Article Text

Abstract
Objective To assess the knowledge, attitudes and practices of healthcare professionals regarding the diagnosis and management of spontaneous intracranial hypotension (SIH).
Methods We performed a cross-sectional, web-based survey of multiple healthcare professional groups in the UK from June to August 2021. There were 227 respondents to the survey, including 62 general practitioners, 39 emergency medicine physicians, 38 neurologists, 35 radiologists, 20 neurosurgeons, 18 anaesthetists and 15 headache nurse specialists. The majority of the respondents were at the consultant level and all worked in the UK National Health Service.
Results Few general practitioners or emergency medicine physicians had ever been involved in the care of a patient with SIH or received teaching about SIH. Only 3 of 62 (4.8%) general practitioners and 1 of 39 (2.5%) emergency medicine physicians were confident in recognising the symptoms of SIH. Most neurologists were confident in recognising SIH and performed MRI of the brain as a first-line investigation, although there was variability in the urgency of the request, whether contrast was given or MRI of the spine organised at the same time. Most said they never or rarely performed lumbar puncture for diagnosis of SIH. Most neuroradiologists, but few general radiologists, were confident in interpreting imaging of patients with suspected SIH. Lack of access to epidural blood patching, personnel able to perform myelography, and established management pathways were identified by many respondents as barriers to the treatment of SIH.
Conclusions We have identified a lack of awareness of SIH among non-specialists, several barriers to optimal treatment of SIH and a variation in current management pathways. The results highlight the need for education of healthcare professionals about SIH and the development of clinical practice guidelines to enable delivery of optimal and equitable care for patients with SIH.
- headache
- CSF
- neuroradiology
- neurosurgery
- pain
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
It is known that misdiagnosis and diagnostic delay are common in spontaneous intracranial hypotension (SIH) and several misconceptions are purported to exist in healthcare professionals regarding its diagnosis and management.
WHAT THIS STUDY ADDS
This is the first attempt to systematically survey the knowledge, attitudes and practices of healthcare professionals regarding SIH.
The results show that only a small proportion of general practitioners and emergency medicine physicians are aware of SIH, investigation and management pathways are variable, and there are several barriers to optimal treatment.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These findings serve as baseline data to aid the development of clinical practice guidelines for SIH and highlight important research questions.
We also hope that the results of this survey will be helpful in promoting awareness and education about SIH among non-specialist healthcare professionals.
Introduction
Background
Spontaneous intracranial hypotension (SIH) is a disabling but treatable disorder typically caused by a spontaneous spinal cerebrospinal fluid (CSF) leak. SIH can be diagnosed by clinical history and neuroradiological investigations and treated with non-targeted epidural blood patch (EBP), targeted fibrin glue patching or surgery.1
SIH can present in a variety of different healthcare settings, ranging from outpatient presentation with chronic daily headache, to emergency presentation with acute crisis or deterioration secondary to complications such as subdural haematoma or cerebral venous sinus thrombosis. The management of SIH necessitates coordinated multidisciplinary care, which may include a variety of healthcare professionals, including (but not limited to) general practitioners, emergency medicine physicians, nurses, neurologists, radiologists, anaesthetists and neurosurgeons.
A recent survey of patients with SIH in the UK has shown that the diagnosis of SIH is commonly delayed and treatment can be difficult to access.2 SIH is likely to be more common than previously thought. However, with the best estimate of its annual incidence being 4 per 100 000 individuals per year,3 most general neurologists, neurosurgeons, radiologists and anaesthetists will only see a handful of cases in their career and most general practitioners and emergency medicine physicians may never see a case. Several misconceptions in the diagnosis and management of SIH are thought to exist in clinical practice, which are contradicted by recent evidence.4
We hypothesised that healthcare professionals are likely to have low confidence in diagnosing and managing patients with SIH and that management pathways would be variable, driven by low exposure, low teaching rates and lack of transference of recent evidence into clinical practice.
Objective
The objectives of this survey were to assess the knowledge, attitudes and practices of healthcare professionals in the UK regarding the diagnosis and management of SIH.
Methods
Patient and public involvement
Patient members of the CSF Leak Association, a UK-based charity, were involved from the original conception of the study. The questionnaire was designed in conjunction with patients to ensure the questions were relevant to their priorities, experiences and preferences. Two of the authors of the study are patients who have experienced this condition (JS-B and CJ) and were also involved in the analysis and interpretation of the results and writing of the manuscript. The patient organisation plans to help disseminate the results to the patients and the public via their website and social media platforms.
Study design
We performed a cross-sectional, web-based survey of multiple healthcare professional groups regarding their knowledge, attitudes and practices in the diagnosis and management of SIH. The survey questions were developed and the usability of the survey was tested by focus groups comprising members of the Spontaneous Intracranial Hypotension Specialist Interest Group, with representation from patient members of the CSF Leak Association.
The open survey was hosted by the CSF Leak Association from June to August 2021 on the Snap Surveys platform. The survey was advertised by mailing lists and personal communication to colleagues from members of the Spontaneous Intracranial Hypotension Specialist Interest Group, and by the CSF Leak Association via the social media platforms Facebook and Twitter. No monetary or other incentive was offered for completion of the survey. Respondents were able to review and change their answers by navigating through the survey screens before submitting their answers and were able to save their answers to return to complete at a later time. We included a browser cookie that stopped respondents from completing the survey more than once.
The questions included information on respondents’ specialty, level of experience and exposure to SIH, followed by questions on respondents’ knowledge and practices regarding the diagnosis and management of SIH relevant to their specialty area. The survey included branching logic so that respondents were only asked questions relevant to their specialty. Free-text questions asked all respondents who were aware of the syndrome of SIH to comment on any barriers they felt existed in the diagnosis, investigation and treatment of SIH.
Participants
The survey was open to the following specialty groups working in the UK: general practitioners, emergency medicine physicians, neurologists, radiologists, neurosurgeons, anaesthetists and headache nurse specialists.
Statistical analysis
Convenience sampling was used and no formal statistical sample size calculation was performed. Statistical analysis was performed using SPSS V.27. Normality assumptions were based on visual inspection of histograms and Shapiro-Wilk test. Descriptive data were summarised as mean with SD or median with IQR depending on the distribution of data. No statistical between-group comparisons were made.
Consent
The purpose and content of the survey were approved by the Board of Trustees of the CSF Leak Association charity. No personally identifiable data were collected and responses were anonymous from the point of entry. Participants were not recruited in connection with any use of any healthcare service.
Respondents were informed of the approximate time to complete the survey, the purpose of the survey and the methods of data storage. In order to complete the survey, respondents were required to consent to the data collected being used in a publication. Respondents were asked to disclose any conflicts of interest.
Results
Participants
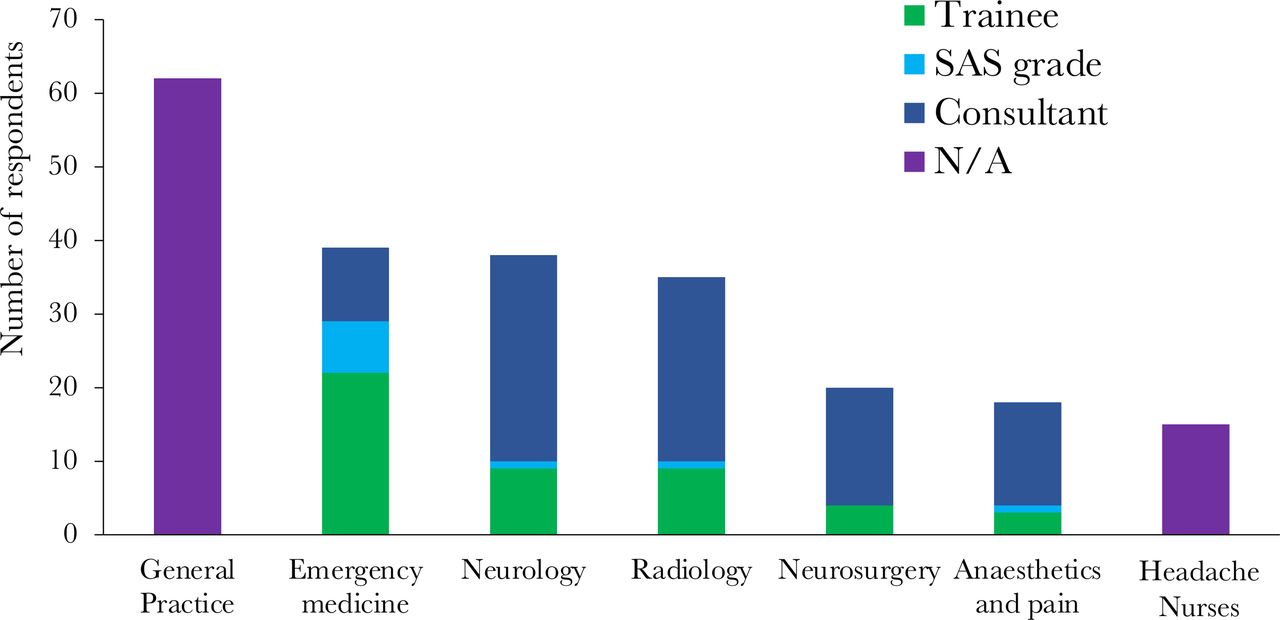
There were 227 respondents to the survey, including 62 general practitioners, 39 emergency medicine physicians, 38 neurologists, 35 radiologists, 20 neurosurgeons, 18 anaesthetists and 15 headache nurse specialists. Of the radiologists, 16 were neuroradiologists and 19 were general radiologists (used to denote any radiologist who was not a neuroradiologist). Most respondents were at the consultant level of seniority, except for emergency medicine physicians (see figure 1). All respondents worked within the National Health Service and 34% also worked in private practice. Of the hospital specialists (neurologists, radiologists, anaesthetists and neurosurgeons), 12.6% worked in district general hospitals and 73.8% worked in neuroscience centres.
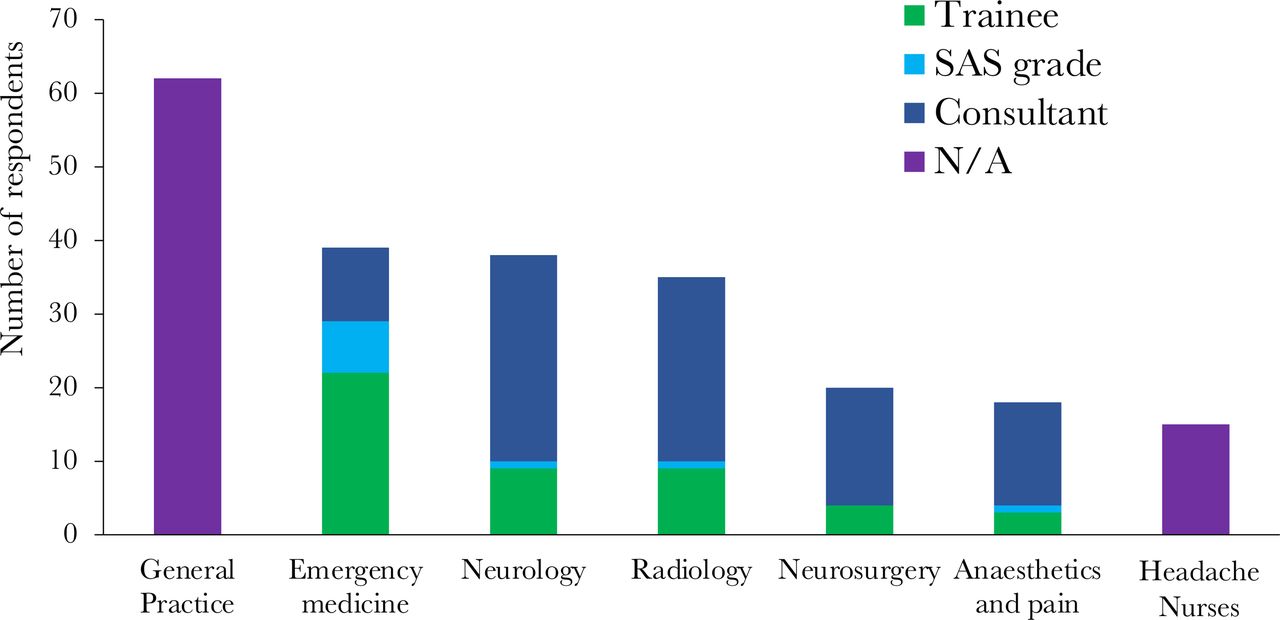
Survey respondents by specialty and grade. ’Radiology’ includes 16 neuroradiologists and 19 general radiologists. SAS grade: staff grade and associate specialist (doctors who are neither trainees nor consultants who have at least 4 years of postgraduate training, two of whom are in the relevant specialty). N/A, not applicable.
Exposure to SIH
Among 62 general practitioners, 23 (37%) said they were aware of the syndrome of SIH and 9 (14.5%) had been involved in the care of a patient with SIH. Among 39 emergency medicine physicians, 9 (23%) were aware of the SIH syndrome, but only 1 (2.5%) had been involved in the care of a patient with SIH.
All neurologists, neuroradiologists and neurosurgeons who responded to the survey were aware of SIH and the majority had been involved in the care of a patient. Approximately half of anaesthetists and headache nurses had been involved in caring for a patient with SIH (figure 2).

Exposure to SIH by specialty group. ‘Radiology’ includes 16 neuroradiologists and 19 general radiologists. The recruitment methods, which included emails to contacts and mailing lists by members of the Spontaneous Intracranial Hypotension Specialist Interest Group and the social media via the CSF Leak Association, likely biased the results towards respondents who were already aware of SIH or involved in its diagnosis and management. SIH, spontaneous intracranial hypotension.
The most commonly cited barrier to diagnosis of SIH (in 38 respondents) was lack of awareness of the condition in medical professionals. Other barriers to diagnosis are listed in table 1.
Responses to the question ‘what barriers (if any) do you feel there are in the diagnosis of SIH?’
Clinical diagnosis
Only 3 of 62 (4.8%) general practitioners and 1 of 39 (2.5%) emergency medicine physicians were confident in recognising the symptoms of SIH.
Most neurologists said they were either confident (60.5%) or very confident (21.1%) in recognising the symptoms of SIH. Most (89%) were able to list at least three symptoms of SIH, and 68% were able to list at least three differential diagnoses of SIH, with the most common answers being migraine, postural tachycardia syndrome, cervicogenic headache and postdural puncture headache. Most (87%) were able to list at least one predisposing condition for SIH, with the most common answers being forms of connective tissue disease.
Of the five headache nurse specialists who saw new patients in the clinic, three were unconfident and two were confident in recognising the symptoms of SIH.
Investigations
All but one (97%) of the neurologists who responded said they would request MRI of the brain as the first-line investigation, 78% said they would request contrast to be given and 54% would request MRI of the spine performed at the same time. Twenty-three (60.5%) would request first-line imaging urgently, with the remainder requested routinely.
Most neurologists said they would never (39%) or rarely (39%) perform lumbar puncture as part of the investigation of SIH. Six (16%) said they perform it sometimes and one (2.6%) about half the time.
Most neurologists said they never (28.9%) or rarely (31.6%) performed an active stand test and autonomic testing or referred to an autonomic clinic in patients with suspected SIH, with only four (10.5%) saying they often or always did this.
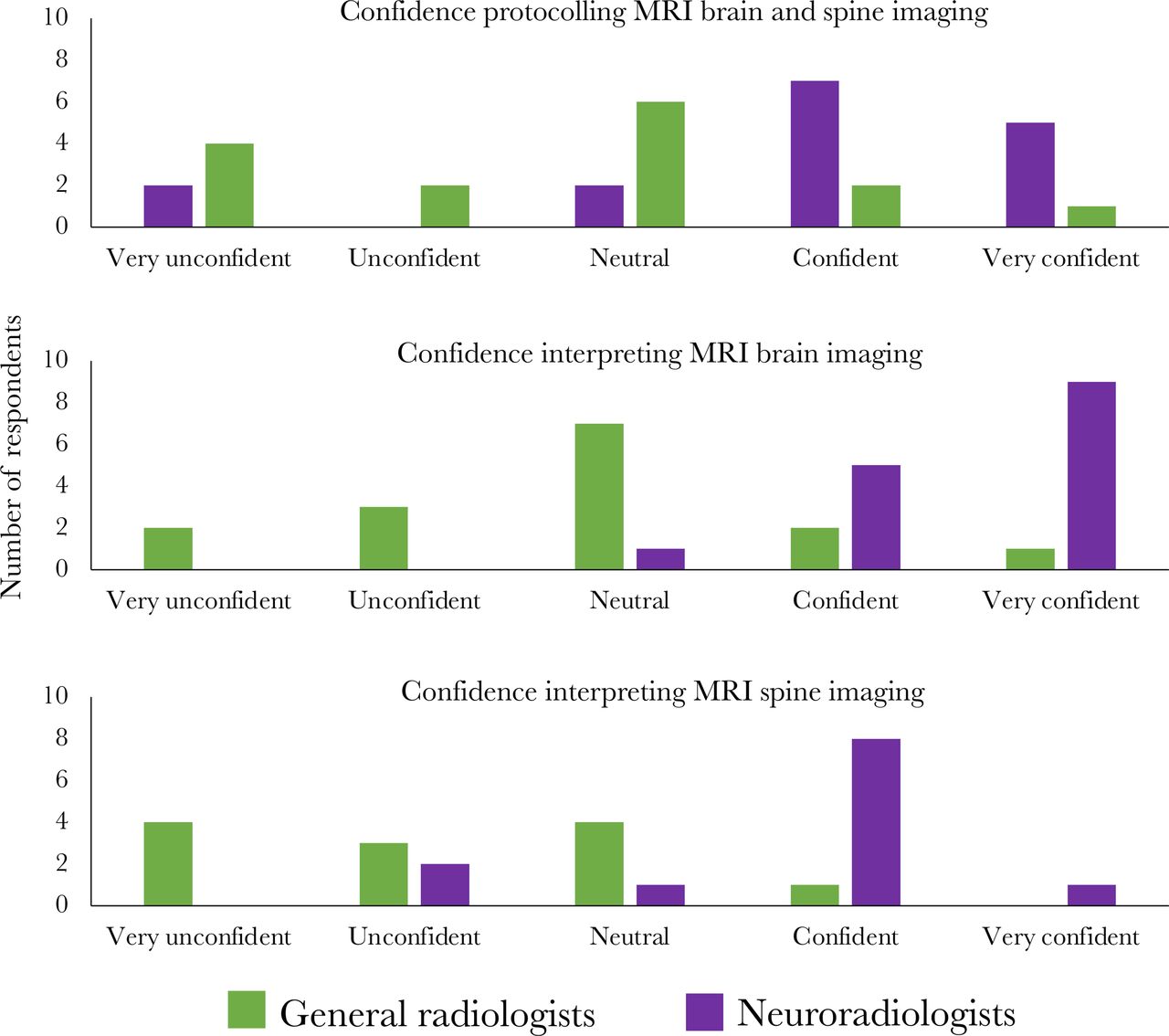
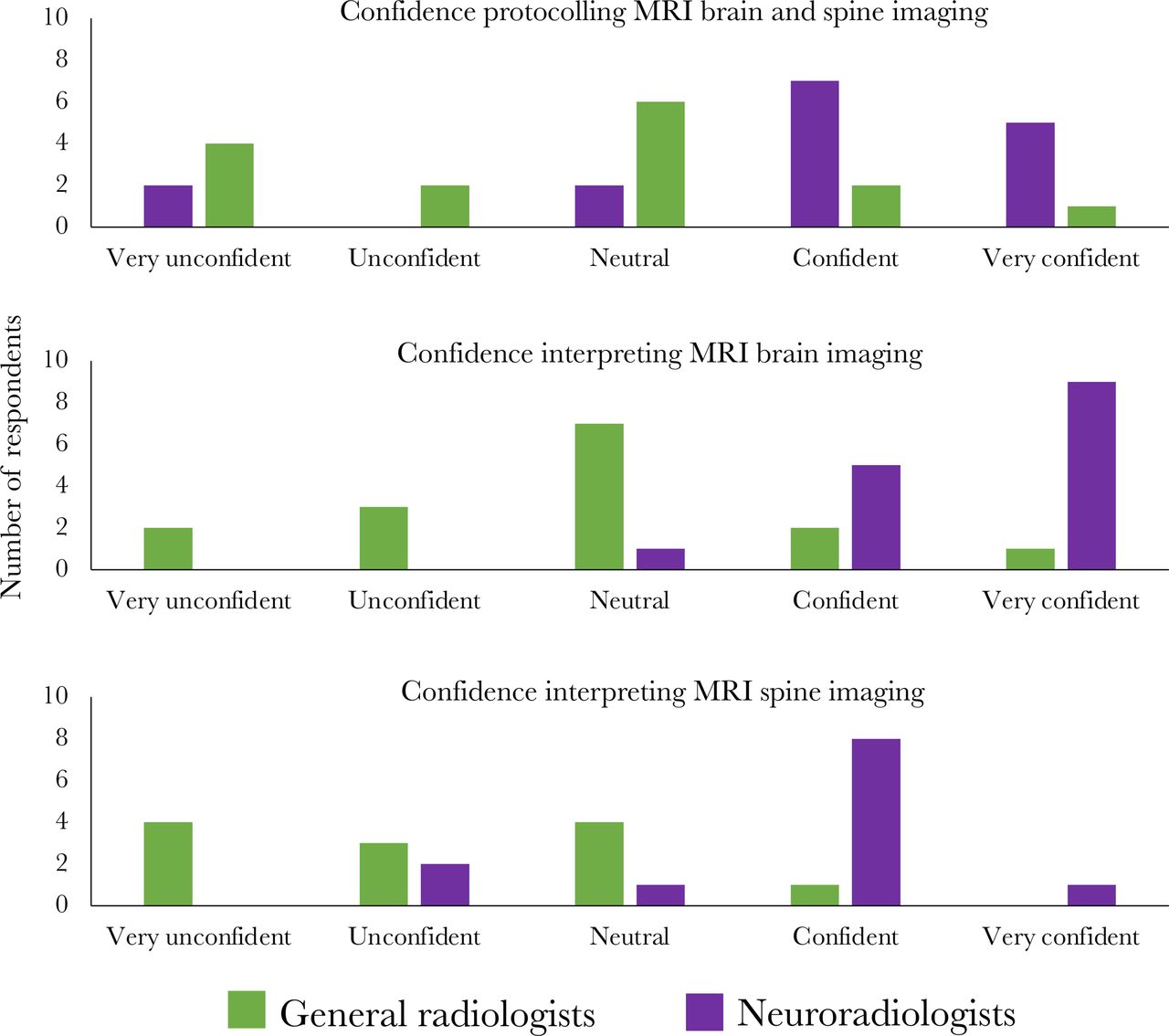
Of the radiologists, most neuroradiologists were confident in protocolling MRI of the brain and spine for SIH, but confidence levels in general radiologists were variable (figure 3). Ten (62.5%) neuroradiologists and four (27%) general radiologists said they routinely give gadolinium contrast with MRI of the brain scans requested for patients with suspected SIH. Half of the neuroradiologists and 27% of general radiologists said they routinely perform high-resolution images of the spine. Fourteen (88%) neuroradiologists and five (33%) general radiologists said they routinely image the whole spine. Neuroradiologists were more commonly asked to report MRI of patients with SIH than general radiologists and were more likely to be confident in interpreting the imaging (figure 3).
{kind=link}
{kind=link}
{kind=link}
Confidence levels of radiologists in protocolling and reporting MRI of the brain and spine of patients with suspected spontaneous intracranial hypotension.
Only four respondents (all neuroradiologists) performed myelography. One performed CT myelography and three performed both CT myelography and digital subtraction myelography. Two performed lateral decubitus imaging routinely. None performed myelography with anaesthetic support. Two used precontrast saline bolus and one used postcontrast saline bolus. Two acquired the first set of images less than a minute after injecting contrast, one between 5 and 10 min, and one >10 min after injecting contrast.
The most commonly reported barriers to investigation of SIH were lack of awareness of the typical imaging findings, delays to MRI being performed, lack of personnel able to perform myelography and lack of a standardised investigation pathway (see table 2).
Responses to the question ‘what barriers (if any) do you feel there are in the investigation of SIH?’
Management
The most commonly recommended conservative management strategies by neurologists were bed rest (97%), hydration (94%), oral caffeine (97%) and avoidance of Valsalva manoeuvres (72%). The results were similar for headache specialist nurses. About two-thirds (23 of 36) had used intravenous caffeine for patients with SIH (5 said they did this often or always), and half (18 of 36) had used greater occipital nerve block injection for patients with SIH (4 said they did this often or always). Access to these therapies was not ascertained and will have influenced the responses. Of the neurologists who said that they recommend a specific duration to trial conservative management before organising EBP, the recommended duration ranged from 1 week to 4 months (median 2 weeks, IQR 1.9 weeks).
There was variation in the ease of organising an EBP: of the 35 neurologists who responded to this question, 11 (31%) reported that it was difficult or very difficult to organise, 13 (37%) that it was easy or very easy to organise, and 11 (31%) were neutral. The most commonly reported barriers to organising EBP were the availability of a person able to perform the procedure, the lack of a dedicated person or pathway for it being performed, difficulty of obtaining emergency theatre slots, and hesitancy from some anaesthetists to perform given the perceived lack of a strong evidence base in SIH.
Of the hospital specialists (neurologists, radiologists, anaesthetists and neurosurgeons), 24 of 100 did not know who usually performed EBPs in their trust. Of the 76 who did know, 50 (66%) said they were usually performed by an anaesthetist and 22 (28.9%) by a neuroradiologist. Thirty-seven (45%) said there was a dedicated person or group of people who performed EBP in their trust.
Only six respondents (three anaesthetists and three neuroradiologists) performed non-targeted EBP themselves. The location they were performed in varied, including interventional radiology suite (three), theatre (two) and anaesthetic room (one). Four performed EBP as a day-case procedure and two performed with an overnight stay in hospital. The target volume of blood aimed to inject varied between 20 mL and 50 mL. All three neuroradiologists regularly used imaging guidance. Two anaesthetists used imaging guidance sometimes and one never. Sedation was only routinely offered by one operator.
Of the 20 neurosurgeons who responded, 9 had an interest in spinal surgery and 11 had performed surgery for SIH. Of the 11 who did not have a spinal surgery interest, 7 said if presented with a patient with SIH they would manage the patient themselves and 4 said they would refer to a colleague. Eleven had used intracranial pressure monitoring in patients with SIH, usually to aid diagnosis in imaging negative patients who had not responded to EBP. Three thought it was helpful rarely, two sometimes, one about 50% of the time, one often and one always. Three did not know how often it had been helpful.
The most commonly reported barriers to the management of SIH were lack of personnel able to perform EBP, lack of a management pathway or guidelines, and perceived difficulty in treating SIH (see table 3).
Responses to the question ‘what barriers (if any) do you feel there are in the treatment of SIH?’
Discussion
This is the first attempt to systematically survey the knowledge, attitudes and practices of healthcare professionals regarding SIH. We successfully surveyed a relatively large number of respondents in a variety of specialties who are involved in the diagnosis and management of SIH. We have shown that only a small proportion of general practitioners and emergency medicine physicians are aware of SIH or have ever seen a patient with SIH, despite more than 95% of patients previously surveyed having first presented to these settings.2 Even in those who are aware of the diagnosis, there is low confidence in recognising its symptoms. Many respondents highlighted this lack of awareness as the main barrier to the diagnosis of SIH. In contrast, almost all neurologists, neuroradiologists and neurosurgeons who responded to the survey have managed patients with SIH. Most neurologists are confident in diagnosing SIH clinically, and most neuroradiologists (but few general radiologists) are confident in diagnosing it neuroradiologically. Despite this, there was variation in the investigations that respondents said they organised, the protocols for MRI and the urgency which the investigations are arranged. Lack of personnel to perform myelography was identified as a barrier to investigation by several respondents. There was consensus on the conservative measures which should be recommended but not on how long these should be pursued before proceeding to EBP, and there was variability in the frequency that symptomatic treatments with intravenous caffeine or greater occipital nerve blocks were performed. Respondents identified several barriers to organising EBP and many commented that the lack of guidelines or a clear management pathway was a barrier to optimal treatment.
The lack of awareness of SIH among non-specialists may help to explain the previously reported misdiagnosis and diagnostic delay in SIH.2 5 This is particularly important as urgency of treatment may lead to increased likelihood of treatment success, as shown by a recent study of surgery for SIH, although it is not known whether this also applies to non-surgical treatment.6 The infrequent use of lumbar puncture as a diagnostic tool is encouraging, given that CSF opening pressure is not a reliable feature of SIH.7 8 The rarity of autonomic testing may reflect a lack of consideration of postural tachycardia syndrome, an important differential diagnosis of SIH, or a lack of access to facilities enabling testing.9 The low confidence of general radiologists in protocolling and interpreting the results of MRI scans suggests a need for either better education or for imaging of all patients with suspected SIH to be protocolled and interpreted by a neuroradiologist. The variability in ease of organising EBP will hopefully be aided by better education and the introduction of standard management guidelines. The perceived difficulty in diagnosing and treating SIH commented on by some respondents as a barrier is in contrast to the rapidly developing investigation techniques and treatments, which means that in most patients who do not respond to first-line treatment the leak site can now be identified and treated.10 This may reflect a lack of application of recent evidence in the clinical environment, but also identifies the need for higher quality evidence in SIH, such as from randomised controlled trials.
There are limitations to this study. The response rate from the total population who were invited to complete the survey via mailing lists is not known. Due to the recruitment pathways via members of the Spontaneous Intracranial Hypotension Specialist Interest Group and the CSF Leak Association, there is likely to have bias towards respondents who are more aware and knowledgeable about SIH than other healthcare professionals. Responses to the survey were anonymous and participants were not asked which hospital or trust they worked in. This was done to encourage comprehensive reporting. However, because of this, we could not identify the number of respondents who worked in the same centre or the number of different centres from which responses were received and therefore whether there was bias towards a particular centre or region of the country. There was a high proportion of respondents who worked in specialist neuroscience centres, rather than district general hospitals, partly explained by the recruitment methods via members of the specialist interest group (who all work in neuroscience centres), but also that in the UK the primary place of work of most neurologists, neuroradiologists and neurosurgeons is in a specialist neuroscience centre.
To the best of our knowledge, no other similar surveys have been performed. Much of the literature on SIH is published in the USA, from specialist centres which have a dedicated service for patients with CSF leaks. The survey exclusively targeted healthcare professionals in the UK, so it is uncertain to what degree our results are generalisable to other countries with different healthcare systems.
A UK regional neuroscience centre has recently published their experience of managing 71 patients with SIH and described their locally developed treatment pathway.11 Almost all patients responded to the staged treatment protocol. This indicates that where multidisciplinary groups of healthcare professionals are interested in SIH and where a treatment pathway is in place, good outcomes can be achieved.
Many respondents highlighted lack of awareness among non-specialists and lack of established management pathways as barriers to diagnosing and treating SIH. These findings serve as baseline data to aid the development of clinical practice guidelines for SIH. We also hope that the results of this survey will be helpful in promoting awareness and education about SIH among non-specialist healthcare professionals.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The purpose and content of the survey were approved by the Board of Trustees of the CSF Leak Association charity. No personally identifiable data were collected and responses were anonymous from the point of entry. Participants were not recruited in connection with any use of any healthcare service. Research ethics committee approval was not required in accordance with the Health Research Authority (HRA) decision tool. In order to complete the survey, respondents were required to consent to the data collected being used in a publication. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors acknowledge other members of the Spontaneous Intracranial Hypotension Specialist Interest Group who contributed to either the development of the survey questions or recruitment of participants, including Heather Angus-Leppan, David Butteriss, Lalani Carlton-Jones, David Choi, Amar Chotai, Brendan Davies, Paul Dorman, Simon Ellis, Danny Morland, Jenny Pople, Daniel Scoffings, Russell Secker, Sarah Mead, Ahmed Toma, Tamsin Trevarthen and James Walkden; Natalie Cookson, who helped in developing the survey questions for the emergency medicine specialists; the Board of Trustees of the CSF Leak Association, who supported the study; and all the respondents to the survey who gave up their time.
Footnotes
Contributors SC: conception and design of survey, analysis of data, interpretation of results, drafting and revising the manuscript. JA, CD, ID, PA, NR, AO, PS, JN, LD'A, SL, VI and EV-H: design of survey, revising the manuscript. JS-B: design of survey, acquisition, analysis of data. CJ: conception and design of survey, interpretation of results, revising the manuscript. MM: conception and design of survey, interpretation of results, revising the manuscript, and is the author responsible for the overall content as the guarantor. All authors approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JA has served on the advisory boards of Allergan/AbbVie, TEVA and Neurorelief; has received payment for educational presentations from Allergan/AbbVie and TEVA; and has received support for educational meetings from Allergan/AbbVie, TEVA, Novartis, Eli Lilly and Merz. LD'A is supported by an NIHR Academic Clinical Fellowship and was the recipient of a research fellowship sponsored by B Braun. SL has received honoraria for attending on advisory board meetings of AbbVie, Eli Lilly, Novartis, Lundbeck, Salvia and TEVA; and has received payment for educational presentations from AbbVie, Eli Lilly, Novartis and TEVA. CJ and JS-B are members of the CSF Leak Association charity and have experienced a CSF leak themselves. MM is chair of the medical advisory board of the CSF Leak Association; has served on advisory boards for Allergan, Autonomic Technologies, Eli Lilly, Novartis, Pfizer, Salvia and TEVA; has received payment for educational presentations from Allergan, electroCore, Eli Lilly, Novartis and TEVA; has received grants from Abbott, Medtronic and electroCore; and has a patent on system and method for diagnosing and treating headaches (WO2018051103A1, issued).
Provenance and peer review Not commissioned; externally peer reviewed.