Article Text

Abstract
Background: Rapid reperfusion in ischaemic stroke with emergent large vessel occlusion (ELVO) reduces morbidity and mortality. Limited distribution of endovascular clot retrieval (ECR) capable comprehensive stroke centres (CSCs) necessitates development of pre-hospital models of care to provide equitable and economical access to reperfusion therapy. We examine the time metrics of the traditional secondary transfer strategy in comparison to the direct bypass strategy and the potential utility of the ACT-FAST prehospital triage algorithm on a large volume Melbourne primary stroke centre (PSC).
Method: Retrospective analysis of consecutive patients presenting to a PSC from 1 January 2020 to 31 December 2020. Clinical records were interrogated for ACT-FAST positive patients. Time metrics were established using Google Maps traffic modelling and local/published door-to-needle, door-in-door out and door-to-groin data.
Results: 88 patients during the study period were ACT-FAST positive. Of these, 49/88 (56%) cases had ELVO ischaemic strokes, 24/88 (27%) cases had intracranial haemorrhages and the remaining 15/88 (17%) had non ELVO ischaemic strokes or mimics (seizure, complex migraine, etc). 28/88 (32%) cases met indication for and were subsequently transferred to a CSC for consideration of ECR. The modelled median scene to groin time for the direct bypass strategy is 94 min whereas the median scene to groin time for the secondary transfer strategy is 109 min, giving a difference of 15 min.
Conclusion: Time savings to groin puncture for the direct bypass strategy is substantially less than previous estimates and suggests that the secondary transfer strategy continues to be a viable pathway for a high efficiency PSC.
- stroke
- cerebrovascular disease
- health economics
- health policy & practice
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Access to reperfusion therapy, in particular endovascular clot retrieval, is limited. Prehospital models of care are being continuously revised to optimise access to therapy while maintaining cost-effectiveness.
WHAT THIS STUDY ADDS
This study highlights the three models of care currently available in Melbourne, Australia and examines the hypothetical effect of pre-hospital paramedic triaging at a high efficiency primary stroke centre (PSCs). It finds a majority of patients do not benefit from direct bypass to a comprehensive stroke centre and the delay to groin access for endovascular clot retrieval at our centre is much less than previously suggested in previous studies.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study suggests that secondary transfer is still a viable pathway if workflows are optimised to reduce door-in-door out times. There remains a considerable role that high performing PSCs can play in the overall stroke systems of care.
Background
Time is brain. Although intravenous thrombolysis is widely available at primary stroke centres (PSCs), the availability of endovascular clot retrieval (ECR) is limited to a few comprehensive stroke centres (CSCs) located in the major capital cities of Australia. This necessitates interhospital transfer of emergent large vessel occlusion (ELVO) patients both in the metro and regional settings to these CSCs for ECR.
Currently, there are three distinct pathways an ELVO stroke patient within metropolitan Melbourne may arrive at a CSC. First, and historically, all suspected stroke patients are initially transported for assessment at the nearest hospital from the scene with 24/7 thrombolysis service, regardless of PSC or CSC designation. These patients are then transferred to CSC for consideration of ECR if appropriate. Since late 2017, with the commission of the first Australian Mobile Stroke Unit Ambulance (MSU), a second option became available during 08:00–18:00 hours, Monday to Friday operating within 20 km from the city centre.1 Eligible patients are given intravenous thrombolysis on the MSU and if a ELVO is identified by the on-board CT angiography, transferred directly to a CSC. Finally, in 2019, a city-wide PSC bypass strategy was implemented by Ambulance Victoria using the ACT-FAST tool (figure 1). This pathway involved ACT-FAST positive patients being taken directly to the nearest CSC for assessment, bypassing PSC along the way.
The ACT-FAST tool is designed to identify patients with ELVO in the field using clinical features alone based on a three-step algorithm.2 The first step assesses for unilateral arm weakness using the NIHSS (National Institutes of Health Stroke Scale) method of arm drift and is fulfilled when one arm drifts to the stretcher in <10 s. The second step of ACT-FAST depends on which arm is weak. If the right arm is weak, paramedics are instructed to look for dysphasia. If the left arm is weak, paramedics are instructed to assess for left sided neglect. The third step is to determine eligibility for ECR therapy including that time of onset <24 hours, that deficits are not pre-existing, good premorbid functional level and to rule out common stroke mimics. A patient is considered ACT-FAST positive if a patient fulfils all three steps of the algorithm (figure 1).

ACT-FAST algotithm. BSL - Blood sugar level
The catchment area of the Eastern Health network—located in the east of Melbourne with Box Hill Hospital (BHH) as the network PSC was in principle not included in the ACT-FAST bypass strategy. We aim to examine the potential utility of the ACT-FAST prehospital triage tool in expediting treatment times and appropriately triaging suspected stroke patients in our catchment area.
Methods
Departmental stroke databases were interrogated for patients who presented via ambulance with ongoing neurological symptoms for stroke team assessment from 1 January 2020 to 31 December 2020. Patient medical records were reviewed by an acute stroke nurse to determine if they met ACT-FAST criteria based on paramedic or medical assessment. ACT-FAST diagnostic accuracy was then compared with CT-angiogram imaging for the presence of ELVO (ICA, M1, M2, basilar artery occlusion). Variables collected included: age, sex, postcode, premorbid modified Rankin score, presence and location of ELVO on CTA, hyperacute therapy received, door to needle time (DTN) and door-in-door-out (DIDO) times and discharge diagnosis.
Potential direct bypass strategy time savings were estimated using google maps-based traffic modelling. Using the postcode of each patient as the on-scene location reference, travel time to BHH and then onwards to the usual referral CSC (The Royal Melbourne Hospital) was compared with the travel time if the patient was transported direct to the nearest CSC (The Royal Melbourne Hospital or Monash Medical Centre). Travel times were modelled for both day and night-time traffic. The median time from these traffic models was then used for further analysis, representing an estimated median time saved regardless of the time of the day. Analysis was performed using Microsoft Excel 365 and Stata (V.17.0).
Results
Number of ELVO, non-ELVO ischaemic strokes, intracranial haemorrhage and mimics
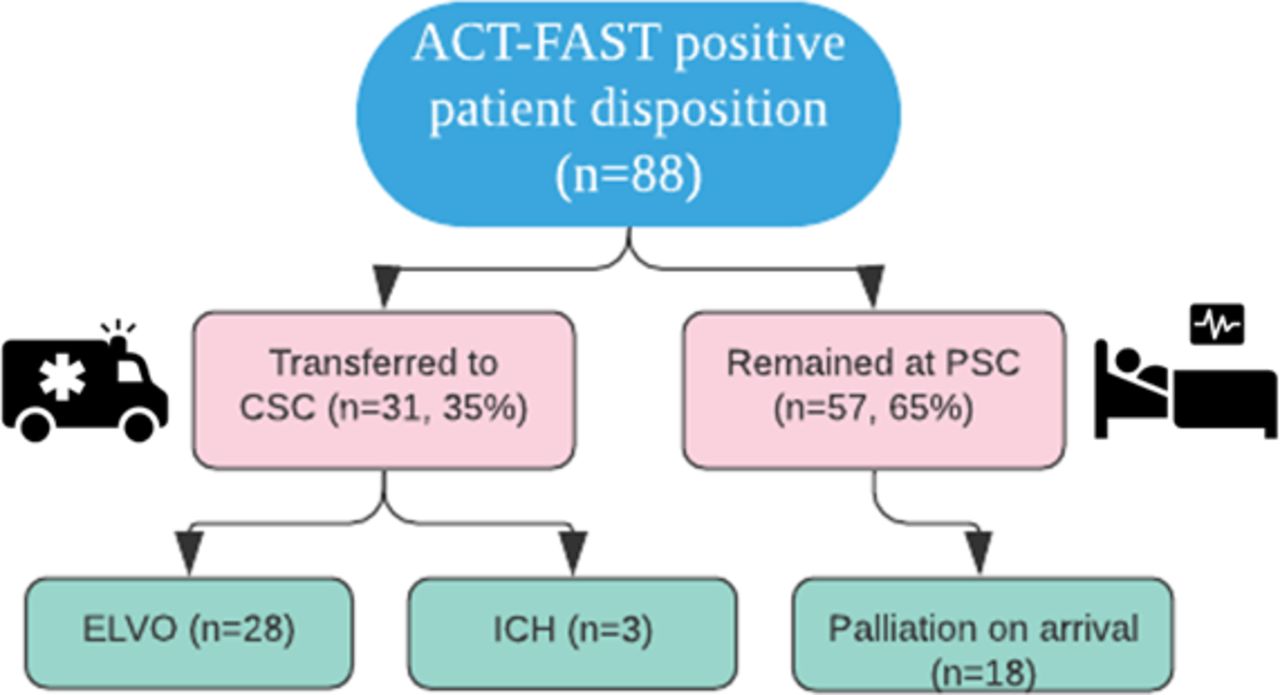
A total of 1216 presentations were included with 88/1216 (7%) presentations ACT-FAST positive (table 1). Of these, 49/88 (56%) cases had ELVO ischaemic strokes, 24/88 (27%) cases had intracranial haemorrhages (ICHs) and the remaining 15/88 (17%) had non EVLO ischaemic strokes or mimics (seizure, complex migraine or functional etc). Of 88, 28 (32%) cases met indication for and were subsequently transferred to a CSC for consideration of ECR. Four additional patients during the study period were ACT-FAST negative but had ELVO amendable to ECR, these were also transferred to a CSC for ECR. In total, 19/ (28+4) (59%) of ECR cases received thrombolysis prior to transfer. Of 88, 18 (20%) cases were palliated on arrival after clinical and neuroimaging assessment. Of the ICH cases, only 3/24 (12.5%) of these required transfer to a neurosurgical centre during their admission (figure 2).
Patient characteristics

Disposition flow chart of ACT-FAST positive patients. CSC, comprehensive stroke centre; ELVO, emergent large vessel occlusion; ICH, intracranial haemorrhage; PSC, primary stroke centre.
ACT-FAST had 92% sensitivity and 97% specificity for ELVO. Negative predictive value (NPV) was 99.7%, while positive predictive value (PPV) was 55.7%.
Where data were available, of 54 patients flagged as ACT-FAST positive by paramedics, as noted in ambulance documentation, 21 (40%) were in fact not positive based on step 3 eligibility criteria.
Time metrics
The median scene to BHH time in our cohort was 15 min (IQR 8.5–21). The modelled median time to transfer patients in our cohort directly from scene to the closest CSC (The Royal Melbourne Hospital or Monash Medical Centre) was 24 min (IQR 20–28).
The median DIDO time for ECR transfer, and door-to-needle (DTN) time were 50 min (IQR 41–63 min) and 45 min (IQR 35–62 min) respectively for this cohort. The median outbound transport time from BHH to The Royal Melbourne Hospital (the main referral CSC for our centre) was 20 min.
The time metrics used for comparison were derived from a consecutive sample of 460 ECR cases during the calendar years 2018–2019 (prior to the implementation of ACT-FAST triage bypass) from the two designated Victorian state-wide ECR centres (The Royal Melbourne Hospital and Monash Medical Centre). CSC-arrival-to-arterial-access times in direct-presenting patients is 70 min compared with 24 min for metropolitan secondary transfer patients.3 The discrepancy between the times is due to the fact that direct presentations still require a full workup including history, examination, multimodal CT imaging and activation of the catheter laboratory prior to ECR whereas secondary transfer patients can be taken directly to the preactivated catheter laboratory. BHH secondary transfer patients would fall under the subset of metropolitan secondary transfer patients.
Therefore, in the Eastern Health catchment area the median scene to groin time for the direct bypass strategy is 94 min (Transfer time from scene to nearest CSC of 24 min+door to groin time of 70 min). The median scene to groin time for the secondary transfer strategy is 109 min (Transfer time to BHH of 15 min+median DIDO of 50 min+BHH to CSC transfer time of 20 min+door to groin time of 24 min) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Comparison of direct bypass and secondary transfer strategy timeline estimates.
Discussion
Within the Eastern Health catchment area, the time saving to ECR observed with the direct bypass strategy as compared with the secondary transfer strategy was substantially less than previous research estimates across metropolitan Melbourne (15 min vs 52 min).3 Moreover, the majority of patients who were transferred on to the CSC from our PSC for ECR received thrombolysis prior to transfer, which given the study period DTN time of 45 min equates to median therapy administration time of 60 min from scene (Transfer time to BHH of 15 min+DTN time of 45 min). Pending the results of ongoing trials, the use of IV thrombolysis prior to thrombectomy remains the standard of care for eligible ELVO cases. It is associated with higher rates of successful reperfusion before thrombectomy (2.4% vs 7.0%) and overall successful reperfusion (79.4% vs 84.5%).4 To date, primary ECR has not been shown to be superior and its non-inferiority is still up for debate. Further, the precise temporal relationship between bridging thrombolysis and ECR in respect to final patient outcomes is not entirely clear.
Previous studies in the Australian setting have found conflicting conclusions regarding the functional outcomes of patients undergoing the direct bypass strategy as compared with the secondary transfer strategy. A 2018 Victorian observational study showed that there was no difference in regard to 90-day functional outcomes between the two groups, but the study risks selection bias as no time metrics were analysed.5 A more recent 2020 observational study from New South Wales out of Liverpool Hospital, a CSC, revealed 93 min longer stroke onset to groin puncture time, worse 90-day functional outcomes (39.6% vs 61.0% of MRS 0–2) and higher mortality (25.3% vs 6.8%) in the secondary transfer group.6 Results from the 2022 RACECAT randomised control trial based in the Catalonia region of Spain, with 1401 patients randomised, showed that there was no significant difference in the rate of good (MRS 0–2) 90-day outcomes (32.8% in secondary transfer vs 33.4% direct bypass) or mortality (37.3% in secondary transfer vs 35.8% direct bypass) between direct bypass and secondary transfer groups.7
Although 90-day functional outcomes have not been shown to be conclusively different between the two transfer strategies, we acknowledge that the effectiveness of reperfusion therapy is highly time sensitive. Meretoja et al attempted to model the additional benefit of ECR on top of thrombolysis with respect to timing. It found that on average, 4 days of disability free days were gained with every 1 min reduction to ECR reperfusion. This finding was relatively static with modelling of ECR at both 45 min and 90 min post thrombolysis.8 Therefore, at the individual patient level the estimated 15 min delay between the two strategies study could be clinically significant, equating to 2 months of disability free days lost.
Our data suggest only one-third of ACT-FAST positive patients would have benefited from the direct bypass strategy. In a resource limited environment, we do need to consider the economic and human cost of bypassing the PSC for all ACT-FAST positive patients. For example, over triage and burdening of the CSC with ACT-FAST positive cases not eligible for ECR may reduce workflow efficiency which may impact treatment metrics for actual ECR candidates. Additionally, human factors such as increased distance to family support, increased distance to follow-up appointments and the disorientating effect of unfamiliar surroundings should also be considered in a patient’s stroke journey from hyperacute therapy to recovery or palliation. The literature on this important opportunity cost is scant and any significant reorganisation of stroke service must take these factors into account.
The difference in time savings from previous estimates seen in our study can largely be attributed to the relatively fast DIDO times achieved at our PSC compared with other services. Since 2015, there has been a continuous quality improvement programme to reduce delay factors at our centre for both DTN and DIDO times.9 The trend reveals there has been a 55% reduction in the DIDO time from 2015 to 2021 (111 min to 50 min). This has been achieved with a combination of interventions including streamlining the referral process to the CSC by granting the neuro-interventionalist PSC imaging access as well as systematically streamlining the code stroke process by setting up a task force to identify and resolve delay factors involving key partners such as the stroke team, emergency department, CT radiographers and the ambulance crew. Even in the presence of a bypass strategy, it is imperative for PSCs to maintain and improve hyperacute treatment metrics as not all patients with ELVO present with high NIHSS or are ACT-FACT positive.
There is currently one MSU in operation in Melbourne, in the first 365 days of operation between 2017 and 2018, it was reported that the MSU facilitated 42 patients for ECR.1 More recent data are not publicly available. Results from two pivotal randomised controlled trials, B PROUD and BEST-MSU have shown that compared with conventional prehospital stroke care, MSU care led to improved functional outcomes.10 11 We; therefore, expect there to be a growing role of the MSU in prehospital stroke care. However, given the resource intensive nature of MSUs, its operational capacity (currently only Monday to Friday during normal working hours), cost-effectiveness and applicability in non-urban or resource-limited settings is still under investigation.
This study affirms that the ACT-FAST algorithm has good sensitivity, specificity and NPV for ELVO. The PPV of 55.7% is similar to previous validation studies and is higher than other field validated scales such as the Rapid Arterial Occlusion Evaluation Scale at 42% and Los Angles Motor Scale at 36%.2 The algorithm only missed four cases of ELVO stroke during the study period.
A large proportion of the false positive ACT-FAST cases were ICH, the vast majority did not require time sensitive neurosurgical intervention despite significant clinical deficits from mostly small to moderate size bleeds. Apart from 3 cases, the rest were all managed in our PSC stroke unit.
Our data also suggest information required in ‘step 3’ of the algorithm may be challenging to acquire on scene by paramedics. Therefore, the number of false positives is likely higher in practice. It is assumed all paramedics have undergone training to use the algorithm.
The main limitation of our study is the observational retrospective nature with time analysis done using google maps software modelling. In addition, we did not consider extra possible delays out of our scope and ability to measure, for instance, ambulance transport factors such as trolley loading and parking. Another limitation of our study is the use of the latest published but nonetheless non-contemporaneous time assessment data for time metric comparison. Unfortunately, workflow metrices are not routinely measured or collected at stroke centres in Australia. The data used for comparison was collected prior to COVID-19 and thus given the shift in some aspects of workflow post COVID-19 it is possible the time difference between the transfer strategies has changed. Anecdotal experience suggests secondary transfer cases may have an additional time advantage during the pandemic as rapid COVID-19 PCR testing done at the PSC may help expedite the procedural workflow at the CSC. Direct health economic calculations and quantitative analysis of human factors was out of the scope of this study.
Although the findings from this study are specific to our PSC the challenges faced are not unique, the overall reality is that the most clinically beneficial and cost-effective strategy of identifying and triaging potential ELVO stroke patients eligible for hyperacute therapy is still contentious. Certainly, the implementation of a continuous quality improvement programme to improve workflow efficiency at a PSC level can be replicated locally and abroad. We contend that there remains a considerable role high performing PSCs can play in the overall stroke systems of care.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Footnotes
Twitter @frosttan07
Contributors Study planning and guarantors: ST and PMCC; LG; Data collection: KS and TF; Time metric modelling: LG and ET.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.