Article Text

Abstract
Background In patients with multiple sclerosis (MS), relapses and disability progression have been associated with decreased health-related quality of life (HRQoL).
Methods PROTYS, a prospective, multicentre, single-arm, observational study in seven Swiss MS centres, evaluated correlations between change in disability status (measured through the Expanded Disability Status Scale (EDSS)) and HRQoL changes (measured through the global Multiple Sclerosis International Quality of Life (MusiQoL) index questionnaire) in 35 patients with relapsing remitting MS on natalizumab for 1 year. In addition, several other scales were also used, such as: Multiple Sclerosis Intimacy and Sexuality Questionnaire-19, EuroQoL-5 Dimension, and Fatigue Scale of Motor and Cognitive Function. A post hoc analysis further assessed the association between HRQoL changes after 1 year and the MusiQoL subscores and other patient-reported outcome (PRO) measures.
Results At 1 year, patients were categorised into ‘EDSS improved’ (6/35), ‘EDSS stable’ (28/35) and ‘EDSS worsened’ (1/35). Mean disability scores decreased for ‘EDSS improved’ and ‘EDSS stable’ but increased for ‘EDSS worsened’. Mean MusiQoL index score for ‘EDSS improved’ increased from 61.2 at baseline to 66.3 at 1 year, while the ‘EDSS stable’ group increased from 67.9 to 70.8. No meaningful statistical relationship was observed between EDSS group and changes in MusiQoL score. For the post hoc analysis, patients were categorised in ‘MusiQoL improved’ (n=21) and ‘MusiQoL worsened’ (n=14) groups. MusiQoL subscores for ‘symptoms,’ ‘psychological well-being’ and ‘activities of daily living’, as well as scores for several related PRO measures, correlated with improvement of the MusiQoL global index. There was no correlation between the changes in MusiQoL global index and EDSS score.
Conclusions Natalizumab treatment for 1 year resulted in either improved or stable EDSS status in most patients, and although no significant relationship was observed between global HRQoL change and EDSS change, several domains of HRQoL seemed to improve with natalizumab treatment.
Trial registration number NCT02386566.
- MULTIPLE SCLEROSIS
- QUALITY OF LIFE
- COGNITION
- MOTOR CONTROL
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Multiple sclerosis (MS) is associated with impaired health-related quality of life (HRQoL). Though existing studies note improvement in HRQoL with natalizumab treatment, the current evidence on how disease progression is correlated with HRQoL—in particular with specific HRQoL domains—is limited.
WHAT THIS STUDY ADDS
Our results suggest that natalizumab treatment of patients with MS appears to improve several domains of HRQoL: fatigue, symptoms, overall health state, sexual dysfunction and work productivity, regardless of whether disease progression (as measured by Expanded Disability Status Scale scores) was stable or improved.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our results highlight important factors of the HRQoL of patients with MS, and specifically underline the need to further evaluate how the different domains of HRQoL are affected.
1. Introduction
In patients with multiple sclerosis (MS), frequent relapses and disability progression have been associated with decreased health-related quality of life (HRQoL).1–5 Balance problems, spasticity and depression have been shown to have the most detrimental effect on HRQoL in relapsing–remitting MS (RRMS),6 while fatigue and impaired gait are reported by many patients as the most disabling symptoms.7 8
The potential impact of disease-modifying therapies (DMTs) on HRQoL is actively being investigated.9 Evidence on the potential impact of treatment with the DMT natalizumab on HRQoL is limited, though the existing studies note improvement in HRQoL with natalizumab.3 9–17 Natalizumab treatment has been shown to stabilise or improve disability over time, when measured with the Expanded Disability Status Scale (EDSS),18–22 and improve fatigue,23 24 visual function.25 In addition, natalizumab treatment has shown improvements in physical and psychological measures of HRQoL.3 10
Associations between EDSS changes and HRQoL changes in patients treated with natalizumab have, until now, not been investigated. Thus, the aim of the PROTYS study was to evaluate the relationships between EDSS change and changes in HRQoL, as measured by the global Multiple Sclerosis International Quality of Life questionnaire (MusiQoL) index in patients with RRMS treated with natalizumab for 1 year. A post hoc analysis assessed the association between improvement or worsening in HRQoL after 1 year of natalizumab treatment and the scores of patient-reported outcome (PRO) measures assessing a variety of domains.
This work presents the primary result of the PROTYS study combined with the post hoc analyses.
2. Methods
2.1 Study Design
The PROTYS study (NCT02386566) was a phase IV, prospective, multicentre, observational study to assess the correlation of EDSS with quality of life in patients with MS newly treated with natalizumab. Patients were enrolled over a 2-year period from October 2014 to October 2016 at seven sites in Switzerland.
The primary objective of the PROTYS study was to investigate the associations between categories of change in disability (EDSS) with HRQoL (MusiQoL) at 3 month intervals up to 1 year in a real-life setting of patients with RRMS who started treatment with natalizumab.
Due to low patient numbers, the recruitment goal of the PROTYS study was not met. In December 2016, due to futility in the interim analysis, the decision was taken to stop recruitment and to analyse the population of patients already enrolled. Because of this we were unable to evaluate association between categories of EDSS change and HRQoL, which was the primary outcome of the study. Nevertheless, a subsequent post hoc analysis on the complete PROTYS per-protocol population aimed to identify which factors influence HRQoL based on the MusiQoL index in patients after 1 year of treatment with natalizumab. The secondary objectives of the PROTYS study are reported in online supplemental information.
Supplemental material
The primary objectives of the post hoc analysis were the correlation between the change from baseline to end of study (EOS) in the scores described in detail in Section 2.4, in the annual relapse rate (ARR), the ARR of relapses requiring steroid treatment, and the change after 1 year of natalizumab treatment in the global MusiQoL questionnaire index (categorised as improved or worsened after 1 year).
2.2 Population
Inclusion and exclusion criteria are presented in online supplemental table 1. This observational study included patients who were starting treatment in compliance with the official guidelines of Swissmedic (the Swiss authority for authorisation and supervision of therapeutic products). The decision to prescribe natalizumab was made prior to and independently of the study.
The per-protocol population was defined as patients who completed a full year of natalizumab treatment, received at least eight natalizumab infusions within the year, and had both EDSS and MusiQoL scores available at baseline and at 1 year. The post hoc analysis was also performed on the per-protocol population.
2.3 Treatment
Patients meeting the inclusion criteria were treated with natalizumab 300 mg (Tysabri, Biogen, Cambridge, Massachusetts, USA) intravenous infusion, administered every 4 weeks as specified in the Swiss product label.
2.4 Measures and assessments
Neurological disability was assessed through EDSS assessment at 3 month intervals.26 All EDSS raters were trained and certified. Based on EDSS scores at baseline and at 1 year, the patients were divided into three groups: ‘EDSS improved’ (≥1.0-point decrease sustained for at least 12 weeks), ‘EDSS stable’ (changes sustained for <12 weeks or with changes <1.0) and ‘EDSS worsened’ (≥1.0-point increase sustained for at least 12 weeks).
The overall QoL was measured through self-administered MusiQoL questionnaire at baseline and at year 1.27
At each study visit, the self-administered tests and questionnaires were used except for the Multiple Sclerosis Intimacy and Sexuality Questionnaire-19 (MSISQ-19), which was administered only at study visits 3 and 5. Further information on the self-administered tests and questionnaires can be found in online supplemental information. The study assessments are described in online supplemental table 2.
Participants entered responses to all questionnaires either on paper or directly into an electronic case report form (eCRF) using tablet computers, with the exception of the symbol DMT scores (paper version), which were calculated and entered into the eCRF by study staff.
Relapses were recorded and ARRs calculated. Relapse was defined as the appearance of a new neurological abnormality or worsening of previously stable or improving pre-existing neurological abnormality, separated by at least 30 days from onset of a preceding clinical demyelinating event, present for at least 24 hours and not accompanied by fever or infection.
2.5 Safety
All patients received standard care throughout the observation period. All serious adverse events (SAEs) were recorded. Tests for anti-John Cunningham virus (JCV) antibodies and brain MRI scans were performed according to the standard of care and collected if performed.
2.6 Statistical analyses
2.6.1 PROTYS study
A power calculation was performed prior to the PROTYS study, specifically a one-way analysis of variance with α=0.05, 80% power, two sided and common SD=22. This resulted in the estimated recruitment total of 88 patients being sufficient to answer the research question. An attrition rate of 20% would result in 72 patients in the per-protocol population (24 for each EDSS category, equally distributed). All analyses were performed on the per-protocol population. For the primary outcome, an increase of 10 points in MusiQoL score for the EDSS improved group and a decrease of 10 points in MusiQoL score for the EDSS worsened group were estimated to be required for statistical power. Descriptive statistics (n, mean, median, minimum, maximum and SD) were performed for continuous variables, and frequency distributions (n, %) were used to describe discrete variables. Missing data were substituted by carrying forward the last valid post-baseline observation (last observation carried forward). To test for significant differences between the means at different time points, the Wilcoxon signed-rank test or the Student’s t-test were used as specified. P values less than 0.05 were deemed significant.
2.6.2 Post hoc analysis
Changes in PROs over the course of treatment were investigated for the total population using the Wilcoxon Mann-Whitney test. Statistical endpoints of the assessment of the correlation between the various PRO endpoints are described in online supplemental table 3. Spearman’s correlation coefficients were used to investigate relationships between the change over 1 year in the MusiQoL global index, MusiQoL sub scores and other PROs. Analyses were run separately in the overall study population (N=35) and in the subgroup of patients with improvement in MusiQoL global index (n=21) and with worsened MusiQoL global index (n=14). For the post hoc analysis, the MusiQoL categories of ‘improved’ and ‘worsened’ at 1 year versus baseline were defined as: ‘improved’ equals change in the global MusiQoL index >0, and ‘worsened’ equals change in the global MusiQoL index<0. The post hoc analysis statistical endpoints are described in online supplemental information. All statistical analyses of the study data were performed according to the predefined statistical analysis plan by ACG+using SAS V.9.4 or a newer version.
2. Results
3.1 Patient characteristics
In the PROTYS study, 48 patients with RRMS were screened for inclusion into the study (online supplemental figure 1). The baseline characteristics of the per-protocol population are shown in table 1. In the post hoc analysis, the per-protocol population of 35 patients was included. The per-protocol population was subdivided into two subgroups, one with MusiQoL global index improved (n=21) and one with MusiQoL global index worsened (n=14).
Patient characteristics (N=35; per-protocol population)
3.2 Disability status
In the PROTYS study, after 1 year of natalizumab treatment, 6/35 patients (17.1%) were assessed as ‘EDSS improved’, 28/35 patients (80.0%) as ‘EDSS stable’ and 1/35 (2.9%) as ‘EDSS worsened’. In the ‘EDSS improved’ group: median disability score was 4.00 (Q1, Q3: 2.00, 5.00; range: 2.00–3.50) at baseline and 2.00 (Q1, Q3: 1.00, 3.00; range: 1.00–3.50) at EOS (median change=−1.50; Q1, Q3: −2.50 to –1.00; range: −2.50 to –1.00) (figure 1). In the ‘EDSS stable’ group: median disability score was 3.00 (Q1, Q3: 2.00, 3.5; range: 1.00–5.50) at baseline and 2.50 (Q1, Q3: 2.00, 3.50; range: 1.50–5.50) at EOS (median change=0; Q1, Q3: −0.50, 0.00; range: −1.00 to 0.50) (figure 1). The patient assessed as ‘EDSS worsened’ had an EDSS score of 2.0 at baseline and 3.0 at EOS, sustained for at least 12 weeks. As only one patient showed worsening the subsequent analyses of the primary results were performed comparing the ‘EDSS improved’ and ‘EDSS stable’ groups. Results on the mean change from baseline in number of relapses are available in online supplemental information.

Median EDSS scores at baseline and at 1 year (EOS). N=6 patients (17.1%) were assessed as ‘EDSS improved’ (≥1.0 increase sustained for at least 12 weeks), and n=28 patients were assessed as ‘EDSS stable’ (changes sustained for <12 weeks or changes of <1.0). The single patient with progressed EDSS from 2.0 at baseline and 3.0 at EOS is not separately shown in the graph. EDSS, Expanded Disability Status Scale; EOS, end of study.
3.3 PROTYS study MusiQoL index score (global HRQoL)
In the ‘EDSS improved’ group, the MusiQoL index score, representing global HRQoL, increased from a mean of 61.2 at baseline to 66.3 at 1 year (mean change=5.1 ± 6.4). In the ‘EDSS stable’ group, the MusiQoL index score increased from 67.9 at baseline to 70.8 at 1 year (mean change=2.9 ± 12.1) (table 1). There were no statistically significant differences between the groups.
Analyses of MusiQoL subscores showed that there were no significant differences between the EDSS groups in changes from baseline to 1 year. For the MusiQoL subparameter ‘symptoms’, the score increased in the ‘EDSS improved group’ from a mean of 56.3 at baseline to 71.9 at 1 year (mean change=15.6 ± 11.7), and in the ‘EDSS stable’ group from 64.3 at baseline to 69.4 at 1 year (mean change=5.1 ± 15.9; p=0.118) (table 2). There was no statistically significant difference between the EDSS groups in mean change from baseline to 1 year.
Global HRQoL in patients with RRMS at baseline and 1 year after starting treatment with natalizumab as measured through the MusiQoL questionnaire
3.4 Post hoc analysis
The post hoc analysis was performed on the ‘MusiQoL improved’ (n=21) and ‘MusiQoL worsened’ (n=14) groups. Baseline characteristics and baseline values for scores are in table 2. No correlation was detected in the ‘improved’ and ‘worsened’ MusiQoL groups between the changes from baseline in the MusiQoL global index at 1 year and sex or educational level. No significant differences in sex or educational level between the ‘improved’ and ‘worsened’ groups were found (Fisher’s exact test). The baseline characteristics of patients with an improved MusiQoL index and worsened MusiQoL index appear to be different between the groups (table 3). Baseline, EOS and change from baseline to EOS for MusiQoL index shown in table 4.
Baseline values for scores
Baseline (BL), EOS and change from Baseline to EOS for MusiQoL index: total, improved and worsened groups
There was no correlation between baseline MusiQoL and change in MusiQoL global index from baseline to 1 year (figure 2). A summary of the negative or no correlations of the post hoc analysis results are detailed in online supplemental information.

Scatter plot of MusiQoL global index at baseline versus change in MusiQoL global index, by MusiQoL change categories. MusiQoL, Multiple Sclerosis International Quality of Life.
In the ‘improved’ patients, three specific dimensions of MusiQoL, the ‘symptoms’ score (r=0.5294, p=0.0136), the ‘psychological well-being’ score (r=0.6383, p=0.0018) and the ‘activities of daily living’ score (r=0.5098, p=0.0182), showed a strong positive correlation with the improvement of the MusiQoL global index. This result shows significant direct association between the change of MusiQoL global index and the change in the above dimensions. The differences between MusiQoL groups for ‘improved’ versus ‘worsened’ patients were significant for all domains, except for the domains ‘relationships with family’ and ‘coping’ (figure 3).

The change from baseline to EOS for MusiQoL Index improved (n=21) and worsened (n=14), Wilcoxon Mann-Whitney test, *p<0.05, **p<0.01, ***p<0.001. EOS, end of study; MusiQoL, Multiple Sclerosis International Quality of Life.
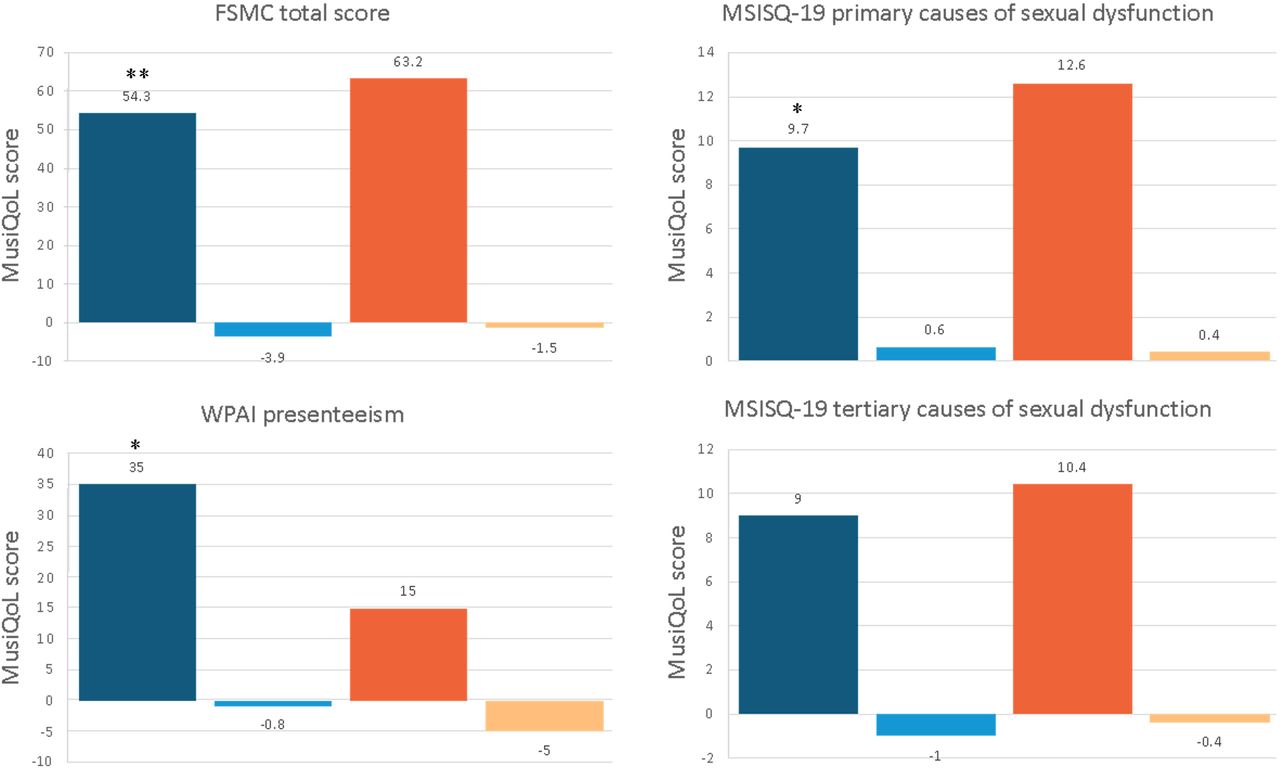
In both the ‘improved’ and the ‘worsened’ groups, no correlation was found between the change from baseline in MusiQoL global index and the change in the EDSS score. There were no significant differences in the EDSS score change between the ‘worsened’ or ‘improved’ patients (Wilcoxon Mann-Whitney test). In the total natalizumab population, improvements in the Work Productivity and Activity Impairment (WPAI) presenteeism score (r=−0.5439, p=0.0294) and the MusiQoL sub scores, psychological well-being (r=0.4609, p=0.0053), symptoms (r=0.4279, p=0.0103), and sentimental and sexual life (r=0.4361, p=0.0088) were correlated with the improvement of the MusiQoL global index. This was consistent with the findings in the MusiQoL-improved patients showing that improvement in MusiQoL global index correlated with the score of the MSISQ-19 for primary causes of sexual dysfunction (r=−0.5157, p=0.0167), the FSMC total score (r=−0.6300, p=0.0022), and in the presenteeism WPAI score (r=−0.5862, p=0.0452) (figure 4, online supplemental table 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between change in global MusiQoL index after 1 year of natalizumab and the change from baseline to end of study (EOS) in the neurological symptoms and the PROs. Non-parametric Spearman’s correlation coefficient. *p<0.05, **p<0.01. FSMC, Fatigue Scale of Motor and Cognitive Function; MSSIQ-19, Multiple Sclerosis Intimacy and Sexuality Questionnaire-19; MusiQoL, Multiple Sclerosis International Quality of Life; PROs, patient-reported outcomes; WPAI, Work Productivity and Activity Impairment.
In addition, a negative association between the increase in the ‘tertiary causes of sexual dysfunction’ score and the improvement of the MusiQoL global index (‘psychosocial causes’ score, r=−0.4113, p=0.0640) was found. Finally, a negative association between the change from baseline to 1 year in the MusiQoL global index and the change in the Beck Depression Inventory-FS score in the ‘improved’ group was found (r=−0.4930, p=0.0619).
3.5 Safety/complications
No treatment-related SAEs were reported. Four patients experienced one or more SAEs, including acute hospitalisation with psychosis (n=1), mastitis and urinary tract infection (n=1), pregnancy (n=1) and severe MS relapses (n=2). In one patient a relapse occurred approximately 6 weeks, in another patient 6 months after initiating natalizumab treatment while still on therapy.
Discussion
The primary PROTYS study looked at patients with RRMS treated with natalizumab for 1 year and aimed to assess correlations between changes in disability status and HRQoL; the post hoc analysis looked further at factors that may influence QoL in patients with MS treated with natalizumab.
While there was no statistically significant difference in global HRQoL change (MusiQoL index score) between ‘EDSS improved’ and ‘EDSS stable’ groups of patients, natalizumab treatment did appear to improve several domains of HRQoL: fatigue, symptoms, overall health state, sexual dysfunction and work productivity, regardless of whether EDSS scores were stable or improved. Additional results and discussion regarding fatigue and work productivity are characterised in online supplemental information.
With respect to changes in EDSS within 1 year of natalizumab treatment, the majority (80.0%) of patients had stable EDSS scores, with all other patients (except for one with EDSS progression) showing sustained EDSS improvement. Long-term data from the 10 year real-world Tysabri Observational Programme (TOP) study revealed a 10-year cumulative probability of disability improvement of 33.1% and of worsening 27.8%.16 Furthermore, in the TOP study which provides the real-world experience of 5384 patients, 23.9% (n=1287) had confirmed disability improvement.17 In the PROTYS study, after 1 year of treatment with natalizumab 17.1% (6/35) of patients were assessed as ‘EDSS improved,’ 80% (28/35) of patients were ‘EDSS stable’ and 2.9% (1/35) of patients were ‘EDSS worsened’. These differing results may be due to the low study participant number in the PROTYS study (n=35), the different periods of analysis for EDSS (sustained for ≥12 week for PROTYS and sustained for ≥24 weeks for TOP), and differences in patient demographics (for PROTYS the median EDSS was 3.00 with a range of 1.00–5.50).17
Concerning changes in global HRQoL, we report a slight improvement in global HRQoL as measured by the MusiQoL index score. Planche et al reported a statistically significant improvement in MusiQoL in a population of patients with RRMS treated with natalizumab (n=48).28 Therein, the mean MusiQoL score increased from 58.6 at baseline to 68.1 at 1 year (p<0.001).28 The increase in MusiQoL score was significant at 6 months after baseline and remained significant but did not increase beyond a score of 69.8 over 3 years.28 It is difficult to make direct comparisons between the PROTYS study and the study of Planche et al because our analysis was restricted to comparisons between ‘EDSS improved’ and ‘EDSS stable’ groups of patients. Interestingly, mean HRQoL at baseline was higher in the PROTYS study compared with the study by Planche et al,28 and the mean MusiQoL scores in both populations of patients in both studies were approximately 70 after 1 year of natalizumab treatment. Improvements in HRQoL with natalizumab treatment have also been reported by others using evaluations other than MusiQoL.3 10 In Planche et al the HRQoL significantly improved within 6 months of treatment with natalizumab and this was sustained through 3 years of treatment.28 It is therefore conceivable that we did not detect a statistically significant difference due to the small number of patients in each EDSS group, and the comparison being restricted to ‘EDSS stable’ and ‘EDSS improved’ groups of patients.
In the post hoc analysis, it was shown that improvements observed in MusiQoL global index after 1 year of natalizumab treatment correlated with improvements in the ability to cope with symptoms, in overall health, in primary causes of sexual dysfunction (MSISQ-19) and in presenteeism (WPAI). This suggests that improvements in patient psychological well-being, resolution of MS symptoms including fatigue and sexual dysfunction, and increases in workability may be important factors contributing to the increases in overall QoL.
Our results aligned with those of Planche et al, who reported that improvements in MusiQoL were mainly driven by the subparameters ‘symptoms’, ‘activity of daily living’, ‘psychological well-being’ and ‘coping’.28 The improvements in overall QoL over 1 year for patients initiating natalizumab in the PROTYS study are consistent with prior reports of natalizumab treatment effects on QoL.3
In a recent study—also on Swiss patients with MS—use of the EuroQol 5 Dimension (EQ-5D) and EQ-VAS showed that fatigue, depression and spasticity were important contributors to disease burden at a population level. For RRMS, the EQ-VAS was mostly impacted by balance problems, depression, dizziness and spasticity.6 Although in the PROTYS study the ‘EDSS improved’ group had significantly greater improvements in EQ-VAS compared with the ‘EDSS stable’ group (mean change=14.5 vs −0.1, p=0.011), the post hoc analysis revealed no correlation between change of MusiQoL global index and changes of EQ-5D. Others have reported significant correlations between high EDSS scores and lower EQ-5D index scores.29
Even though in the PROTYS study significant correlations between MusiQoL global index and changes in EQ-5D were not found, the mean change of the ‘EDSS improved’ group may be clinically meaningful. A study by Kohn et al found the minimal clinical important difference (MCID) for the EQ-5D index scores to range from 0.050 to 0.084 with patients with severe disability having higher MCIDs than patients with mild-moderate disability.30 However, the study is limited in this aspect by the fact that these MIDs were not considered during study design, and thus this is an area where future research would be useful.
As regards sexual dysfunction, it has been shown that tertiary sexual dysfunction increases as HRQoL decreases.31 We found that the MSISQ-19 subparameter ‘tertiary’ was significantly more improved in the ‘EDSS improved’ group compared with the ‘EDSS stable’ group (mean change=-3.5 vs −0.1, p=0.029. Furthermore, the post hoc analysis showed that improvements in sexual life were correlated with the improvement of the MusiQoL global index. This was consistent with the findings in the ‘MusiQoL improved’ patients showing that improvement in MusiQoL global index correlated with the score of the MSISQ-19 for primary causes of sexual dysfunction. In addition, a negative association between the increase in ‘tertiary causes of sexual dysfunction’ score and the improvement of the MusiQoL global index was found (online supplemental tables 3,4). Significant improvements in sexual dysfunction (based on MSISQ-19) within 24 weeks of starting natalizumab treatment have also been shown in another study.32 Given that mental health aspects of HRQoL have been shown to be detrimentally impacted by sexual dysfunction,33 and that our results suggest that resolution of MS symptoms such as sexual dysfunction may be an important factor contributing to the increases in overall QoL, aspects of sexual dysfunction in patients with RRMS treated with natalizumab should be further investigated in larger studies.
This study had several limitations; slow recruitment, which led to small numbers of patients and meant that the original recruitment goals were not met, risk stratification strategies that precluded treatment with natalizumab in patients positive for JCV antibodies, and some sites reported low number of patients having disease activity enough to fulfil natalizumab indications according to the local prescribing information. This may have been affected by new MS therapies, fingolimod, alemtuzumab, teriflunomide and dimethyl fumarate, which were entering the market prior to or at the time of recruitment. The study duration was also limited to 1 year, which may have been too short to observe significant changes in some of the domains of HRQoL. Finally, the EDSS was limited to fully ambulatory patients (EDSS up to 3.5) and therefore we cannot assess impact of higher degrees of disability on HRQoL.
Conclusions
In conclusion, we report that 1 year of natalizumab treatment resulted in sustained EDSS improvement in 17.1% of patients and stable EDSS in 80% of patients. While there was no statistically significant difference in global HRQoL change (MusiQoL index score) between ‘EDSS improved’ and ‘EDSS stable’ groups of patients, natalizumab treatment did appear to improve several domains of HRQoL: fatigue, symptoms, overall health state, sexual dysfunction and work productivity, regardless of whether EDSS scores were stable or improved. The results of the post hoc analysis suggest that improvements in patient psychological well-being, resolution of MS symptoms including fatigue and sexual dysfunction, and increases in workability may be important factors contributing to the increases in overall QoL.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethikkommission Nordwest- und Zentralschweiz: EKNZ 2014-327 Participants. gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank Dr R. Mähler (Neuropraxis Wohlen, Wohlen, Switzerland), Dr P. Stellmes (Neurologie am Löwenplatz, Lucerne, Switzerland) and Dr Anke Salmen (Department of Neurology, Inselspital, Bern University Hospital and University of Bern, Switzerland) for their participation in the study as investigators. Katharina Bruppacher (Biogen Switzerland AG, Baar, Switzerland), for her help with the protocol and regulatory submissions, Melanie Barth and Melinda Farkas (Biogen Switzerland AG, Baar, Switzerland), for operational support. The authors also thank Dr Mea Holm and Lyndsey Kostadinov CMPP of Medicalwriters.com (Zurich, Switzerland) for providing medical writing support (writing and editing the manuscript) funded by Biogen Switzerland (Baar, Switzerland).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LA wrote and worked on the study protocol; was principal investigator of the study, recruited and cared for patients during the study, evaluated and interpreted data, and worked on the manuscript. CZ interpreted data and reviewed the data analysis and the manuscript. OF was involved in patient recruitment, drafting the manuscript, and interpretation of data conception and design of study. CPK was involved in patient recruitment, interpreted data, and reviewed the data analysis and the manuscript. SM worked on the study protocol, evaluated, and interpreted data, and worked on manuscript. JK, AL, CG and CV interpreted data and reviewed the data analysis and the manuscript. EV-B designed the protocol, interpreted the data, and reviewed the data analysis and the manuscript. KN wrote and worked on the study protocol, evaluated, and interpreted data, and worked on the manuscript.
Funding This study was funded by Biogen Switzerland (CHE-TYS-12-10341).
Competing interests LA has received speaker honoraria and/or travel compensation for activities with Biogen, Novartis, Bayer Schweiz AG, Teva, Merck, Sanofi Genzyme, Roche, Celgene and the Swiss MS Society (SMSG). CZ received honoraria for speaking, consulting fees, grants or travel compensation from Abbvie, Almirall, Biogen Idec, Celgene, Genzyme, Lilly, Merck Serono, Novartis, Roche, Teva Pharma. OF has received honoraria for lectures and advisory boards as well as research and travel support from Biogen, Novartis, Almirall, Bayer Schweiz AG, Teva, Merck, Sanofi Genzyme, Roche and the Swiss MS Society (SMSG). CPK has received honoraria for lectures as well as research support from Biogen, Novartis, Almirall, Bayer Schweiz AG, Teva, Merck, Sanofi Genzyme, Roche, Celgene and the Swiss MS Society (SMSG). SM received speaker honoraria and/or travel compensation for activities with Bayer Schweiz AG, Biogen, Celgene, Teva, Merck-Serono, Sanofi Genzyme, Novartis, Roche and Almirall and the Swiss MS Society (SMSG).J. Kuhle received speaker fees, research support, travel support from, and/or served on advisory boards for Swiss MS Society, Swiss National Research Foundation (320030_189140/1), University of Basel, Progressive MS Alliance, Bayer, Biogen, Bristol Myers Squibb, Celgene, Merck, Novartis, Octave Bioscience, Roche, and Sanofi. AL received financial compensation and/or travel support for lectures and advice from Almirall, Biogen Idec, Bayer, Celgene, Genzyme, Merck Serono, Novartis, Roche Teva. A Lutterotti is a co-founder of Cellerys and co-inventor on a patent held by the University of Zurich on the use of peptide-coupled cells for treatment of MS.C. Gobbi received honoraria for speaking, consulting fees, grants or travel compensation from Abbvie, Almirall, Biogen Idec, Celgene, Genzyme, Lilly, Merck Serono, Novartis, Roche, Teva Pharma. CV was an employee of Biogen Switzerland at the time of the study. EV-B is an employee of Biogen International. KN has served on advisory boards for Biogen, Novartis, Bayer Schweiz AG, Teva, Merck, Sanofi Genzyme, Roche, Celgene and the Swiss MS Society (SMSG).
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.