Article Text

Abstract
Background Reversal of vision metamorphopsia (RVM) is a rarely reported disorder characterised by rotation of vision, 180 degrees in the coronal plane. A systematic review and analysis of all available reports of RVM was undertaken to identify the clinical picture, underlying aetiology and proposed pathophysiology and to define anatomical localisation.
Methods We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and used Scopus, Web of Science, Ovid, Medline, Embase, PubMed and CINAHL databases to search for articles about RVM. The available articles were published from 1974 to 2022. We summarised the evidence, analysed the data and represented anatomical localisation to provide information on the clinical patterns for diagnostics and management.
Results Twenty-eight articles fulfilled the selection criteria, providing 52 cases of reported RVM. Reports focused on the clinical picture and evaluation of neurological signs and symptoms. The most common underlying aetiology was a posterior circulation stroke or interruption of the vestibular system. In the analysis, we demonstrated statistically significant differences between ischaemic and vestibular aetiology in the duration of episodes (p=0.03, Z=2.13) and vomiting (p=0.02, Z=2.28) subgroups. Insults present on brain imaging have been mapped via two-dimensional graphical representations (n=16).
Conclusions This review intends to raise awareness of this unusual phenomenon. Swift recognition of this disorder is paramount and appropriate management should be tailored to the individual aetiology. Brain mapping and analysis of cases may elucidate the anatomical localisation of the central integrator of visuospatial orientation. We suggest that sensory information may be synthesised by a multinucleated visuospatial system to form a visual representation of extrapersonal verticality.
- STROKE
- VISION
- BRAIN MAPPING
- MRI
- NEUROOTOLOGY
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Reversal of vision metamorphopsia (RVM) is a rare phenomenon characterised by rotation of vision 180-degrees in the coronal plane. Information is very limited and current knowledge comes from case reports only.
What this study adds
This analysis provides new insight into aspects of spatial perception. By mapping brain lesions and comparing the characteristics of cases, we have presented useful information for loading for localising neuronal pathways and improving upon the current understanding of the visuo-spatial cortex.
How this study might affect research, practice or policy
This review suggests that a high index of clinical suspicion is paramount, as RVM can often present without associated symptoms or examination findings. Clincians should be particularly wary of patients presenting with RVM greater than four hours in duration or with associated vomiting, as stroke was the most likely aetiology.
Introduction
Reversal of vision metamorphopsia (RVM) is a term coined by River et al in 1998.1 Prior to this it has been referred to by many other names such as ‘room tilt illusion’, ‘upside-down vision’ or ‘inverted vision’, although none of these are as specific. RVM is a rarely reported disorder and is specifically characterised by 180-degree rotation of vision in the coronal plane.1 It is also possible for patients to present with other varying degrees of visual tilt and through different three-dimensional planes, although these are usually referred to as incomplete RVM or room tilt illusion at a specific degree of rotation. An example of incomplete RVM or room tilt illusion would be a 90-degree rotation of vision in the sagittal plane. However, this article has chosen to focus on 180-degree rotation of vision in the coronal plane only, one of the more common rotations of vision, so that more reliable findings can be demonstrated with regard to the clinical picture, underlying aetiology, pathophysiology and anatomical localisation.2 Historically, RVM has arisen from a central nervous system (CNS) insult to the brain, where posterior circulation ischaemia is the most common aetiology.2 Other case reports of this phenomenon describe a wide variety of causes, such as vestibular dysfunction, tumours, trauma, seizures, surgical and multiple sclerosis. Thus, the importance of early recognition is stressed to avoid serious consequences.3 With barely one report per year published globally in the literature, patients presenting with RVM are among the very few. Although it is possible that a higher degree of clinical recognition may have developed from continuing publication, there still remains a distinct paucity in the literature with regard to guidelines, review articles, variation of symptoms, examination findings, underlying aetiology and proposed pathophysiology.4 5 This article will provide a systematic review and meta-analysis of all case reports ever published. It will involve a thorough assessment of the clinical picture, clinical patterns and underlying aetiology and define anatomical localisation in order to elucidate collective understanding of the mechanisms of pathophysiology. To our best knowledge this is the most objective and comprehensive review of the subject material. This analysis provides new insight into aspects of spatial perception that have mostly remained theoretical in nature. By mapping brain lesions and comparing the characteristics of cases, one is able to present useful information for localising neuronal pathways and improving the current understanding of its pathophysiology. The seminal works by River et al,1 Malis and Guyot6 and Sierra-Hidalgo et al2 have provided many postulations regarding the processes behind spatial recognition. This analysis aims to build on these ideas, specifically for RVM.
Methods
A comprehensive literature search was performed from seven databases (Scopus, Web of Science, Ovid, Medline, Embase, PubMed and CINAHL), incorporating the following keywords and terms in various combinations and configurations: ‘inversion’, ‘reversal’, ‘rotation’, ‘180 degrees’, ‘vision’, ‘metamorphopsia’, ‘upside down’, ‘rotated vision’ and ‘room tilt illusion’. All abstracts of the identified articles were scrutinised using the appropriate inclusion and exclusion criteria; the selection of articles is demonstrated in figure 1. Cases were included if the author described complete RVM (a 180-degree visual tilt in the coronal plane). Cases were excluded if their patients experienced incomplete RVM (a visual tilt other than 180 degrees in the coronal plane) or if the authors did not specify the degree of tilt. Google Scholar was used to identify any potentially missed articles and the reference lists of all included papers were reviewed with ‘backward chaining’ employed to gather pertinent papers for consideration. There were no restrictions in articles published in any country or any language in order to reduce publication bias. Therefore, 52 cases were identified from 28 different articles that fulfilled the inclusion and exclusion criteria. The earliest article was published in 1974 and the search was continued up to April 2022. The main characteristics of the included cases are summarised in table 1. A retrospective analysis of historical cases has been presented to help define the mechanisms of pathology and anatomical localisation and provide a comprehensive overview of the pathophysiological perception of verticality. Data were collected on demography, duration of symptoms, common presenting complaints, examination findings, aetiology and a large portion dedicated to imaging and anatomy. A subgroup analysis has been completed to conclude if there were statistically significant differences between the characteristics of ischaemic and vestibular aetiology. Continuous variables have been presented as mean and SD. Comparison of the data has used the Student’s t-test for parametric data and Mann-Whitney U for non-parametric data. Comparison of proportions has been analysed with Z test. All comparisons were two-tailed, a p value of <0.05 was deemed statistically significant and CIs of 95% were used where appropriate.
Characteristics of the included reports1–17 28–38
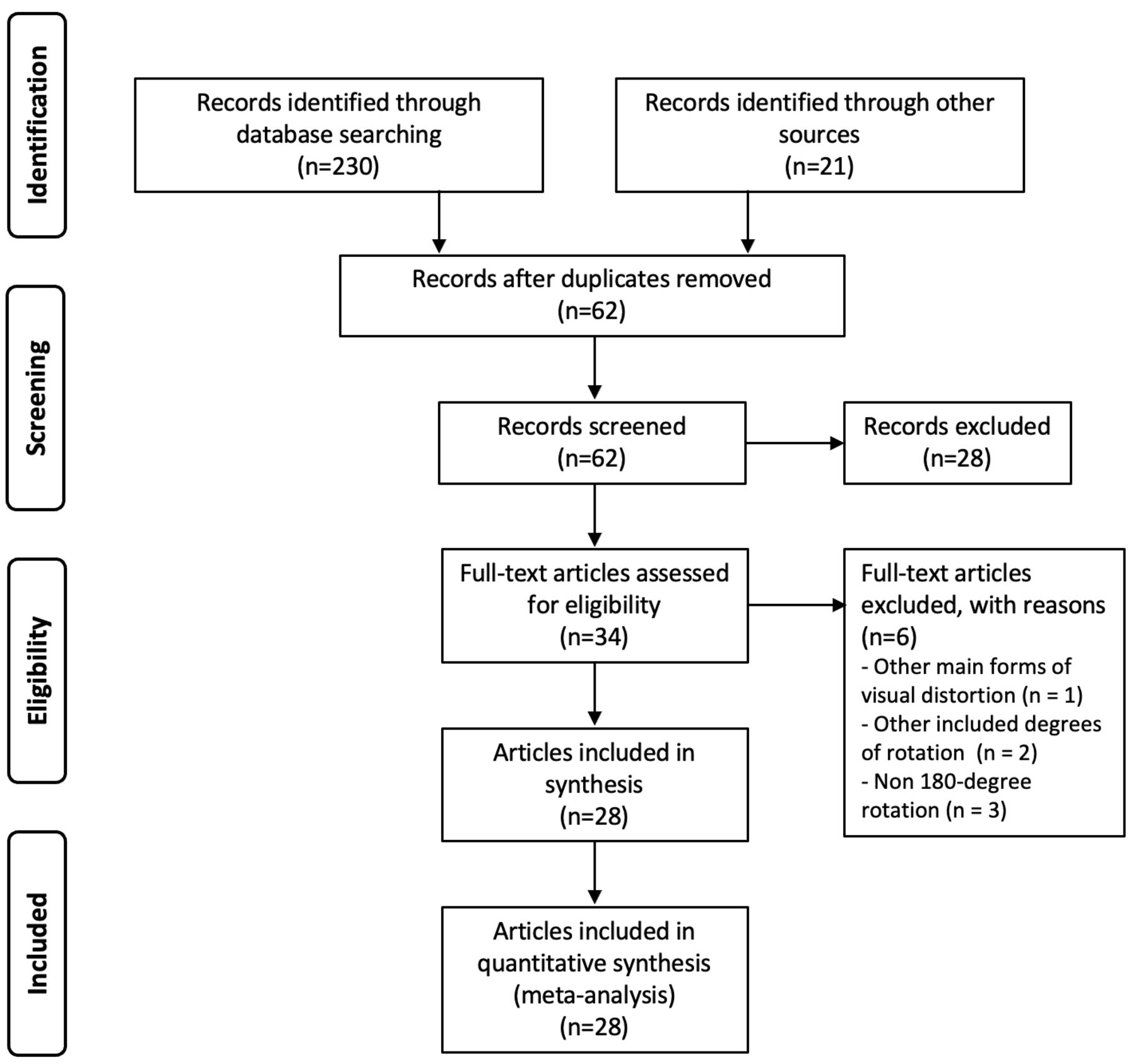
PRISMA flow chart showing the preferred reporting items for this systematic review and meta-analysis. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Results
Clinical picture and epidemiology
As these are rare cases, estimating the incidence and prevalence in this cohort is particularly challenging. The number of cases is few and geographically disparate, and as such there is currently insufficient evidence to provide accurate or reliable estimations. Out of the cases that specified, there was an overall predominance of male patients: 66.0% male and 34.0% female (n=47). The mean age of onset was 52.2±20.2 years (range 12–85 years, n=47). Injury to the CNS was most common to structures in the posterior fossa, peripheral portion of the vestibular pathway or posterior cerebrum. More specifically, common pathology was localised to the cerebellum in 10 cases, brainstem structures in 9 cases, inner ear in 8 cases, posterior region (as described in the reports) in 4 cases, parietal lobes in 3 cases, peripheral portion of the vestibulocochlear nerve in 3 cases, occipital lobe in 2 cases, periventricular in 2 cases, thalamus in 2 cases, caudate nucleus in 1 case, frontal lobe in 1 case, parieto-occipital junction in 1 case, temporo-occipital junction in 1 case, ventricle in 1 case, diffuse in 1 case and unclear in 10 cases. RVM was associated with insults of a single focus in 24 cases (46.2%), multifocal in 12 cases (23.1%), diffuse in 1 case (1.9%) and unclear in 15 cases (28.9%). With regard to the duration of episodes, certain articles have been imprecise in their assessments. In these, authors have defined the duration of episodes with qualitative values such as ‘few hours’ or ‘brief seconds’.6 7 One solution to this problem is to provide an analysis with a dichotomous representation of the mean duration of episodes. With this, one would categorise the duration of episodes into the following groups: ‘seconds’, ‘minutes’ or ‘hours’. In this scenario, ‘minutes’ is recognised as the clear mean and median. However, it may be more useful to infer timing in the small number of cases that have not provided exact numerical values. As such, the term ‘brief seconds’ has been understood as 3 s, ‘seconds’ has been understood as 30 s, in cases 1 and 2 ‘few minutes’ has been understood as 3 min, in case 23 ‘minutes’ has been understood as 10 min, ‘hours’ has been understood as 2 hours, and ‘few hours’ has been understood as 3 hours. In this case, the mean duration of episodes was 135.33 min (n=47, range 3 s–72 hours). However, with significant outliers removed (cases 15, 30, 31, 34, 43, 49 and 52), the mean duration of episodes is 12.09 min (n=40).2 6 8–11 With removal of non-numerical values, the mean duration of episodes is 177.83 min (n=34), and with additional removal of outliers as well as non-numerical values the mean duration of episodes is 16.07 min (n=29).
Presenting symptoms and complaints
Each case demonstrated 180-degree rotation of vision in the coronal plane (n=52). The most common associated symptoms were vertigo (n=21, 40.4%), vomiting (n=13, 25.0%) and nausea (n=12, 23.1%). In addition to the complaints of vertigo, an extra 7.7% (n=4) described a presentation of ‘dizziness’, so in total 48.1% (n=25) presented with some form of complaint of dizziness. Headache was not a very common symptom as it was only present in 15.4% (n=8) of cases, and 11.5% (n=6) did not present with any additional symptoms at all. In two cases, there was a history of a preceding illness, such as a respiratory infection, prior to the acute reversal of vision.11 12
Examination findings
The most common positive examination finding was nystagmus (n=17, 32.7%). Other associated eye signs elicited were diplopia (n=3, 5.8%), abnormal saccade (n=1, 1.9%), apraxia (n=1, 1.9%), hemianopia (n=1, 1.9%), internuclear ophthalmoplegia (n=1, 1.9%), gaze palsy (n=1, 1.9%) and skew (n=1, 1.9%). Ataxia was the next most common associated symptom (n=12, 23.1%), with 7.7% (n=4) of cases presenting specifically as gait ataxia and 7.7% (n=4) as truncal ataxia. Abnormal sensory findings were demonstrated in 13.5% (n=7) of cases, and weakness (n=4, 7.7%), abnormal reflexes (n=3, 5.8%) and hearing deficits (n=2, 3.9%) were not common findings. Of the total cases, 44.2% (n=23) presented with a normal clinical examination at the time of presentation.
Underlying aetiology
Acute infarct was the most common cause of RVM (n=18, 34.6%), with an interruption to the peripheral portion of the vestibular pathway second (n=11, 21.2%). Of these vestibular cases, 54.5% (n=6) were caused by Ménière’s disease, 9.1% (n=1) by cupolithiasis, 9.1% (n=1) by endolymphatic sac tumour, 9.1% (n=1) by herpes zoster infection to the vestibular nerve, 9.1% (n=1) by perilymphatic fistula of the lateral semicircular canal and 9.1% (n=1) by a surgical removal of an acoustic neurinoma. Of the total 52 cases, other aetiologies were transient ischaemic attack (n=4, 7.7%), multiple sclerosis (n=3, 5.8%), migraine (n=2, 3.9%), seizure (n=2, 3.9%), abscess (n=1, 1.9%), concussion (n=1, 1.9%), cortical dysplasia (n=1, 1.9%), haemorrhage (n=1, 1.9%), idiopathic intracranial hypertension (n=1, 1.9%), opioid toxicity (n=1, 1.9%), posterior cortical atrophy (n=1, 1.9%), ventriculostomy (n=1, 1.9%) and unclear in 7.7% (n=4).
Management
Management was individualised as per the underlying aetiology. It was considered on a case-by-case basis, then associated with the guidelines surrounding that subject area. For example, if stroke were the underlying aetiology, patients were investigated with a full stroke work-up and implementation of future stroke prophylaxis was applied as indicated. In all cases, RVM appeared to resolve spontaneously and there was no evidence of any beneficial effect from chemical intervention. The mean duration of episodes for cases managed with anticoagulation or an antiplatelet agent was 948.21 min (n=5), and the mean duration of episodes for patients treated without chemical intervention was 20.6 min (n=5). There was no statistically significant difference between the two groups (p=0.75, Z=−0.32). For non-vascular aetiology RVM, some patients with recurrent rotations of vision were treated with gabapentin. The authors described a complete resolution of symptoms in both cases.13 14 Flunarizine, a selective calcium antagonist, was used to prevent recurrent attacks, with no further attacks identified at 6-month follow-up.15 Carbamazepine and diazepam were both used effectively in the treatment of seizures1 16 and methylprednisolone was used for multiple sclerosis.17 Management was unclear in 29 cases (55.8% of 52 cases).
Subgroup analysis comparing the characteristics of ischaemic (vascular) and vestibular aetiology
There was no statistically significant difference in age when the ischaemia aetiology group was compared with the vestibular aetiology group (55.8±12.9 years vs 56±17.31 years; p=0.61, Z=0.51). There was a statistically significant difference in the duration of episodes of the ischaemia aetiology group compared with the vestibular aetiology group (267.59±916.4 min vs 32.12±63.81 min; p=0.03, Z=2.13). With regard to patient symptoms, there were no statistically significant differences in vertigo between the ischaemia and vestibular subgroups (ischaemia: n=10, 45.5% of 22 cases; vestibular: n=7, 63.6% of 11 cases; p=0.54, Z=−0.62). However, there was a statistically significant difference in patients presenting with vomiting in the ischaemia subgroup when compared with the vestibular subgroup (ischaemia: n=10, 45.5% of 22 cases; vestibular: n=0, 0% of 11 cases; p=0.02, Z=2.28). With regard to examination findings, there were no statistical differences between the ischaemia and vestibular subgroups in patients presenting with nystagmus (ischaemia: n=10, 45.5% of 22 cases; vestibular: n=2, 18.2% of 11 cases; p=0.25, Z=1.15) or presenting without associated examination findings (ischaemia: n=4, 18.2% of 22 cases; vestibular: n=6, 54.5% of 11 cases; p=0.08, Z=−1.74). There were numerically more patients presenting with findings of ataxia in the ischaemia subgroup compared with the vestibular subgroup, although this was not statistically significant (ischaemia: n=8, 36.4% of 22 cases; vestibular n=0, 0% of 11 cases; p=0.06, Z=1.87).
Discussion
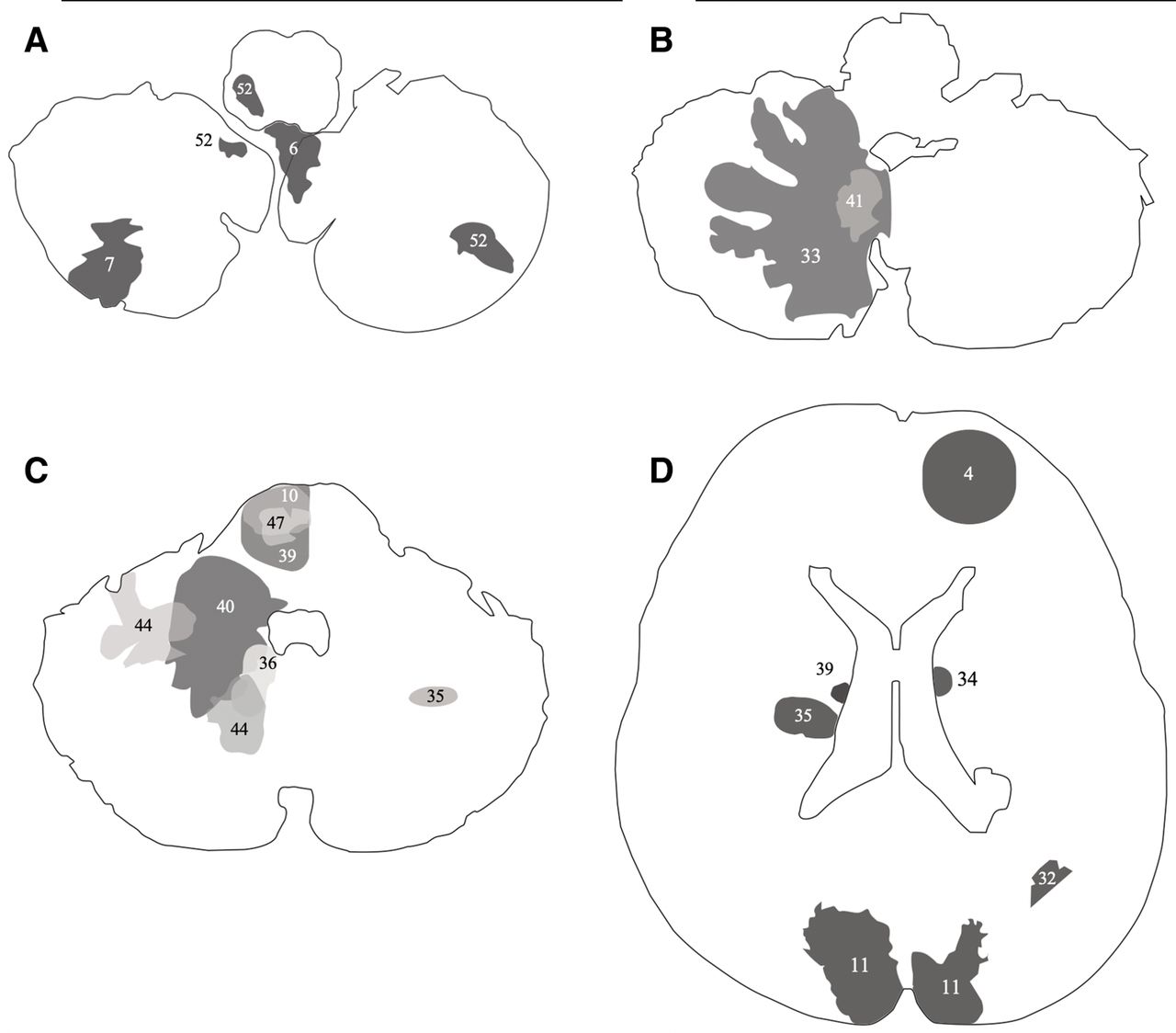
To briefly summarise the results, the meta-analysis has identified that patients with RVM are most likely to be male and presenting with symptoms of dizziness, vertigo, nausea and vomiting. The most common positive examination findings were eye signs and ataxia, but a high proportion did not demonstrate any examination findings. The underlying aetiology varied, but most commonly due to an acute infarct. A high proportion of cases were also due to an interruption of the peripheral portion of the vestibular pathway, which includes the semicircular canals, otolith organs and vestibular component of cranial nerve VIII. We have provided the most up-to-date demographics and epidemiology and have demonstrated significant differences between the subgroups of ischaemia and vestibular system in order to aid in future clinical diagnostics. We have mapped lesions via a two-dimensional graphical representation in order to provide visual insight into the RVM pathways (figure 2).

{kind=link}
{kind=link}
Brain mapping. A graphical representation of the anatomical locations of brain insults based on MRI and CT of cases 4, 6, 7, 10, 11, 32, 33, 34, 35, 36, 39, 40, 41, 44, 47 and 52: (A) cerebellum and medulla, (B) cerebellum and pons, (C) cerebellum, superior cerebellar peduncle and pons, and (D) supratentorial structures including the lateral ventricles.
In normal vision, a two-dimensional image is projected onto the retina via photons. Due to the convexity of the lens, photons of light are refracted in such a way that the image that reaches the retina is inverted.18 The brain interprets the image in conjunction with several complex neurological systems to present the information as upright in its verticality. The current theory of neurological pathways begins with the individual receptive sensory networks. Information is gathered by the visual system, vestibular system, proprioceptive system, graviceptive system and tactile sensation in order to provide an accurate representation of vertical reality.19 In RVM, where the patient’s perception of their own body remains upright and aligned with gravity, it is the external spatial representation that is rotated 180 degrees. A more scientific explanation for this is that, although the egocentric coordinate frame remains upright in its spatial reality, there is a 180-degree rotation of the visual allocentric coordinate frame.20 21 Although much is yet to be understood about RVM, there are certain pathways and processes that are likely to be involved in the perception of extrapersonal space and visual verticality. We propose that the perception of extrapersonal visual verticality is encoded via a network of sensory apparatus and a multifocal, multinucleated visuospatial system. Due to the communication of multiple external sensory receptors and receiving cranial nuclei in the vestibular system, brainstem, cerebellum and cerebral cortex, it is possible that the brain is able to construct multiple spatial reference frames simultaneously from different sensory perspectives.22 It is possible that when the network is interrupted, normal interpretation of verticality becomes confounded by an imbalance of the remaining communicating system, resulting in an active rotation of vision. We can infer that even if there is an interruption to the integrated system in one or more areas (such as in an acute stroke), there are enough remaining functional components to provide adequate information to re-establish spatial reference frames and overcome the representation of rotated vision.
Brainstem and cerebellum
The brainstem and cerebellum were the locations with the highest representation of injury among the cases. There were 9 cases with injury to the part of the brainstem and 10 cases with injury to the cerebellum. Of the brainstem structures, four cases were localised to the medulla and three to the pons. Of the traditional visuospatial structures, the vestibular nuclei are located in the rostral medulla and caudal pons. Some of the other important visuospatial structures, like the medial longitudinal fasciculus, oculomotor nucleus and interstitial nucleus of Cajal, are located in the pons and midbrain, respectively.23 However, these structures are involved in providing optokinetic movement, conjugate movement, vestibular-ocular response and smooth pursuit and are not involved in the direct perception of a visual field.23 It is understood that these areas project fibres to the pulvinar lateral geniculate nucleus of the thalamus before ascending to the cerebral cortex. Although lesions to these areas are known to cause subjective visual vertical tilts, they are not commonly described to cause a complete rotation of vision.23 It is possible that these brainstem structures have functions that are crucial to the brain’s formation of external visual space. Similarly, the cerebellum is not traditionally implicated in the perception of vision. It plays a pivotal role in the coordination of eye movements, but there is currently little evidence to suggest a direct pathway from the retina to the cerebellum for the formation of visual space.24 Out of the cases described, the greatest distribution of injury was over the medial portions of the cerebellum (figure 2). The components most affected were the cerebellar nuclei, peduncles, flocculus and nodulus. We propose that these structures are involved in a visuospatial network that aids in the construction of a retinotopic map. Some research using voxel-based morphometric analysis has demonstrated that these cerebellar structures may be responsible for multiple visual field maps and part of the dorsal attention and visual network.24 The cerebellum receives some afferents directly from the vestibular system, which synapse at the inferior cerebellar peduncle.23 We propose that, although there is no direct connection with visual neurons, it is likely that the cerebellum is part of a large network that may provide reference maps for coherent perception of vision.
Vestibular system
There was a high representation of vestibular pathology among the cases: eight cases demonstrated disease of the inner ear and three cases demonstrated an interruption of the vestibular nerve. At the brain’s peripheries, the utricles and saccules sense linear acceleration, whereas the semicircular canals sense angular acceleration in the roll planes.25 Impulses are carried via afferent pathways which converge at the vestibular nucleus in the brainstem, before reaching a higher order. It is considered that some pathways bypass these nuclei and form direct synapses with the cerebellum.26 From current evidence, it is understood that the information is used for the encoding of postural control and head movement in three-dimensional space.26 In order to provide external visual stability, there is significant interaction between the visual and vestibular systems. One such mechanism is the vestibulo-ocular reflex, which encodes information from the vestibular organs and generates compensatory eye motions.25 In multiple cases described, an interruption of the vestibular system has brought about an alteration of extrapersonal verticality. It is highly likely that vestibular otolith signals may be relevant to the perception of three-dimensional extrapersonal space.26
Visuospatial cortex
Current knowledge of the visuospatial system suggests that neuronal pathways converge in the nuclei of the thalamus, before diverging towards the parietotemporal cortex.27 The integration and synthesis of information from the vestibular and visual systems are evidently important in the formation of extrapersonal space and verticality. It has been suggested that visuovestibular integration is most likely localised at the temporoparietal junction.27 It has also been postulated that plasticity is present in the neuronal cells of the posterior parietal region. It is possible that these cells demonstrate a multimodal nature as they are able to receive sensory information from multiple receptor systems and process this accordingly.1 28 However, our study adds evidence to the ideology that multiple cortical regions are involved in the formation of extrapersonal space and visual verticality. There were two cases with insults directly to the occipital lobes, one case to the temporo-occipital region, one case to the parieto-occipital region, two cases to the parietal lobe and one case to the frontal lobe. Multiple lobe involvement may suggest that the visuospatial cortex may cover more brain than just the parietotemporal region. It is possible that communication between different lobes may provide a network of differing spatial perspectives to construct a coherent representation of upright, extrapersonal space.
Clinical significance
Swift recognition from the history and examination findings is likely to improve time to investigation and guide further appropriate management. However, there is no current evidence that acute management has any beneficial effect on reducing RVM episode duration. We hypothesise that the discrepancy in the mean duration of RVM episodes between the ‘anticoagulation/antiplatelet group’ and the ‘no intervention group’ may be confounded by the extent of individual disease severity. Our results have demonstrated that it is difficult to clinically differentiate between benign and serious causes of RVM and so it is paramount that RVM is identified and appropriately investigated. However, extra attention should be paid to patients describing RVM of a longer duration (more than 4 hours) as we found that this was more likely to be related to an ischaemic aetiology. Additionally, as RVM is likely to resolve spontaneously, it is pertinent that late clinical presentations are not dismissed. For all presentations, clinicians should adopt a high degree of suspicion and a low threshold for head and neck imaging.
Limitations
The author acknowledges the subjectivity of case reports, which is the main source for analysis of this retrospective review. However, it is understood that information on this topic is very limited and clinical trials surrounding this cohort of patients are yet to exist. Furthermore, due to the rarity of the condition, there is only a small sample size for the data analysis and it is to be understood that statistically significant findings act only as a guidance for future research endeavours.
Conclusion
This systematic review and meta-analysis has identified the key patterns and significant differences of all known cases of complete RVM. It highlights the importance of taking a detailed history and performing a thorough neurological examination. A high index of clinical suspicion is paramount as RVM can often present with subtlety or without associated symptoms or examination findings. Visual symptoms are transient and appear to resolve spontaneously irrespective of treatment. The aetiology of cases was diverse, the most common of which was a posterior circulation stroke or interruption to the peripheral portion of the vestibular pathway, most likely resulting in a unifocal region of injury. For the most part, there were no statistical differences in the characteristics between the ischaemia and vestibular subgroups, although notably patients in the ischaemia subgroup were more likely to present with RVM of a longer duration or symptoms of vomiting when compared with those in the vestibular subgroup. As MRI is the most precise modality to demonstrate the integrity of the posterior fossa, we would advise performing timely MRI of the brain and angiography as first line to identify any sinister underlying pathology. Multiple regions of injury have been mapped and presented via two-dimensional graphical representations (figure 2). Future studies involving functional imaging should be encouraged in order to accurately localise these tracts and enhance knowledge of the multisensory network and visuospatial system.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors JAY was the lead and is the sole author of this research.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.