Article Text

Abstract
Background Homeless or precariously housed individuals live with poor health and experience premature mortality compared with the general population, yet little is known about age-related brain changes among these individuals. We evaluated whether MRI measures of brain structure are differentially associated with age and selected risk factors among individuals who are homeless or precariously housed compared with a general population sample.
Methods We compared T1-weighted and diffusion tensor imaging measures of brain macrostructure and white matter microstructure in a well-characterised sample of 312 precariously housed participants with a publicly available dataset of 382 participants recruited from the general population. We used piecewise and multiple linear regression to examine differential associations between MRI measures and between the samples, and to explore associations with risk factors in the precariously housed sample.
Results Compared with the general population sample, older age in the precariously housed sample was associated with more whole-brain atrophy (β=−0.20, p=0.0029), lower whole-brain fractional anisotropy (β=−0.32, p<0.0001) and higher whole-brain mean diffusivity (β=0.69, p<0.0001). Several MRI measures had non-linear associations with age, with further adverse changes after age 35–40 in the precariously housed sample. History of traumatic brain injury, stimulant dependence and heroin dependence was associated with more atrophy or alterations in white matter diffusivity in the precariously housed sample.
Conclusions Older age is associated with adverse MRI measures of brain structure among homeless and precariously housed individuals compared with the general population. Education, improvements in care provision and policy may help to reduce the health disparities experienced by these individuals.
- ACQUIRED BRAIN INJURY
- ALCOHOL-RELATED PROBLEMS
- CONCUSSION
- HEAD INJURY
Data availability statement
No data are available. Data cannot be made publicly available due to possible privacy breaches and other ethical and legal obligations to the study participants. Inquiries regarding data use or data sharing can be made to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Individuals who are homeless or precariously housed have a higher burden of illness as compared with the general population.
WHAT THIS STUDY ADDS
This is the first study to look at differential associations between quantitative MRI measures of brain health and age among these individuals compared with the general population. In this cross-sectional analysis of 694 participants, we found that older age was more strongly associated with adverse MRI measures of brain structure among those who were precariously housed compared with the general population.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Care providers should be aware of the differences in brain health and consider earlier evaluation and intervention, with traumatic brain injury and substance dependence being especially important brain health factors to consider. Policy-makers should consider increasing targeted availability and/or expanded eligibility of supportive services.
Introduction
Individuals who are homeless experience disproportionately high morbidity and mortality compared with the general population,1 and individuals who are precariously housed face similar mortality as those who are homeless.2 Previous studies report considerably higher rates of communicable diseases,3 mental illness4 and substance misuse, as well as high rates of unintentional injury such as falls, assault and traumatic brain injury.5 6 Previous studies also report higher rates of non-communicable diseases, cognitive impairment and age-related conditions, which some have taken as evidence for accelerated ageing.5 Indeed, homeless individuals over the age of 50 have a high prevalence of ‘geriatric syndromes’, comparable with general population samples more than 20 years older.7 8
There is preliminary evidence for differential brain changes in homeless and precariously housed samples, with a higher-than-expected prevalence of stroke and nearly one-third having pathological findings visible on MRI.9 10 Only one study to date has looked at quantitative MRI in homeless individuals compared with a control group and found that homeless individuals had smaller thalamic and brainstem volumes compared with controls, and that history of traumatic brain injury was associated with lower volumes of various brain structures compared with those without traumatic brain injury.11 However, this study was limited in sample size (nhomeless=25, ncontrol=26) and reported only basic between-group differences in volume across a few regions of interest. To date, it is unknown whether MRI measures of brain structure differ between homeless or precariously housed individuals compared with the general population, or whether there is a differential association with age that could indicate accelerated degenerative processes. If there are differential associations between MRI measures of brain structure and age, there are potential implications for education, public health policy and health delivery, especially given the ageing homeless population.12
In this study, we evaluated whether age is differentially associated with MRI measures of brain structure in a well characterised sample of individuals who are precariously housed (n=312) compared with a publicly available sample of individuals from the general population (n=382). We hypothesised that older age would be associated with greater whole-brain atrophy and differential white matter diffusivity among precariously housed individuals compared with the general population. We characterised differential associations with age across regions of interest and also explored whether risk factors that are over-represented in homeless or precariously housed samples, such as mental illness diagnoses, substance dependence, intravenous drug use, HIV, traumatic brain injury or stroke, were associated with atrophy or white matter diffusivity in the precariously housed sample.
Methods
Study samples and participants
The Hotel Study is a prospective longitudinal observational study of individuals who are precariously housed in an impoverished neighbourhood of Vancouver, Canada.10 13 14 Participants were recruited from single-room occupancy hotels, a downtown community court and a local hospital emergency department and were assessed monthly and yearly on various aspects of health and functioning, including one or more multimodal MRI scans of the brain. Inclusion criteria included being aged 18 or older, ability to speak English and ability to provide informed consent; no other exclusion criteria were applied. Participants in this study are demographically similar to studies on homelessness and have comparable health characteristics.15 16 Mental illness and substance use diagnoses were assessed using the best estimate clinical evaluation and diagnosis form by study psychiatrists,17 HIV status by baseline serology and traumatic brain injury was operationalised as being struck in the head, neck or face, and losing consciousness for any period of time, as assessed through a structured interview. MRI scans were acquired for research purposes and not for any specific clinical indication. Any clinically significant incidental findings were reported to the participants and their care providers. Of the 515 participants enrolled in the broader study, we included baseline data from participants between the ages of 18 and 65 who had a T1-weighted and diffusion tensor imaging (DTI) scan of sufficient quality to be analysed (n=312). Age 65 was selected as an upper bound as it aligns with the Canadian Government (and commonly used) cut-off between adulthood and older adulthood.18
Data from the general population was collected as part of the population-based and open-access Cambridge Centre for Ageing and Neuroscience repository (CamCAN; http://www.mrc-cbu.cam.ac.uk/datasets/camcan/).19 20 The CamCAN dataset was selected as it is a comparably large dataset with all imaging acquired on a single MRI scanner. To facilitate comparison to the Hotel Study sample, we included participants who were between the age of 18 and 65 who had a T1-weighted and DTI scan of sufficient quality to be analysed (n=382). In supplementary analyses, we also evaluated an additional healthy control sample that was acquired on the same scanner, with the same acquisition parameters as the Hotel Study sample (n=35), and processed identically to Hotel Study scans. These additional scans were acquired as part of a control sample for a different study and thus, there was no blinding of participant group required for research staff.
Neuroimaging acquisition and processing
For the Hotel Study sample, T1-weighted and diffusion tensor imaging scans were acquired on a 3T Philips Achieva scanner with an eight-channel SENSE head coil and for the CamCAN sample all scans were acquired on a 3T Siemens TIM Trio scanner with a 32-channel head coil. Scan acquisition parameters are detailed in the online supplemental methods.
Supplemental material
All scans were processed using similar processing pipelines. T1-weighted scans were processed using FreeSurfer V.6.021 with full processing and quality control details outlined in the online supplemental methods. Tissue-to-intracranial volume ratio was derived by dividing total cerebral brain tissue volume (excluding the ventricles, cerebellum and brainstem) by estimated intracranial volume. Cortical thickness was extracted according to the Desikan-Killiany atlas22 and subcortical volumes were extracted according to the standard FreeSurfer subcortical segmentation atlas.23 Hotel Study DTI scans were processed using FSL V.5.0.11 and CamCAN DTI scans were processed with FSL V.6.0 (https://fsl.fmrib.ox.ac.uk),24 with full processing and quality control details outlined in the online supplemental methods. Mean whole-brain fractional anisotropy (FA) and mean diffusivity (MD) data were extracted by taking an average from the white matter skeleton, and values across white matter tract regions of interest were exported according to the Johns Hopkins University white matter tract atlas.25 In general, decreased FA and increased MD is indicative of damaged or degraded white matter integrity, and this pattern is generally seen with increasing age.26 However, DTI findings are not specific to any particular pathology and can change throughout a disease process, and thus, conservative interpretation about the exact meaning of DTI measures is required.26 Therefore, we constrain our interpretation of our DTI findings to ‘alterations in diffusivity’ rather than making any direct interpretations about the underlying brain pathology.
Statistical analysis
We tested for differences between samples in median age with a Wilcoxon rank-sum test, and for differences in the proportion of sex between samples with a χ2 test. We centred all MRI measures in each sample to the sample mean (ie, CamCAN values were centred on the CamCAN sample mean for that metric) and standardised the data. We report standardised beta weights throughout to facilitate comparison across imaging metrics and samples. We first looked at broad, whole-brain measures including tissue-to-intracranial volume ratio, cerebral white matter volume, cortical volume, subcortical grey matter volume, average whole-brain FA and average whole-brain MD. We describe the difference in average slope between age and these whole-brain measures using multiple linear regression with a sample×age interaction term. However, there were non-linear associations between age and several whole-brain measures. Quadratic terms improperly describe non-linear relationships in cross-sectional studies27 and other non-linear methods (eg, general additive models) yield coefficients that are challenging to interpret and compare across measures or samples. Therefore, we used piecewise regression to algorithmically estimate the age at which the breakpoints occurred and estimate slopes before and after the breakpoint.28 We also evaluated differential associations between age and cortical thickness, subcortical volumes and white matter diffusivity across regions of interest using multiple linear regression with sample×age interaction terms. As shown in online supplemental figure 1, linear approaches provided good estimates of average slope across the lifespan compared with non-linear approaches, so we used linear models to characterise region of interest results with one single standardised value for each region of interest. As shown in online supplemental figure 2, the slope for whole-brain atrophy in the CamCAN sample was not significantly different from the healthy control sample acquired on the same scanner as the Hotel Study sample. Therefore, we use the CamCAN sample as the primary comparator throughout due to the larger sample size. We covaried for estimated intracranial volume for all volumetric measures except for tissue-to-intracranial volume ratio and we covaried for sex for all measures. All region of interest analyses were corrected for multiple comparisons to a false discovery rate of p<0.05.
One major factor that could disproportionately influence our results are individuals who had structural lesions due to traumatic brain injury, a subgroup which is over-represented in the precariously housed sample compared with the general population.29 To evaluate whether our results were largely driven by these individuals, we first created a lesion overlap figure to describe the distribution and overlap of the lesions. We manually drew the lesion mask for each participant in FSL using T1-weighted and FLAIR images that were coregistered and then non-linearly registered the T1-weighted images and lesion masks to the MNI-152 standard space. To run the sensitivity analysis, we removed these participants and ran identical models to our original analyses. A second subgroup that could potentially influence our results are individuals who had MRI evidence of stroke. This has been characterised previously in detail in a largely overlapping sample of participants, but in general the strokes were relatively small and either lacunar or cortical.9 As the strokes were generally small, we did not create a lesion overlap figure but we did re-run our analyses with these participants removed.
Finally, we explored whether factors such as mental illness diagnoses, substance dependence, intravenous drug use, HIV positivity, traumatic brain injury or stroke were associated with tissue-to-intracranial volume ratio or mean whole-brain FA in the precariously housed sample. To account for missing data, we used multiple imputation as described in the online supplemental methods. We used multiple linear regression with an age2 term to account for the non-linear relationships of the imaging variables with age, and then successively added blocks of variables.
All statistical analyses were conducted in R V.4.0.4,30 with piecewise regression implemented using the segmented package,31 region of interest results displayed using the ggseg package32 and multiple imputation performed using the mice package.33
Results
The total sample included 694 participants, with 382 from the general population (CamCAN) sample and 312 from the precariously housed (Hotel Study) sample. The general population sample was slightly older (44.2 vs 41.8; W=67 022, p=0.0047) and had a lower proportion of males (47.6% vs 78.8%; χ2=69.4, p<0.0001), and all subsequent analyses were adjusted for age and sex.
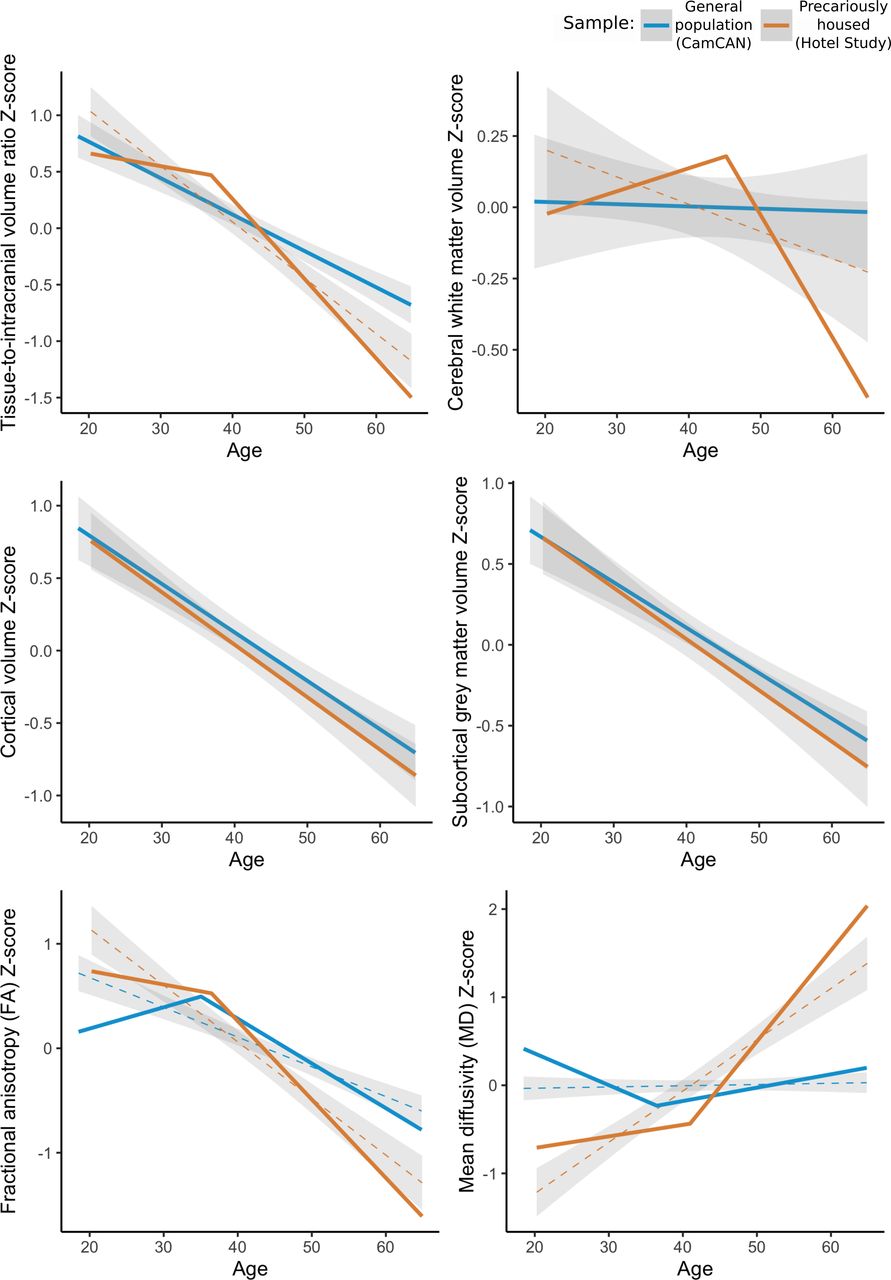
The crude relationships between whole-brain imaging outcomes and age for each sample are shown in figure 1, with adjusted estimates reported in-text and in online supplemental table 1. Older age was associated with whole-brain atrophy in both samples; however, the precariously housed sample had a stronger association than the general population (β=−0.20, p=0.0029). The relationship between atrophy and age was linear in the general population and non-linear in the precariously housed sample, where older age was associated with more atrophy after age 37.0 (95% CI=30.0 to 44.0). The association between age and atrophy was 6.5 times the slope before age 37 and approximately two times the magnitude of association as in the general population.
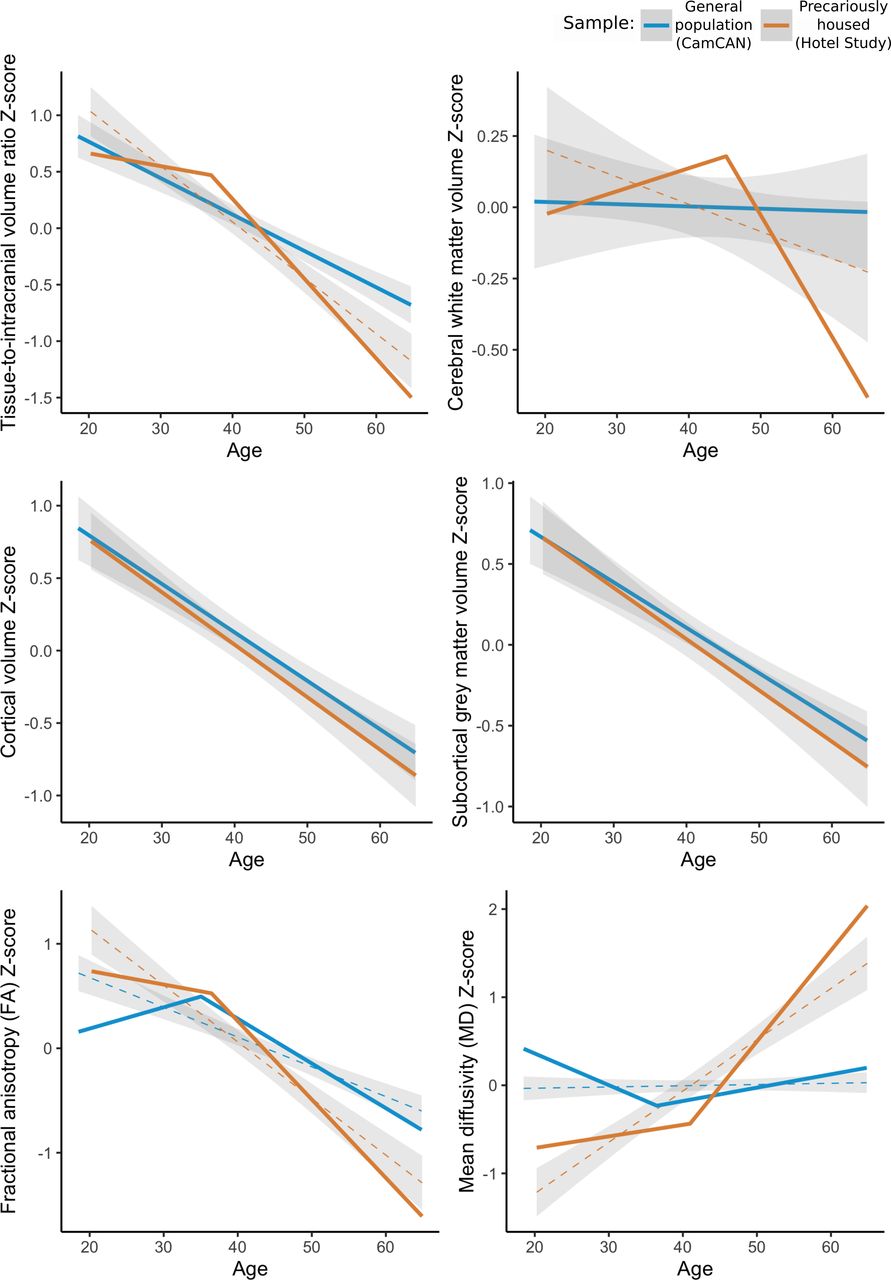
Whole-brain measures in the general population sample (Cambridge Centre for Ageing and Neuroscience (CamCAN); blue) and in the precariously housed sample (Hotel Study; orange). Each metric is centred to the mean of the respective sample and standardised. For linear relationships, a linear fit and shaded 95% CI is shown. For non-linear relationships, the piecewise regression estimates are shown with a dashed linear (+ 95% CI) fit shown for reference.
The differential atrophy in the precariously housed sample appeared to be largely driven by cerebral white matter volume (β=−0.12, p=0.0015), as neither cortical volume (β=−0.049, p=0.16) nor subcortical grey matter volume (β=−0.060, p=0.19) were significantly different in slope compared with the general population, and both declined linearly in each sample. The relationship between age and cerebral white matter volume was linear in the general population and stable across the age range. In contrast, the relationship was non-linear in the precariously housed sample as older age was associated with higher cerebral white matter volume up to age 39.8, after which it was associated with lower cerebral white matter volume.
There was also a stronger association between age and both whole-brain FA (β=−0.32, p<0.0001) and whole-brain MD (β=0.69, p<0.0001) in the precariously housed sample relative to the general population, with non-linear relationships in both samples for each metric. After age 36.4 in the precariously housed sample, older age was associated with lower FA at a magnitude 5.7 times that of the association before the breakpoint and approximately two times that of the general population at a similar age. After age 43.4 in the precariously housed sample, older age was associated with higher MD at a magnitude 5.4 times that of the association before the breakpoint and 7.9 times that of the general population at a similar age.
Differential associations with age for cortical thickness, subcortical volumes and white matter tract diffusivity between the two samples is shown in figure 2, with full results reported in online supplemental table 2–4. In the precariously housed sample compared with the general population, older age was associated with lower cortical thickness in the middle and inferior temporal areas bilaterally, temporal poles and the middle frontal and medial orbitofrontal areas, lower corpus callosum volume, higher third and lateral ventricle volumes, lower FA in 16 of 20 tracts and higher MD in 14 of 20 tracts.

Differential associations across cortical, subcortical and white matter regions of interest between the general population and precariously housed sample. Beta weight is the standardised beta from a sample×age interaction term for each region in the Desikan-Killiany atlas (top panel, left), FreeSurfer subcortical atlas (top panel, right) and Johns Hopkins University white matter atlas (bottom panel). Positive (blue) beta weights indicate that the relationship between the imaging metric and age is more positive in the precariously housed sample compared with the general population and negative (red) beta weights indicate that the relationship between the imaging metric and age is more negative in the precariously housed sample compared with the general population. FA, fractional anisotropy; MD, mean diffusivity.
Overall, 19 of the 312 precariously housed participants (6.1%) had MRI evidence of encephalomalacia attributable to traumatic brain injury, figure 3. Traumatic brain injury lesions most commonly affected the frontal and orbitofrontal regions, as well as the temporal poles, consistent with the known vulnerability of these regions to trauma.34 Additionally, 17 (5.4%) of the precariously housed participants had MRI evidence of stroke, which has been characterised in detail previously.9 There were no substantive changes in the nature or direction of our findings with either of these subgroups removed (online supplemental table 5 and online supplemental figures 3–5), indicating that our results are not unduly driven by individuals with MRI evidence of traumatic brain injury or stroke.

Overlap of lesions determined to be caused by traumatic brain injury in the precariously housed sample. Lesions are projected on the MNI-152 1 mm template. Yellow/white denotes higher number of lesions overlapping.
Finally, we explored whether factors such as mental illness diagnoses, substance use, intravenous drug use, HIV, history of traumatic brain injury or MRI evidence of stroke were associated with atrophy or whole-brain FA in the precariously housed sample. The final blocks showing all risk factors we explored are shown in figure 4 and the preliminary models and full results are reported in online supplemental tables 6 and 7. Male sex (β=−0.47, p=0.00049) and history of traumatic brain injury (β=−0.35, p=0.0017) were independently associated with greater atrophy. Heroin dependence was associated with lower FA (β=−0.28, p=0.031) and stimulant dependence was associated with higher FA (β=0.34, p=0.034). MRI evidence of stroke fell just outside of statistical significance for both tissue-to-intracranial volume ratio (−β=0.42, p=0.056) and mean whole-brain FA (β=−0.47, p=0.054).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of the associations between risk factors and tissue-to-intracranial volume (left) and risk factors and mean whole-brain fractional anisotropy (right). Error bars denote the 95% CI for the regression estimate. NOS, not otherwise specified.
Discussion
In this study, we found that older age was associated with decreased MRI measures of brain structure among individuals who were homeless or precariously housed compared with the general population. We also found that male sex and history of traumatic brain injury were associated with more atrophy in the precariously housed sample, and that stimulant and heroin dependence were associated with altered white matter diffusivity.
The process of ageing is generally understood to be complex and involves progressive allostatic load leading to physiologic and functional decline.35 36 The decline of MRI measures of brain structure is part of the normal course of ageing in the general population and there is an accelerated decline in senescence.37–40 However, we show that homeless or precariously housed participants have an age-associated decline that occurs earlier and in greater magnitude of that seen in the general population. Our results most likely reflect the effects of both systemic factors (eg, lack of housing) and individual factors (eg, development of mental illness, bodily injury) that accumulate and interact across the lifespan. This accumulation may result in accelerated brain changes where MRI measures of brain structure decline earlier among homeless or precariously housed individuals, similar to the accelerated decline with senescence seen in older adults in the general population. This is supported by studies that have found a higher prevalence of other age-related conditions such as geriatric syndromes,7 8 multimorbidity10 and earlier mortality.2
Our results could also be partly due to the development of pathological conditions that are distinct from normal ageing. Brain atrophy, as assessed by structural neuroimaging, is a non-specific biomarker for conditions such as Alzheimer’s disease41 42 and cerebral small vessel disease.43 44 Greater atrophy with age in our study may be indicative of a neurodegenerative process, especially among older participants. This is supported by previous research that has found that pathological conditions more often seen in older adults are also more common in this sample, with 46% having any neurological illness, 19% having a movement disorder and 11% with a history of stroke.9 10
History of traumatic brain injury was associated with additional atrophy in the precariously housed sample which is congruent with studies that have found a range of neuroimaging changes, including atrophy, in individuals from the general population after traumatic brain injury.45 46 We also found that stimulant and heroin dependence were associated with altered whole-brain white matter diffusivity. Previous studies report mixed findings and that the direction of the association between substance use and structural MRI measures depends on the specific substance and the region of interest.47 48
Our work has potential implications for care providers, policy-makers and researchers. First, care providers should be aware of this differential decline in MRI measures of brain structure and consider earlier evaluation and intervention for individuals experiencing homelessness or precarious housing. History of traumatic brain injury and substance dependence represent especially important factors to consider, and our work highlights the importance of accurate medical and injury history when working with vulnerable groups, especially given the association between traumatic brain injury and homelessness.6 49 Second, our study contributes to the growing evidence showing a high burden of functional impairment, morbidity and mortality among these individuals. Policy-makers should consider increasing targeted service availability, or expanding service eligibility; for example, making supportive services targeted for seniors in the general population available to individuals in these groups at a younger age. Finally, future research should characterise predictors of longitudinal change in these groups and evaluate how changes in brain structure are associated with functioning. Age-related decline in cognitive function, for example, is associated with adverse changes in MRI measures of brain structure,38 and thus, our results likely partially explain the well-documented cognitive and functional impairments experienced by these individuals.50 51 Intervention studies specifically informed by the unique health challenges of this population (eg, earlier targeted cerebrovascular risk factor management strategies including non-traditional risk factors such as intravenous drug use9 are also warranted in an effort to improve overall health.
Limitations
While our study leverages a well-characterised sample of precariously housed individuals and a large open-access sample from the general population, our work has several limitations. First, the two samples were acquired on different scanners with different acquisition parameters, and thus, comparison of the intercepts or ‘main effects’ could be biased by differences between scan acquisitions.52 Therefore, we restricted our analyses to look only at the difference in slope between samples. Imaging metrics could be different in intercept but not slope in the precariously housed sample compared with the general population; however, future work with larger control samples acquired on the same scanner is needed to appropriately evaluate these relationships. Second, while quantitative MRI has been used extensively to evaluate brain structure in vivo, it is important to acknowledge that MRI measures of brain structure may be biased by a variety of factors and are not fully representative of the underlying biology.53 Third, we used a cross-sectional approach to facilitate comparison to the general population. However, cross-sectional studies cannot evaluate what factors are associated with change over time, which may represent particularly important targets for intervention. Additionally, the Hotel Study and CamCAN samples were not rigorously matched on demographic or clinical variables, though we covaried for age and sex in all analyses. Rather, our aim was to use the CamCAN sample as a reference sample for what is normally expected in the general population and then to evaluate specific risk factors within the Hotel Study sample. There are also additional unmeasured variables (eg, acute illness) that could affect MRI measures of brain structure and introduce bias into our results. Future work with closely matched comparison samples will be able to further delineate the specific effects of risk factors on the brain structure of these individuals. Finally, we restricted our exploratory analyses on predictors of atrophy and FA to whole-brain measures. It is possible that some factors are associated with alterations in specific regions of interest but not with whole-brain measures. Additionally, co-use of substances is common, and our substance use variables were generated using a physician-assigned diagnosis of dependence (rather than any history of use). Future studies are needed to characterise the focal brain changes and dose–response characteristics associated with these risk factors.
Conclusions
Older age is associated with adverse MRI measures of brain structure among individuals who are homeless or precariously housed well beyond the normal pattern seen in the general population. History of traumatic brain injury and substance dependence are factors that are over-represented among these individuals and associated with further atrophy and alterations in white matter diffusivity. Changes in care provision and policy are needed to address the disparity in health outcomes for individuals experiencing homelessness and precarious housing.
Data availability statement
No data are available. Data cannot be made publicly available due to possible privacy breaches and other ethical and legal obligations to the study participants. Inquiries regarding data use or data sharing can be made to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The Hotel Study was approved by the research ethics board at the University of British Columbia (H08-00521), the CamCAN study was approved by the Cambridgeshire 2 Research Ethics Committee (10/H0308/50) and the additional healthy control data was derived from a study approved by the University of British Columbia (H13-02340). Informed consent was obtained from all participants, and the planned disclosure of clinically significant findings to participants and care providers was part of the consent process and approved by the Research Ethics Board at the University of British Columbia. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JLS led the processing and analysis of the neuroimaging data, conducted the statistical analyses and led the writing and revision of the manuscript. FV-R, OL and WM contributed to data collection. DW, RCYC, AET, MLH, WS, DJL and TSF contributed to data curation and quality control. AAJ gave guidance on statistical analyses. WGH and WJP gave guidance on analyses and interpretation. AET, AMB, AR, WGH and WJP contributed to funding, and all authors participated in the writing and revision of the manuscript. WJP was the senior author and guarantor of the work.
Funding Funding support for the Hotel Study includes the Canadian Institutes of Health Research (MOP-137103, MOP-390996, PJT-169094) and the BC Mental Health and Substance Use Services Research Institute. Data collection and sharing for this project for the CamCAN sample was provided by the Cambridge Centre for Ageing and Neuroscience. CamCAN funding was provided by the UK Biotechnology and Biological Sciences Research Council (grant number BB/H008217/1), together with support from the UK Medical Research Council and the University of Cambridge, UK.
Competing interests TF is supported by a Sauder Family/Heart and Stroke Professorship of Stroke Research, the Heart and Stroke Foundation of Canada and the Michael Smith Foundation for Health Research. FV-R receives research support from CIHR, Brain Canada, Michael Smith Foundation for Health Research, Vancouver Coastal Health Research Institute and Weston Brain Institute for investigator-initiated research, philanthropic support from the Seedlings Foundation, in-kind equipment support for this investigator-initiated trial from MagVenture, and has received honoraria for participation in an advisory board for Janssen. WH has received consulting fees from Translational Life Sciences, Guidepoint and AbbVie for work unrelated to the Hotel Study. All other authors have no disclosures.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.