Article Text

Abstract
Background Intra-arterial treatment (IAT) improves outcomes in acute ischaemic stroke. Presence of collaterals increases likelihood of good outcome. We investigated whether variations in the circle of Willis (CoW) and contributing carotid arteries influence outcome in patients who had a stroke treated with IAT.
Methods CT angiography data on patients who had an acute stroke treated with IAT were retrospectively collected. CoW was regarded complete if the contralateral A1 segment, anterior communicating artery and ipsilateral posterior communicating artery were fully developed, and the P1 segment was visible. Carotid artery contribution was studied with a self-developed carotid artery score ranging from 0 to 2 depending on the number of arteries supplying the occluded side of the CoW. Good clinical outcome was defined as modified Rankin Score ≤2 and measured at discharge and 3 months. We calculated risk ratios for the relation between completeness of the CoW, carotid score and good outcome, and performed a trend analysis for good outcome according to the carotid score.
Results 126 patients were included for analysis. Patients with a complete and incomplete CoW had a comparable risk for good outcome at discharge and 3 months. A higher carotid score was associated with a higher likelihood of good clinical outcome (p for trend 0.24 at discharge and 0.05 at 3 months).
Conclusion In patients with acute ischaemic stroke treated with IAT, chances of good clinical outcome tended to improve with number of carotid arteries supplying the cerebral circulation. Completeness of the CoW was not related to clinical outcome.
- STROKE
- CEREBROVASCULAR DISEASE
Data availability statement
Data are available upon reasonable request. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The presence of adequate collaterals aids penumbral tissue preservation in acute ischaemic stroke and hence influences outcome after stroke. Most studies measure collateralisation by visibility of leptomeningeal collaterals in the affected hemisphere as seen on CT angiography.
WHAT THIS STUDY ADDS
In this study, we investigated whether variations in collaterals, by means of the circle of Willis and number of carotid arteries supplying the cerebral circulation, are associated with clinical outcome in patients with acute ischaemic stroke treated with intra-arterial treatment.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study further defines which patient is more likely to benefit from intra-arterial treatment.
Introduction
Stroke is one of the leading causes of death and disability. Several trials showed that intra-arterial treatment (IAT) in acute ischaemic stroke treatment leads to better outcomes.1–6 Angiographic success rate is much higher than clinical recovery rate. One of the factors involved in this discrepancy is the presence of collaterals.7 8 The presence of adequate collaterals hinders penumbral tissue loss in acute ischaemic stroke9 and hence influences outcome after stroke.
The cerebral collateral circulation may be divided into primary collateral circulation through the circle of Willis and secondary collateral circulation through the leptomeningeal and ophthalmic arteries. Previous studies on patients with carotid artery occlusion or severe carotid stenosis suggest that an incomplete circle of Willis increases risk of ischaemic stroke.10–12 In addition, extent of collateralisation influences outcome in patients who had a stroke treated with IAT.3 13–15 However, most of these studies measure collateralisation by visibility of leptomeningeal collaterals in the affected hemisphere as seen on CT angiography (CTA).3 13 14 16 In this study, we investigated whether variations in collaterals, by means of the circle of Willis and number of carotid arteries supplying the cerebral circulation, are associated with clinical outcome in patients with acute ischaemic stroke treated with IAT.
Methods
Patients
All patients with acute anterior ischaemic stroke, due to carotid T-top or middle cerebral artery (MCA) (M1) occlusion, who were treated with IAT in the period of October 2002–October 2013 (start of MR CLEAN trial) in Haaglanden Medical Center, The Hague and Antonius Hospital Nieuwegein, were included in the study. Demographic and clinical data were recorded at baseline including age, sex, time of symptom onset, National Institutes of Health Stroke Scale (NIHSS), blood pressure and serum glucose on admission. For all patients, type of intra-arterial therapy (intra-arterial thrombolysis or mechanical thrombectomy including type of device used) was registered. Patients with atherosclerotic carotid bifurcation occlusions or carotid dissections were not included in the study. The decision to treat a patient with IAT was made for each patient individually and IAT was performed only after obtaining consent from the patient or his relatives. Secondary preventive treatment was initiated according to European guidelines.17
Radiological characteristics
For each treated patient, site of intracranial occlusion or stenosis on CTA, presence of extracranial internal carotid artery occlusion or stenosis, Clot Burden Score (CBS),18 Alberta Stroke Programme Early CT Score (ASPECTS),19 leptomeningeal collateral flow (Collateral Flow Grading, CFG),20 degree of recanalisation after IAT (Thrombolysis In Cerebral Infarction (TICI) score20) and anatomy of the circle of Willis were assessed. The circle of Willis was regarded complete if there was a fully developed and open anterior (A)1 segment contralateral to the acute occlusion, anterior communicating artery (ACoA), ipsilateral posterior communicating artery (PCoA) and visible posterior (P)1 segment.
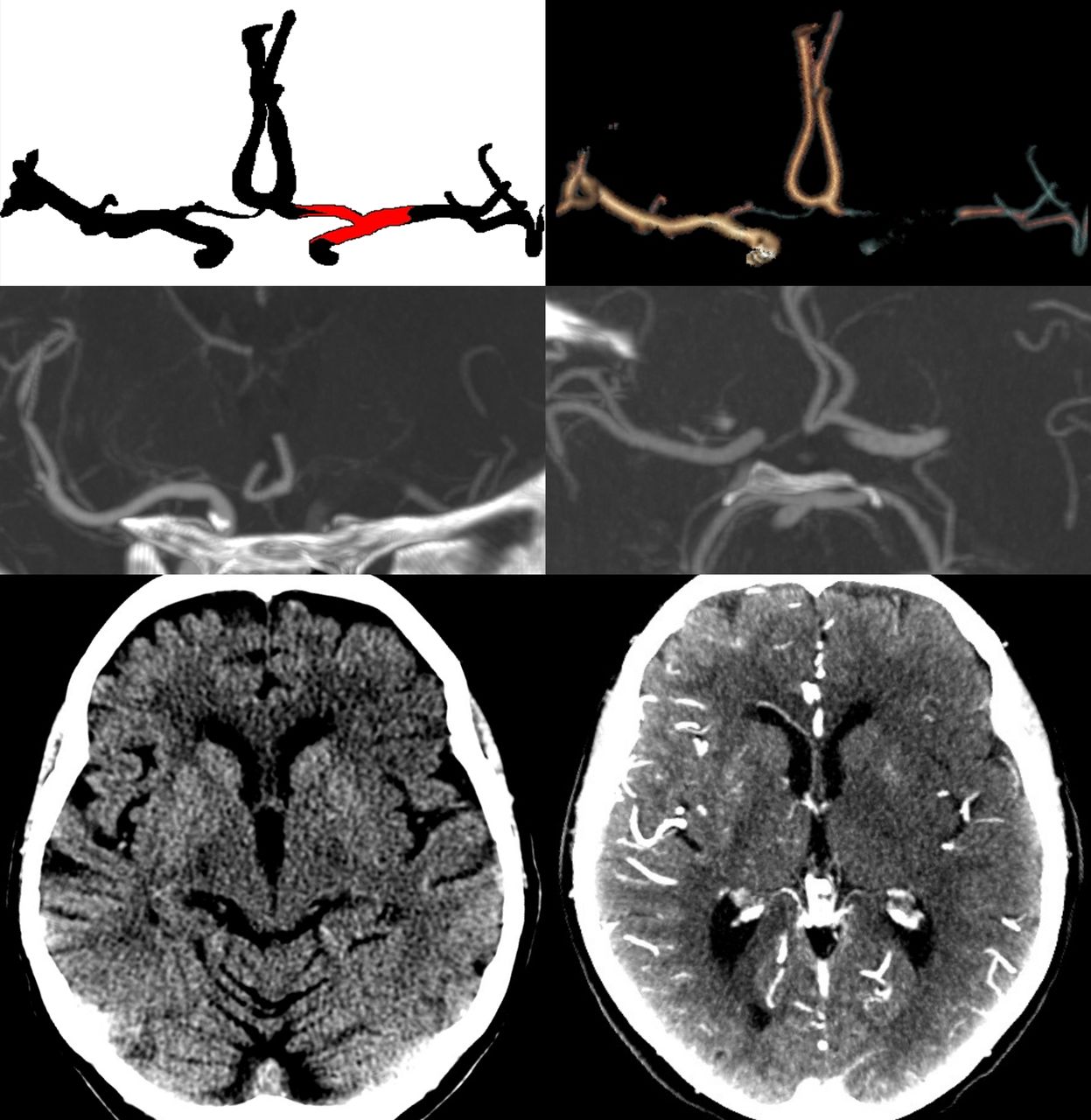
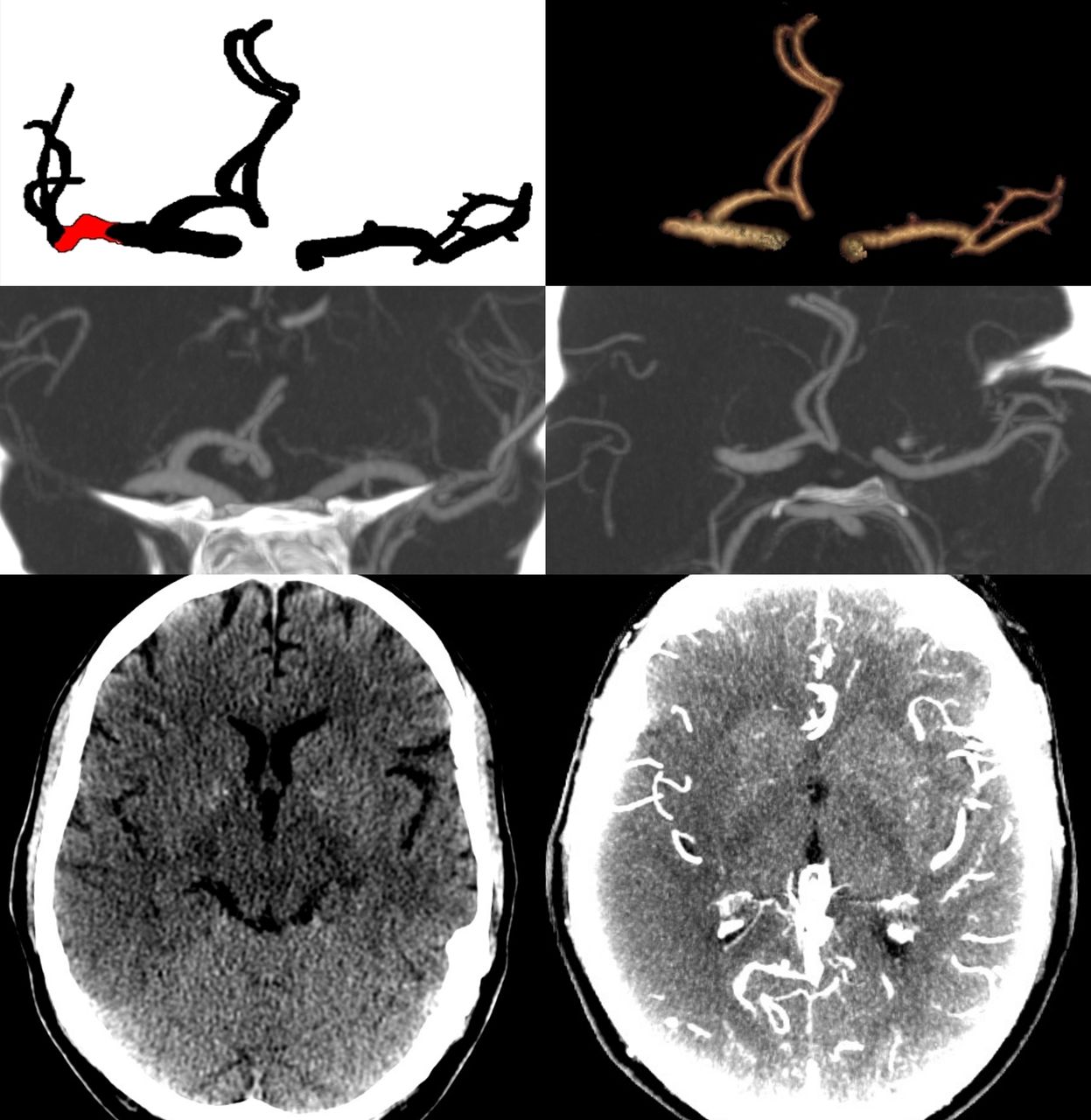
To investigate the contribution of the carotid arteries, we developed a score to determine the effect of circle of Willis variation on cerebral perfusion (figures 1–3):
Carotid score 0: no contribution of either carotid artery to the collateral pathway. An example is a carotid T-top occlusion with a hypoplastic A1 segment contralaterally precluding perfusion of the circle through the contralateral anterior circulation.
Carotid score 1: the circle of Willis is perfused from one carotid artery only. This happens with:
An M1 occlusion with a normal ipsilateral A1 segment and a hypoplastic contralateral A1 segment.
An M1 occlusion with bilateral symmetrical A1 segments but without a visible ACoA precluding perfusion from the contralateral carotid artery.
A carotid T-top occlusion and a dominant contralateral A1 segment, thus feeding both anterior cerebral arteries through the contralateral internal carotid artery (ICA).
Carotid score 2: perfusion from two carotid arteries:
An M1 occlusion with normal bilateral A1 segments and a visible ACoA.
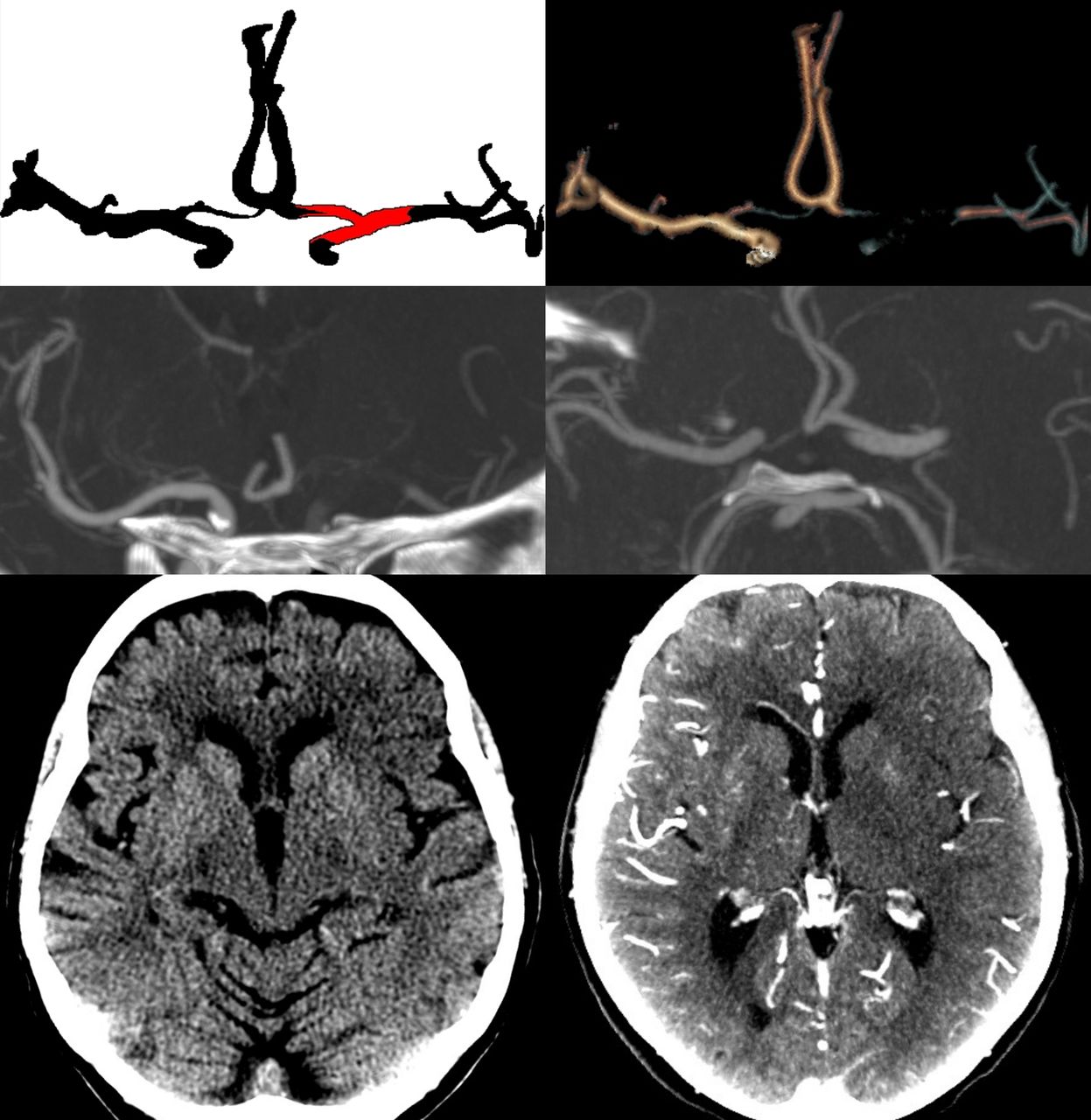
Carotid score 0, no contribution of either carotid artery to the collateral pathway, on non-enhanced CT, CT angiography and maximum intensity projection reconstructions.

Carotid score 1, the circle of Willis is perfused form one carotid artery only, on non-enhanced CT, CT angiography and maximum intensity projection reconstructions.

{kind=link}
{kind=link}
{kind=link}
Carotid score 2, perfusion from two carotid arteries, on non-enhanced CT, CT angiography and maximum intensity projection reconstructions.
Recanalisation was regarded successful if the TICI score at the end of the intra-arterial procedure was 2b or 3. Most patients underwent a CT scan 24 hours after treatment or after any clinical deterioration. All radiological scores were assessed by an experienced neuroradiologist (GLaN) blinded for clinical outcome.
Clinical outcomes
Clinical outcome was retrospectively assessed with the modified Rankin Score (mRS)21 22 at discharge and after 3 months. Good outcome was defined as an mRS score of ≤2. In addition, we recorded complications both during the intra-arterial procedure and during admission.
Statistical analysis
Descriptive statistics were used for baseline, radiological and treatment characteristics. We calculated risk ratios (RRs) and 95% CIs for the relation between the completeness of the circle of Willis (complete vs incomplete), the carotid score and good clinical outcome with Poisson regression.23 Moreover, we performed a trend analysis for good clinical outcome according to the three classes of the carotid score by taking this characteristic as a continuous variable. In addition, we adjusted for the predefined clinical (NIHSS, age and time to IAT) and radiological characteristics (ASPECTS, CFG and CBS). Adjusted RRs were calculated in bivariable analyses.
Results
In the period of October 2002–October 2013, 163 patients were treated with IAT in both centres. We were able to retrieve CTAs in 129 patients. Clinical outcome was missing in one patient and in two other patients, the CTA was of low quality and could therefore not be rated appropriately. Hence, 126 patients were included for analysis. Baseline characteristics were essentially the same for both the complete group of 163 patients treated with IAT and the 126 patients who were subsequently included in our analysis (table 1). Fifty-five per cent (n=69) of all patients were men and median age was 62 years; median NIHSS was 14.
Demographics
Treatment
Overall, 89 patients (71%) were treated with intravenous thrombolysis and 122 patients (97%) were treated with IAT. In four patients (2%), the intra-arterial procedure failed. Most patients treated with IAT had mechanical thrombectomy (table 1).
Radiological parameters
The majority of patients (84%) had an ASPECTS of 7 or more. Successful recanalisation was achieved in 59 patients (49%). The median CFG was 3 (range 0–3) and the median CBS was 3 (range 1–8).
Clinical outcome and completeness of the circle of Willis
Thirty-four patients (27%) had a good clinical outcome at discharge and 53 patients (42%) had good clinical outcome at 3 months (table 2).
Clinical outcome at discharge and at 3 months
Patients with a complete circle of Willis and patients with incomplete circle of Willis had a comparable risk for good clinical outcome at discharge (RR 0.82; 95% CI 0.38 to 1.78) and at 3 months (RR 1.01; 95% CI 0.61 to 1.67; table 2).
Clinical outcome and the carotid score
The majority of patients (n=78, 62%) had cerebral perfusion from both carotid arteries (carotid score 2). Of the patients with a complete circle of Willis (n=26, 21%), 22 patients had carotid score 2. Patients with only one carotid artery (carotid score 1) supplying the intracranial circulation tended to have better outcomes compared with patients with carotid score 0 (RR at discharge 1.29; 95% CI 0.20 to 8.43 and RR 2.00; 95% CI 0.32 to 12.59 at 3 months). Further, patients with a carotid score of 2 tended to have more often a good clinical outcome at discharge (RR 1.85; 95% CI 0.30 to 11.39) and at 3 months (RR 2.92; 95% CI 0.48 to 17.75) compared with those with carotid score 0. In addition, compared with carotid score 1, patients with carotid score 2 also tended to have higher chances of good clinical outcome (RR at discharge 1.44; 95% CI 0.80 to 2.49 and RR at 3 months 1.46; 95% CI 0.90 to 2.37). A higher carotid score was associated with a higher chance of good clinical outcome at 3 months (ptrend=0.05), but not at discharge (ptrend=0.24).
After adjustment for age, NIHSS at presentation, time to start of IAT, ASPECTS, CFG and CBS, the RRs remained essentially the same (online supplemental table).
Supplemental material
Discussion
The number of carotid arteries supplying the cerebral circulation (carotid score) in the setting of IAT for large (M1 or T-top) artery occlusion seems to be an independent predictor of good clinical outcome after 3 months. However, we observed no relation between completeness of the circle of Willis and clinical outcome after IAT.
Incompleteness of the circle of Willis may result in worse cerebral perfusion and hence more damage in case of acute cerebral ischaemia.10–12 Previous studies have shown that completeness of the circle of Willis, particularly the posterior circle of Willis, is a hallmark of deteriorated cerebral perfusion.24 25 In addition, patients with ipsilateral carotid occlusion before IAT in whom ACoA or PCoA or both were absent were shown to have less favourable clinical outcomes at 90 days.26 We could not confirm such a detrimental effect in our patients who had a stroke with an incomplete circle of Willis treated with IAT. A possible explanation for this might be that in our study, only three patients (2%) suffered from an ipsilateral carotid occlusion. We did find a negative influence of impaired carotid contribution by means of our carotid score. Hence, one could hypothesise that the sum of both the carotid occlusion and the incompleteness of the circle of Willis results in less favourable outcome in the aforementioned study. A larger, more recent study combined patients from the DEFUSE2 and CRISP Studies and studied completeness of the circle of Willis in relation to functional outcome after IAT. In line with our results, no association was found between incomplete circle of Willis and functional outcome.27
Contralateral carotid occlusion is well known to increase risk of stroke or death in patients treated with carotid endarterectomy because of symptomatic carotid stenosis.28 In addition, contralateral carotid artery stenosis has been shown to be an independent predictor of poor clinical outcome in patients who had a stroke with acute tandem occlusion treated with IAT.29 These studies are in line with our results, showing that that loss of carotid arteries supplying the cerebral circulation reduces the likelihood of good clinical outcome. Conversely, another study showed that there was no strong effect of a coexisting ICA stenosis in acute MCA stroke on tissue status or perfusion parameters on MRI.30 Moreover, cerebral blood volume was found to be elevated in patients who had a stroke with coexisting ICA stenosis, possibly reflecting improved peripheral collateral circulation. However, patients with carotid occlusions were excluded in this study, only ipsilateral carotid stenosis was studied.
Our study has several limitations. First, our study focused on the collateral circulation by the circle of Willis and carotid arteries. Previous studies have shown that the leptomeningeal collaterals play a key role in chances of successful recovery after IAT.3 13–15 31 32 We, therefore, included a score for leptomeningeal collaterals (CFG)19 and corrected the RR for good clinical outcome for this score (see online supplemental table). After this adjustment, however, the RRs remained essentially the same. Second, we did not measure the flow in the ophthalmic artery. When flow is reversed in the ophthalmic artery, it also functions as collateral for the cerebral circulation. Nevertheless, this reversed flow is merely considered an indicator of diminished cerebral perfusion24 and as such not a rescue pathway for cerebral circulation in case of an acute cerebral arterial occlusion. Third, extracranial carotid disease and basilar artery disease were not included in the study. One could hypothesise that any atherosclerotic disease on these locations also influences the cerebral collateral circulation. In addition, we did not register the presence of fetal-type posterior cerebral artery. The presence of such artery might substitute loss of blood flow in case of an occluded ipsilateral carotid artery and hence influence extent of infarction and functional outcome. However, given the rather low number of patients included in our study, we assume that these effects are limited. Fourth, patients included in our cohort were treated with IAT in the era before IAT was standard of care. We realise that our series is relatively old; however, we think we still retrieve valuable information from it about the pathophysiology of reperfusion and outcome. Although the applied IAT techniques were probably less sophisticated as they are nowadays, we do not expect that this had a substantial impact on our results because our study aimed at finding causal relation between completeness of the circle of Willis and clinical outcome after IAT and hence studied cause of disease.
A possible explanation for the lack of a positive relation between completeness of the circle of Willis and clinical outcome might be that we studied the primary circulation in the acute setting. Previous studies showed that collateralisation may take months to develop and animal models show that restoration of blood flow through collateral vessels after MCA occlusion takes a month.33 34 Most of these studies focused on the role of the collateral circulation by the circle of Willis in patients with atherosclerotic carotid artery disease. We did not select our cohort based on the presence of carotid artery disease. However, we did study the effect of the number of carotid arteries supplying cerebral circulation and found a relation between this carotid score and clinical outcome.
In patients with acute ischaemic stroke treated with IAT, chances of good clinical outcome improve with the number of carotid arteries supplying the cerebral circulation. Completeness of the circle of Willis does not seem to relate to clinical outcome after IAT. Further studies are needed to confirm our findings in a larger cohort.
Data availability statement
Data are available upon reasonable request. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
Formal approval from the local ethics committee was not indicated because this study was based on routinely collected data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conception—AR, GLaN, JB, MW, AA. Design—AR, AA, GLaN. Acquisition and analysis—AR, HH, WS, J-AV. Interpretation of data—AR, JB, MW, GLaN, AA. Draft of the work or substantive revision—AR, JB, J-AV, WS, MW, GLaN, AA. Guarantor - AR.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.