Article Text

Abstract
Background There was no nationwide epidemiological study of Lambert-Eaton myasthenic syndrome (LEMS) in Japan; therefore, we conducted a nationwide survey.
Methods For the first survey, we sent survey sheets to randomly selected medical departments (n=7545) to obtain the number of LEMS who visited medical departments between 1 January 2017 and 31 December 2017. For the second survey, we sent survey sheets to the corresponding medical departments to obtain clinical information on LEMS.
Results We received 2708 responses (recovery rate: 35.9%) to the first survey. We estimated the number of LEMS as 348 (95% CI 247 to 449). The prevalence was 2.7 (95% CI 1.9 to 3.5) in 1 000 000 population. As a result of the second survey, we obtained 30 case records of 16 men and 14 women. Fourteen patients (46.7%) had a tumour, and 10 out of 14 tumours were small-cell lung carcinoma (71.4%). There was a predominance of men in the LEMS with tumour (paraneoplastic LEMS, P-LEMS) (n=11, 78.6%) and women in the LEMS without tumour (a primary autoimmune form of LEMS, AI-LEMS) (n=11, 68.8%) (p=0.0136). The onset age (mean (SD)) for the P-LEMS was 67.1 (9.0), and that for AI-LEMS was 57.8 (11.2) years old (p=0.0103). The disease duration (median) for P-LEMS was 2 years, and for AI-LEMS was 7.5 years (p=0.0134).
Conclusions The prevalence of LEMS in Japan is similar to that in other countries. There are predominances of men in P-LEMS and women in AI-LEMS.
- epidemiology
- clinical neurology
- neuromuscular
Data availability statement
Data are available upon reasonable request. Data are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The prevalence of Lambert-Eaton myasthenic syndrome (LEMS) was estimated at 2.5 in 1 000 000 in Netherland and 2.6 in US Veterans. More than 50% of LEMS had small-cell lung carcinoma (SCLC).
WHAT THIS STUDY ADDS
The prevalence of LEMS in Japan is estimated at 2.7 in 1 000 000. Of 46.7% of patients had tumours. About 33.3% of Japanese LEMS had SCLC. There were predominances of men in the LEMS with tumours (paraneoplastic LEMS, P-LEMS) (78.6%) and women in the LEMS without tumours (primary autoimmune form of LEMS, AI-LEMS) (68.8%). AI-LEMS had a significantly early onset. The median disease duration was significantly longer in AI-LEMS (7.5 years) than in P-LEMS (2 years).
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
The prevalence of Japanese LEMS is similar to those of other countries. Our result suggests that AI-LEMS has different immunological backgrounds from P-LEMS. Japanese patients with LEMS did not receive appropriate medical treatment, namely, lower subscriptions of 3,4-diaminopyridine and immunosuppressants, which should be improved.
Introduction
Lambert-Eaton myasthenic syndrome (LEMS) is an autoimmune disease that targets the P/Q-type voltage-gated calcium channel (VGCC) at the motor neuron terminal of the neuromuscular junction.1–3 The classical triad is proximal muscle weakness, decreased tendon reflexes and autonomic dysfunction.4 In addition, about 10% of patients show cerebellar signs almost exclusively related to small-cell lung carcinoma (SCLC).5 Historically, Drs Lambert and Eaton described patients having malignant tumours with unique electrophysiological findings.6 7 Myasthenia gravis (MG) also represents proximal muscle weakness; however, the targets of autoimmunity are molecules on the postsynaptic membrane.8 Electrophysiological testing is used to discriminate LEMS from MG.9 The anti-P/Q-type VGCC antibody is a diagnostic biomarker for LEMS and is positive in almost 90% of patients.10 Moreover, animal experiments found that patients’ IgG was pathogenic to mice’s skeletal muscle.11 12 Notably, SCLC is associated with LEMS with a frequency of 60%.13
An epidemiological study is a fundamental approach to understanding the aetiology of rare diseases. It also contributes to establishing healthcare policies for rare diseases of unknown aetiology. However, no nationwide survey has been performed for LEMS in Japan. Thus, we conducted a national study following a standard epidemiological protocol14 to estimate Japanese LEMS prevalence and clinical features.
Methods
Study design
We asked physicians at medical departments in Japan to fill survey sheets retrospectively based on the medical records. A task force of Validation of Evidence-based Diagnosis and Guidelines and Impact on Quality of Life in Patients with Neuroimmunological Diseases from the Ministry of Health, Labour and Welfare (MHLW) of Japan designed the diagnostic criteria of LEMS (online supplemental table S1). The Japanese Society of Neurology approved the diagnostic criteria in 2019. The study group followed the Survey Manual of Study on Epidemiological Data Collection and Intractable Diseases from the MHLW, third edition.14 In addition, this study was performed in parallel with a nationwide survey of MG in Japan funded by MHLW. We summarise the flow of the study in figure 1.
Supplemental material

Flowchart of the epidemiological study of LEMS 2018. The study comprises the first study and the second study. LEMS, Lambert-Eaton myasthenic syndrome.
Protocol approvals, registrations and patient consent
The study centre was performed at the Health Service Center of Kanazawa University (Kanazawa, Japan). We asked physicians at medical departments to fill the survey sheets retrospectively based on the patient records. The correspondence tables of the patients were stored in medical departments. Therefore, the study centre did not know the patients’ identities. Because the study was retrospective and collected patient records that did not include their identities, written informed consent from patients was waived. Instead, we provided posters to the medical departments, which announced the ongoing study and allowed patients to not be included in the survey.
The first survey
We performed the first survey to estimate the prevalence of patients with LEMS. According to the MHLW, the total number of medical institutions in Japan in 2017 was 8445 (https://www.mhlw.go.jp/toukei/saikin/hw/iryosd/17/). Online supplemental table S2 shows the number of medical departments that were investigated. From these departments, our sample consisted of: 100% of university hospitals, 100% of hospitals having more than or equal to 500 beds, 80% of hospitals having 400–499 beds, 40% of hospitals having 300–399 beds, 20% of hospitals having 200–299 beds, 10% of hospitals having 100–199 beds and 5% of hospitals having less than or equal 99 beds. We also selected four hospitals that specialised in neuroimmunological diseases. One of the authors (YNa) selected the candidates randomly and prepared the list of departments. The total number of departments that received the survey sheet by 30 March 2018 was 7545. The survey sheet was used to assess the number of LEMS (outpatients and inpatients) that visited the medical departments between 1 January 2017 and 31 December 2017.
The second survey
We sent the second survey sheet and correspondence table to the medical departments that responded to the first survey. The documents included anonymous case records that requested clinical information of patients diagnosed with LEMS. In addition, the second sheet included questions about patient symptoms, examinations, clinical severities, therapies and other information (online supplemental table S3). The correspondence tables of the secondary survey were stored in medical departments. Therefore, the data used were deidentified and anonymised before we had access. We checked the duplication of data manually. We also removed incomplete patient’s record manually.
Data analysis
We estimated the number of patients by the formulae indicated in the survey manual.14 In addition, we calculated the prevalence rate per 100 000 using the Japanese population in 2017 reported by the Statistics Bureau of Japan (n=126 706 000; https://www.stat.go.jp/data/jinsui/2017np/index.html).
We used the Shapiro-Wilk test to evaluate the distribution of continuous data in this study. We used Student’s t test after examining equal variance to compare the means of two normally distributed data, Wilcoxon/Kruskal-Wallis test to compare the medians of two non-normally distributed data, and the χ2 test or Fisher’s exact test for categorical data. We used JMP V.16.1.0 (SAS Institute Japan) for the statistical analysis. Missing data were kept blank.
Results
First survey
Estimated number and prevalence of patients
We received 2708 survey forms from medical departments (percentage of replies: 35.9%). As a result, the number of LEMS patients for 2017 was 348 (95% CI 247 to 449). The prevalence of patients was 2.7 (95% CI 1.9 to 3.5) in 1 000 000 population.
Second survey
We obtained 30 clinical records from medical departments (figure 1) consisting of 16 men and 14 women (men:women ratio=1:0.88). The mean (SD) of the onset age of total patients was 62.2 (11.1) years old. The mean (SD) onset age of the men was 63.3 (9.4) years old and that for the women was 60.9 (13.0) (p=0.5858, Student’s t test) (figure 2). The mean (SD) of onset age of patients with tumour was 67.1 (9.0) years old, and that for patients without tumour was 57.8 (11.2) years old (p=0.0103, Student’s t test) (figure 3).
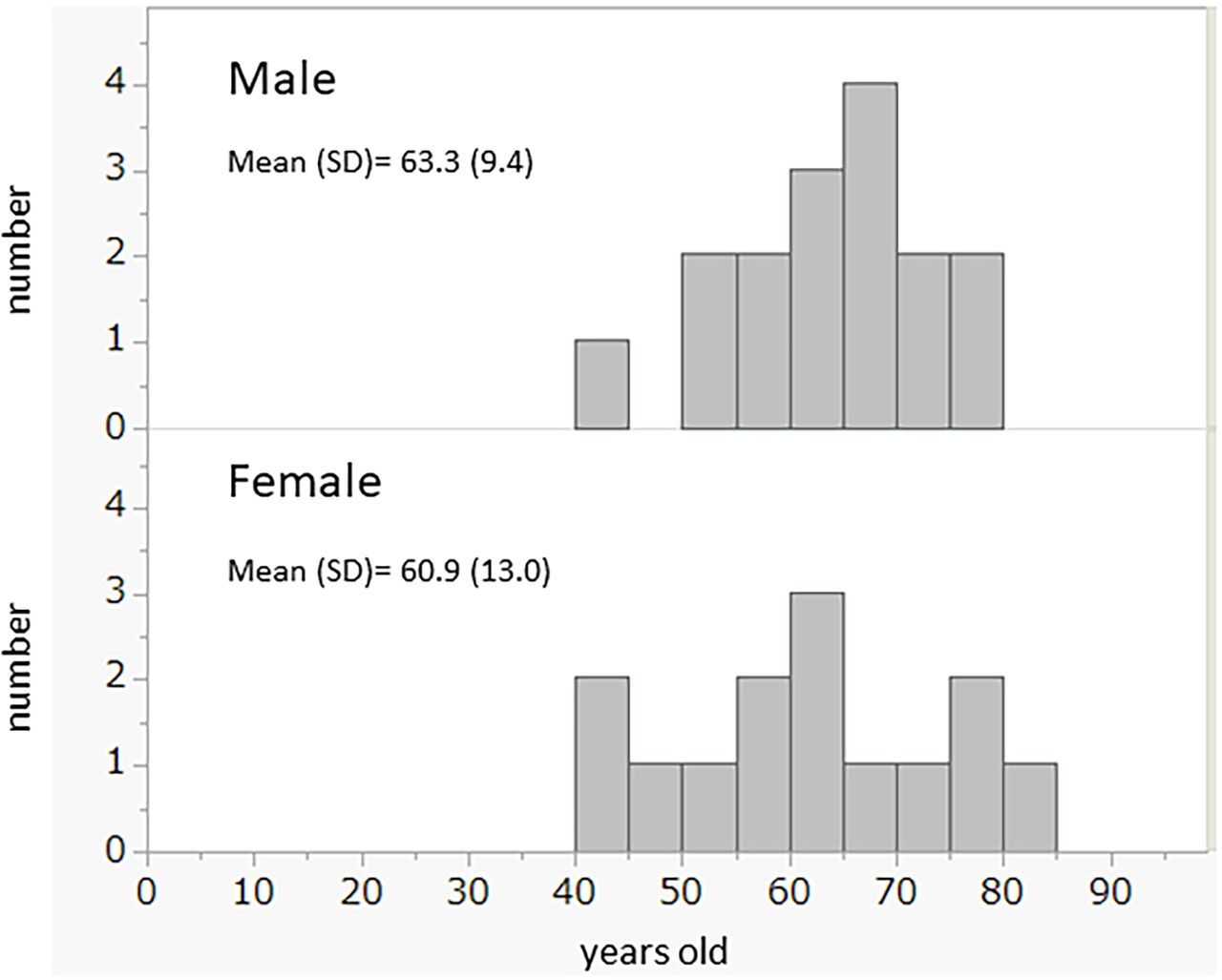
The onset age of patients. Complete analysis and the analyses by sex.
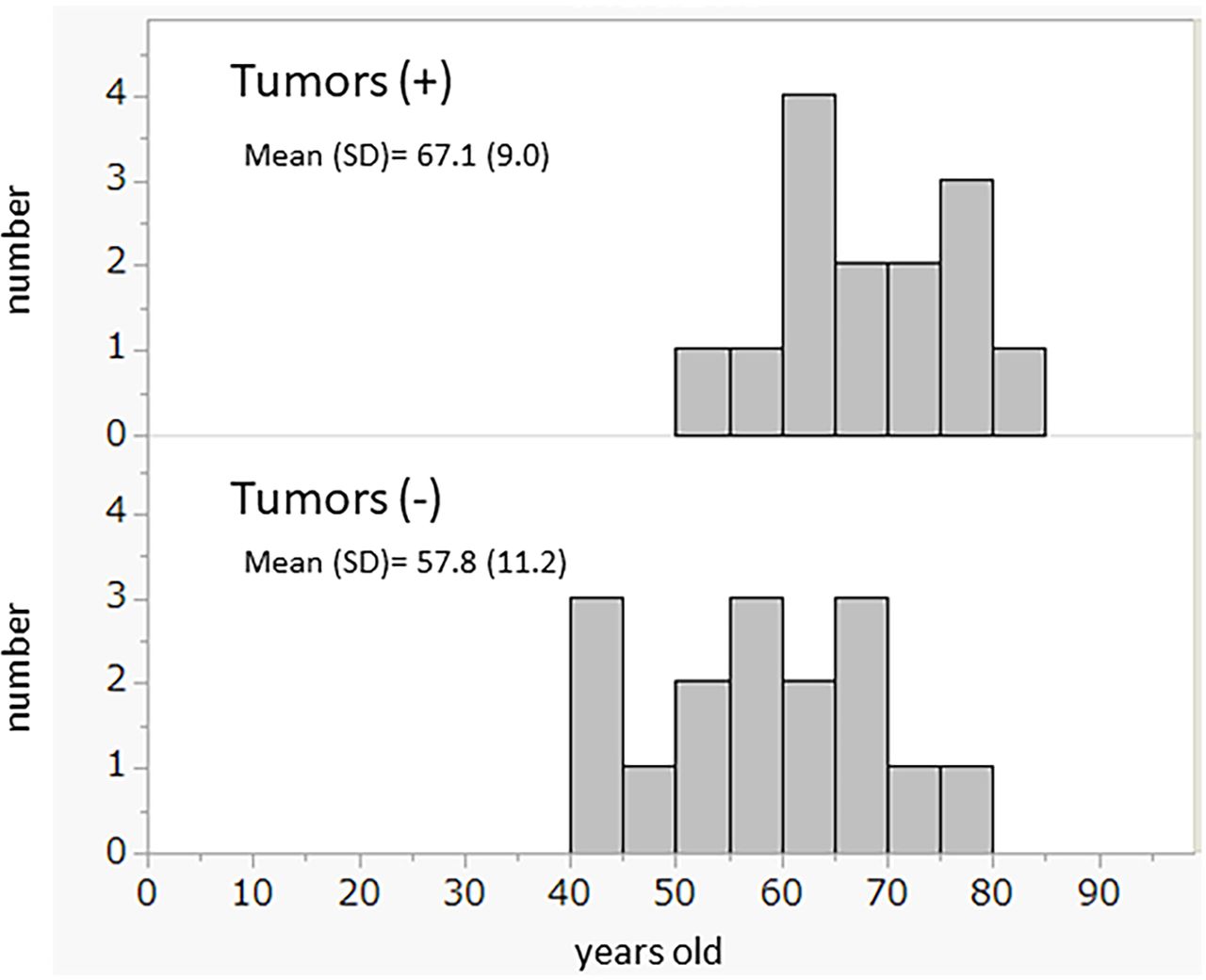
The onset age of patients with or without cancer. Patients with cancer were significantly older than those without cancer (Student’s t-test, p = 0.0103).
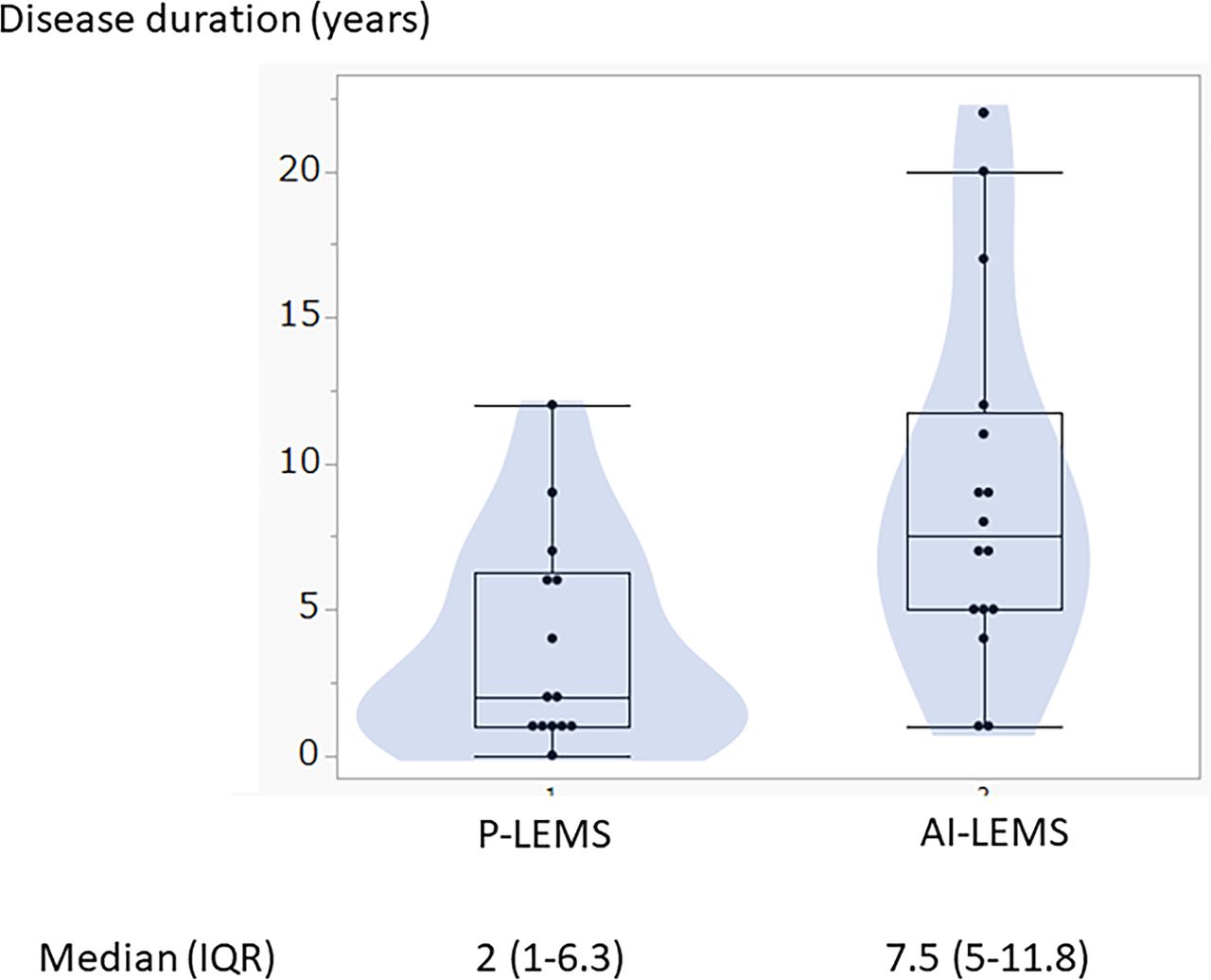
We compared the P-LEMS and AI-LEMS (table 1). Men were predominant in P-LEMS; on the other hand, women were dominant in AI-LEMS (p=0.0136, Fisher’s exact test). Disease duration was significantly longer in AI-LEMS than in P-LEMS (figure 4). The median (IQR) for AI-LEMS was 7.5 (5–11.8) and for P-LEMS was 2 (1–6.3) (p=0.0134). The patients’ symptoms at the time of the study were not different from those of the initial symptoms (online supplemental table S4). Complications of other autoimmune diseases were not remarkable.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disease duration (years) of P-LEMS and AI-LEMS. Overlapping of the box, scatter and violin plots. The disease duration of AI-LEMS was significantly longer than P-LEMS (Wilcoxon/Kruskal-Wallis test, p=0.0134). LEMS, Lambert-Eaton myasthenic syndrome; P-LEMS, paraneoplastic LEMS; AI-LEMS, a primary autoimmune form of LEMS.
Symptoms and background information of LEMS patients with or without tumour
SCLC was found in 71.4% of tumours (10/14). A family history of LEMS was absent. However, one patient had Hashimoto’s disease as a complication and a family history of Hashimoto’s disease in her sister and aunt.
A total of 21 (84%) patients were positive for anti-P/Q-type VGCC antibody (positive: 21/tested: 25) (table 2). There was no significant difference in the positivity ratio for this autoantibody between P-LEMS and AI-LEMS (table 2). The frequency of cerebellar signs was similar between the groups, almost identical to a previous report.15 The titres of the anti-P/Q-type VGCC antibody were not different between P-LEMS and AI-LEMS. Electrophysiological tests were also frequently positive in both groups. However, there was no difference in the positive percentile of laboratory tests between P-LEMS and AI-LEMS.
Laboratory tests of LEMS patients with or without tumour
Table 3 shows the patients’ therapeutic status. AI-LEMS tended to receive 3,4-diaminopyridine (3,4-DAP) frequently. However, overall usage of 3,4-DAP was limited. Prednisolone (PSL) usage was lower in P-LEMS; however, the frequency was not significantly different. Four (25%) AI-LEMS received immunosuppressants (azathioprine, tacrolimus). The plasmapheresi was frequent adjunctive therapy. The length of hospital stay was not different between P-LEMS and AI-LEM (table 4). However, the modified Rankin scale was significantly higher in P-LEMS. No patients died of LEMS; however, four patients died of tumor-associated causes.
Therapies of LEMS patients with or without tumour
Prognosis of LEMS patients with or without tumours
Discussion
This study was the first nationwide epidemiological survey of LEMS in Japan using a survey manual. The prevalence of LEMS was similar to previous reports from other countries. An epidemiological study from the Netherlands in 2004 by Wirtz et al reported a prevalence of LEMS (95% CI) of 2.5 (1.8–3.4) in 1 000 000 population.16 Moreover, Abenroth et al reported a prevalence of 2.6 per 1 000 000 (confirmed cases) in the US Veterans Affairs population.17 The prognosis in SCLC is poor, and median survival without treatment has been reported as 2–4 months.18 Therefore, our methodology may have a lower prevalence estimation.
LEMS is classified into two categories: LEMS with tumour (paraneoplastic LEMS: P-LEMS) and LEMS without tumour (a primary autoimmune form of LEMS: AI-LEMS). Titulaer et al reported that 54% of patients with LEMS had SCLC.19 Moreover, studies reported that men were predominant in LEMS with SCLC.20–22 In the present study, we found SCLC in 10 out of 30 patients with LEMS (33.3%), and 80% of patients with SCLC were men. A previous study with a larger sample size (n=97 patients) by Titulaer et al5 reported that the median age at onset of P-LEMS (with SCLC) was 59.5 years old, and that of AI-LEMS was 54 years old. On the other hand, our study indicated a significantly younger onset age in AI-LEM. A previous study reported a significant predominance of males in P-LEMS, and that the men and women ratio was similar in AI-LEMS.5 However, the present study showed male predominance in P-LEMS and female predominance in AI-LEM. In Japan, overall smoking prevalence (25–64 years) decreased from 56.0% to 38.4% among men and 17.0% to 13.0% among women from 2001 to 2016.23 Therefore, the proportional changes in sex in P-LEMS and AI-LEMS might be attributed to the demographic change in the smoking population, a primary risk factor for SCLC. In addition, LEMS often manifested prior to SCLC diagnosis. Therefore, we have to follow AI-LEMS up for SCLC for years. LEMS is strongly associated with SCLC. We found four patients of LEMS had tumours other than SCLC (aggressive fibromatosis, oropharyngeal endocrine tumour, mixed tumour of lung (squamous cancer and mucinous adenocarcinoma), lung cancer suspected). We cannot exclude the possibility of coincidence of these tumours with LEMS.
Our diagnostic criteria for LEMS followed Titulaer et al,4 modifying the 60% increment rate of compound muscle action potentials (CMAPs) after maximum voluntary contraction or at high frequency (50 Hz), as Oh et al proposed a 60% increment of CMAP as the diagnostic criteria to include seronegative LEMS.24 Sixty per cent increment of CMAP includes false-positive diagnosis; however, a cut-off of 100% improves specificity at the expense of sensitivity. Therefore, we have to consider the appropriate cut-off for increment. The proximal muscle weakness in AI-LEMS was 81.3% in initial symptoms. However, we did not exclude 18.7% of patients from the diagnosis of LEMS. This diagnostic policy is because we could not see the patients nor check every patient’s medical record. Therefore, we admit that the diagnostic process allows individual biases of physicians. According to our diagnostic criteria, the definite LEMS was 16, and the probable LEMS was 4 out of 30 patients.
Our study did not find any differences between P-LEMS and AI-LEMS in frequencies of initial symptoms, current symptoms, cerebellar ataxia, anti-P/Q-type VGCC antibodies and electrophysiological findings. In the present study, the two groups shared similar clinical and laboratory findings; thus, our findings suggest the necessity of radiological examinations to identify tumours in patients with LEMS. On the other hand, the sex ratio and onset ages differed between P-LEMS and AI-LEMS; thus, there may be some aetiological differences between these two conditions.
There were no statistical differences in the selection of medicines between the LEMS with tumour and without tumour groups. However, overall usage of 3,4-DAP was limited compared with previous reports.25 In Japan, there is no available medicine for 3,4-DAP. Therefore, we must use a chemical reagent of 3,4-DAP to treat LEMS after a particular application and approval. The lack of commercially available medicine prevents physicians from subscribing to 3,4-DAP for patients with LEMS. Therefore, we have to change this situation. We also noticed that the use of PSL and immunosuppressant is few in P-LEMS. We think that was because of the reported improved survival of SCLC with LEMS compared with SCLC alone.26–28 As P-LEMS was more severe symptoms than AI-LEMS, we could treat P-LEMS more aggressively.
The limitation of this study was the relatively small number of recovery in the second survey after the first survey (30/348, 8.6%). In addition, this study is the first nationwide epidemiological study; therefore, we have no data to compare in Japan. Therefore, we should repeat the nationwide study periodically. Before this study, we established the diagnostic criteria and the classification of disease severity, contributing to this study’s reliability. Our survey is based on the patients with LEMS who visited the medical departments from 1 January 2017 to 31 December 2017. Therefore, there is a possibility that we missed deceased patients of P-LEMS in this study, and those affected our P-LEMS estimation with our methodology.
This study revealed the clinical features of LEMS in Japan. In addition, a nationwide periodical survey will contribute to understanding LEMS and help improve the treatment and welfare of patients.
Data availability statement
Data are available upon reasonable request. Data are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The Kanazawa University Medical Ethics Committee approved the study protocol (2017–292).
Acknowledgments
We thank physicians in the medical departments at the hospitals who kindly answered our survey sheets. We also thank the Health Service Center Kanazawa University staff for their support in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators Members of Taskforce of Validation of Evidence-based Diagnosis and Guidelines, and Impact on Quality of Life (QOL) in Patients with Neuroimmunological Diseases are as follows; Satoshi Kuwabara (Chiba University), Yuishin Izumi (Tokushima University), Noriko Isobe (Kyushu University), Uzawa Akiyuki (Chiba University), Mieko Ogino (International University of Health and Welfare), Kenichi Kaida (Saitama Medical University), Izumi Kawachi (Niigata University), Haruki Koike (Nagoya University), Yasunori Satou (Keio University), Yuko Shimizu (Tokyo Women’s Medical University), Masahiro Sonoo (Teikyo University), Hideyuki Takeuchi (Yokohama City University), Masayuki Tawara (National Hospital Organization Utano National Hospital), Ichiro Nakajima (Tohoku Medical and Pharmaceutical University), Yuji Nakatsuji (Toyama University), Emi Nakanishi (Kanazawa Medical University), Jin Nakahara (Keio University), Masaaki Niino (Hokkaido Medical Center), Kazuo Fujiwara (Institute for Neurological Disorders), Sonoko Misawa (Chiba University), Hiroyuki Murai (International University of Health and Welfare), Masakatsu Motomura (Nagasaki Institute of Applied Science), Takashi Yamamura (National Center of Neurology and Psychiatry), Takanori Yokota (Tokyo Medical and Dental University), Hiroaki Yoshikawa (Kanazawa University), Makoto Matsui (Kanazawa Medical University).
Contributors HY, YNa, NK, HM and MM contributed to the conception of the work. HY, HM, YNo, YS, KI, YF, SK and MM contributed to the data acquisition. HY and YA contributed to analysing and interpreting data for the work. HY contributed to drafting the work. All authors revised the manuscript critically for important intellectual content and contributed final approval of the version to be published. MM and SK are the guarantors for the overall content.
Funding This study was supported (in part) by a Health and Labour Sciences Research Grant on Rare and Intractable Diseases (Validation of Evidence-based Diagnosis and Guidelines, and Impact on QOL in Patients with Neuroimmunological Diseases) from the Ministry of Health, Labour and Welfare of Japan (Grant number: 20FC1030).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.