, investigations and outcomes of the previous nine biopsy proven cases of H. perplexum myositis. This paper documents the 10th and 11th case and details the first patient with confirmed subclinical H. perplexum myositis infection. The inciting process which prompts progression to clinical disease remains unknown.
Summary of previously published cases of Haycocknema perplexum myositis along with the two newly described cases in this report: clinical presentation, laboratory findings and overall patient outcomes
Based on this case review, we propose that the diagnosis of H. perplexum myositis should be investigated in all patients presenting with the distinctive triad of persistent peripheral blood eosinophilia, elevated serum CK and hepatic derangement in the form of transaminitis. Although not specific for parasitic myositis, this proposed diagnostic triad should trigger consideration of diagnosis. There would be a higher clinical suspicion in patients with clinical features suggestive of myositis, including symmetrical weakness and muscle wasting along with bulbar dysfunction and constitutional symptoms and in those with the appropriate geographical exposure. We would also support investigation of asymptomatic patients presenting with features of the triad given our newfound knowledge of subclinical infection with H. perplexum, as described in case 1.
Conclusions
This report details the first-ever subclinical presentation of H. perplexum myositis and summarises the limited literature describing this enigmatic condition. We suggest that patients with the appropriate geographical exposure, presenting with the features of the proposed diagnostic triad—persistent eosinophilia, hepatic dysfunction and an elevated CK—be further investigated with muscle imaging and needle EMG in the first instance, even if asymptomatic. If the neuroimaging or electrodiagnostic testing suggests a myopathy, we recommend a muscle biopsy be pursued. Early recognition of H. perplexum myositis and initiation of appropriate therapy is essential in limiting ongoing disability. Moving forward, research should be geared towards developing non-invasive diagnostic testing for H. perplexum myositis and using it for further epidemiological prevalence studies.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but was not approved by an ethics committee or an institutional board. The study was deemed minimal risk; it involves information freely available in the public domain from other researchers, and the new data are properly anonymised with retrospective informed consent obtained at the time of original data collection.
Footnotes
Contributors KW completed the case summary and literature review. AK contributed to the literature review and editing. KRI, TR, RW and RU contributed expert opinion to the discussion and assisted with drafting of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.