Article Text

Abstract
Objective: To evaluate avidity of IgG anti-β2-glycoprotein I antibodies (anti-β2-GPI) in patients with antiphospholipid syndrome (APS) and systemic lupus erythematosus (SLE) in relation to thrombosis, and to demonstrate a possible affinity maturation of IgG anti-β2-GPI during the disease course.
Methods: 64 sera from 32 patients (18 with primary or secondary APS, 14 with SLE without APS) and their respective IgG fractions or affinity purified anti-β2-GPI were studied by anticardiolipin (aCL) and anti-β2-GPI enzyme linked immunosorbent assay and by chaotropic assay.
Results: Six, 12, and 14 patients had high, low, and heterogeneous avidity IgG anti-β2-GPI, respectively. In 12 patients an increase in antibody avidity was observed over a period of between four and 12 years. More patients with APS were in the high avidity than in the low avidity anti-β2-GPI group, while the opposite was observed for SLE alone (both p<0.05). The most common clinical feature among patients with high avidity anti-β2-GPI was thrombosis, mainly venous thrombosis (p<0.05 and p<0.02, respectively, v the low avidity anti-β2-GPI group).
Conclusions: Patients with APS with or without SLE may have anti-β2-GPI of high, low, or heterogeneous avidity. High avidity anti-β2-GPI appear to be associated with thrombosis and APS, while in pure SLE low avidity anti-β2-GPI may prevail. Monitoring of avidity may help elucidate the role of anti-β2-GPI affinity maturation in the pathogenesis of APS.
- aCL, anticardiolipin antibodies
- anti-β2-GPI, anti-β2-glycoprotein I antibody
- APS, antiphospholipid syndrome
- SLE, systemic lupus erythematosus
- anti-β2-glycoprotein I antibodies
- antiphospholipid syndrome
- chaotropic test
Statistics from Altmetric.com
- aCL, anticardiolipin antibodies
- anti-β2-GPI, anti-β2-glycoprotein I antibody
- APS, antiphospholipid syndrome
- SLE, systemic lupus erythematosus
Anti-β2-glycoprotein I antibodies (anti-β2-GPI) represent one of the main subgroups of anticardiolipin antibodies (aCL) associated with antiphospholipid syndrome (APS). Several reports have suggested that anti-β2-GPI either recognise conformational and cryptic epitopes on β2-glycoprotein I (β2-GPI)1–3 or bivalently bind two antigen molecules in close proximity.4,5 The equilibrium binding constants of bivalent antibodies may vary over four orders of magnitude,6 partially reflecting the non-linear association between affinity and avidity.7 The measured affinity in such cases is a function of the experimental protocol. Although the avidity of anti-β2-GPI has not been studied extensively,8–10 these antibodies are generally believed to be of low avidity (affinity).11–13 High antigen density is one of the crucial requirements for the binding of low affinity antibodies, depending upon enhanced avidity provided by bivalent attachment to the antigen.14,15 High avidity of anti-β2-GPI has been reported as a distinguishing feature in leprosy, in contrast to low avidity anti-β2-GPI found in human APS.10 β2-GPI dependent aCL, showing high avidity, have been detected in mice.16
The aims of our study were first, to determine affinity/avidity of anti-β2-GPI in patients with APS and/or systemic lupus erythematosus (SLE); second, to demonstrate possible affinity maturation of IgG anti-β2-GPI during the disease course; and third, to relate high avidity IgG anti-β2-GPI to thrombotic events.
METHODS
Patients
Sera from 32 patients were selected from our serum bank (18 with primary or secondary APS, 14 with SLE without APS) on the basis that they had medium or high levels of IgG aCL and IgG anti-β2-GPI and at least a four year disease history (two male, 30 female; mean age 42 years, range 25 to 63). From each patient we chose two serum samples from four to 12 years apart. Patients with SLE fulfilled the criteria established by the American Rheumatism Association17 and revised by the American College of Rheumatology.18 Patients with APS fulfilled the “Sapporo” criteria.19
Detection of aCL
IgG aCL were determined in sera according to the standard aCL enzyme linked immunosorbent assay (ELISA).20,21 Briefly, polystyrene microtitre plates (Medium Binding, Costar, Cambridge, Massachusetts, USA) were coated with cardiolipin, blocked with 10% fetal calf serum (FCS) in phosphate buffered saline (PBS), and incubated with sera diluted 1:100 in FCS/PBS. Alkaline phosphatase conjugated goat anti-human IgG (ACSC, Westbury, USA) and p-nitro phenyl phosphate (Sigma, Taufkirchen, Germany) in diethanol-amine buffer were used as the detection system.
Detection of anti-β2-GPI
Anti-β2-GPI were measured with our in-house ELISA as described recently,22 and evaluated through the European Forum for aPL.23 Briefly, polystyrene microtitre plates (High Binding, Costar) were coated with β2-GPI in PBS and incubated with sera diluted 1:100 in PBS containing 0.05% Tween (PBS-Tween). The detection system was the same as in the aCL ELISA.
Detection of other autoantibodies
Antinuclear antibodies (ANA) were detected by indirect immunofluorescence on HEp-2 cell line substrate (Immuno Concepts, Sacramento, California, USA).24 Serum was considered ANA positive when clearly discernible nuclear staining was observed at a serum dilution of at least 1:40. Anti-Ro/SS-A and anti-La/SS-B antibodies were tested by counterimmunoelectrophoresis.25
Isolation of β2-GPI
β2-GPI was purified from pooled human plasma and checked by polyacrylamide gel electrophoresis, giving a single band as described recently.26 To confirm the molecular form of isolated β2-GPI, an automated N-terminal sequence analysis and sequence similarity search were carried out.26–28 The N-terminal sequence analysis gave a single homogeneous sequence, entirely equivalent to the 10 amino acid residues from the N-terminus of human β2-GPI.
Isolation of anti-β2-GPI antibodies
One gram of the CNBr activated agarose (Sigma) was allowed to swell on a sintered glass filter with 1 mM HCl; 14 mg of pure unnicked β2-GPI in 0.1 M NaHCO3/0.5 M NaCl, pH 8.3 were coupled to 3.5 ml of the activated agarose. The suspension was stirred by rotating for two hours at room temperature. The unreacted sites on the matrix were blocked with 0.2 M glycine. The gel was washed 10 times alternating with 0.1 M NaHCO3/0.5 M NaCl, pH 8.3 and 0.1 M acetate buffer/0.5 M NaCl, pH 4, stacked to the column, equilibrated by PBS with 0.5 M NaCl and 0.1% Tween 20, conserved with 0.02% NaN3, and stored at 4°C. IgG fractions from patients’ sera were isolated on a protein G column (Pierce, Rockford, Illinois, USA), filtered (0.2 μm), and circulated for 90 minutes at 4°C through the β2-GPI column equilibrated in PBS with 0.5 M NaCl and 0.05% Nonidet P-40. After washing with the same buffer, bound antibodies were eluted with 0.1 M glycine/4 M NaCl/0.05% Nonidet P-40 pH 2.5. Eluates were captured by a fraction collector (Pharmacia, Uppsala, Sweden) and immediately neutralised. Fractions containing anti-β2-GPI were analysed by the relevant ELISA. Repeated isolation of anti-β2-GPI from the affinity column showed that both low and high avidity antibodies were eluted from the column using 0.1 M glycine/4 M NaCl/0.05% Nonidet P-40 pH 2.5.
Avidity determination of IgG anti-β2-GPI antibodies by chaotropic assay
Microtitre plates (High Binding, Costar) coated with 50 μl/well of β2-GPI (10 mg/l in PBS, pH 7.4) were incubated for two hours at room temperature (22–26°C). After one washing with 200 μl/well of PBS-Tween, 50 μl/well of standards and samples (isolated anti-β2-GPI antibodies, IgG fractions, or whole sera) diluted 1:100 in PBS-Tween were applied in duplicate and incubated for 30 minutes at room temperature. For avidity determination of IgG antibodies, chaotropic conditions were used in ELISA during antibody binding. Samples were diluted in PBS-Tween containing increasing concentrations of NaCl: 0.15, 0.25, 0.5, 1, 2, 4, and 6 M. After four washes, 50 μl/well of alkaline phosphatase conjugated goat anti-human IgG second antibody in PBS-Tween was added. After 30 minutes of incubation at room temperature and four washes, 100 μl/well of disodium p-nitro phenyl phosphate dissolved at 1 g/l in 1 M diethanol-amine buffer (pH 9.8) were added. Following colour development, optical density was measured at 405 nm against a reagent blank with a Rainbow microtitre plate reader (Tecan, Gröding/Salzburg, Austria). The level of anti-β2-GPI for samples in PBS-Tween with physiological NaCl concentration was derived from the standard curve according to the defined dilutions of monoclonal antibodies.29
RESULTS
The avidity of IgG anti-β2-GPI was determined in all anti-β2-GPI positive patients, regardless of the antibody level. It was clearly different among the tested sera: the lowest avidity was determined in the sera in which the initial binding of anti-β2-GPI to β2-GPI (at 0.15 M NaCl) was completely abolished at 0.25 M NaCl, and the highest was in the sera in which more than two thirds of the initial binding persisted at 6 M NaCl (fig 1).

The example of high, heterogeneous, and low avidity anti-β2-glycoprotein I antibodies.
The discrimination between anti-β2GPI of high or low avidity was made arbitrarily, comparing the initial binding at 0.15 M NaCl with binding at higher salt concentrations. We selected 0.5 M NaCl as the reference concentration for comparison with the initial binding. The presence of high avidity anti-β2GPI was identified when binding at 0.5 M NaCl remained more than 70% of the initial binding. When the binding at 0.5 M NaCl decreased to 25% or less of the initial binding, low avidity anti-β2-GPI was identified. Samples which did not fulfil either of these criteria were considered to be of heterogeneous avidity (fig 1). High avidity of IgG anti-β2-GPI was present in six of the 32 patients, low in 12, and heterogeneous in 14.
To evaluate the effect of anti-β2-GPI concentration on avidity determination, two sera with high avidity antibodies were diluted stepwise in PBS from 1:100 to 1:800 and binding curves at different serum dilutions were compared. Parallelism of the curves (absorbance values as a function of salt concentration) showed that the level of anti-β2-GPI did not influence the measurement of anti-β2-GPI avidity (fig 2).

Avidity determination of anti-β2-glycoprotein I antibodies in diluted serum. mOD: absorbance ×1000.
To detect possible influence of the matrix, whole serum, IgG fraction in PBS, and isolated anti-β2-GPI in PBS from the same blood collection of selected patients were analysed simultaneously by the chaotropic assay. Comparable results (all curves ran in parallel) were obtained, indicating that the matrix did not influence the determination of high avidity IgG anti-β2-GPI (fig 3).

Effect of matrix on the detection of high avidity anti-β2-glycoprotein I antibodies. mOD: absorbance ×1000.
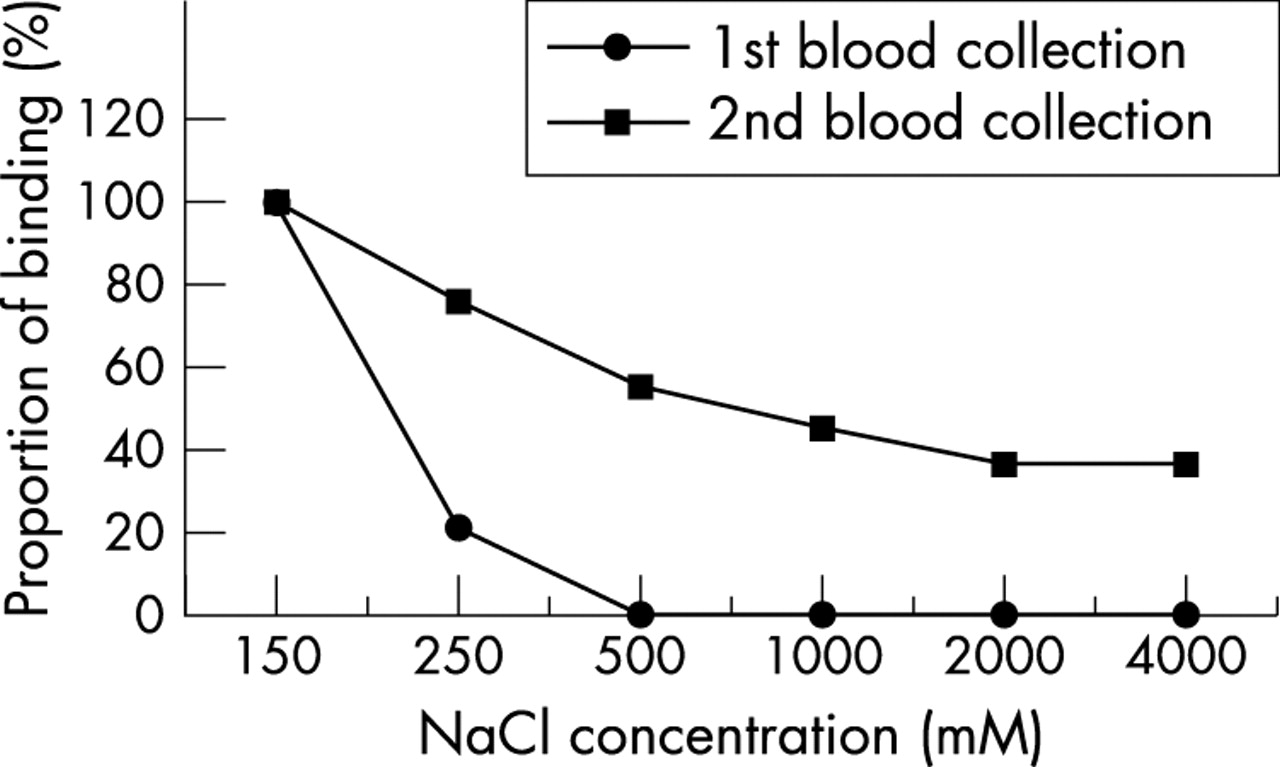
The avidity of anti-β2-GPI varied slightly over the disease course in most patients. However, in 12 of the 32 patients (38%), anti-β2-GPI avidity clearly increased during the disease course (fig 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The example of an affinity maturation of anti-β2-glycoprotein I antibodies in paired samples from the same patient but different blood collections.
Significantly more patients with APS (primary or secondary) were found in the group having high avidity anti-β2-GPI than in the group with low avidity antibodies (5/6 v 5/12, p<0.05). The distribution of clinical and laboratory features of APS and SLE among patients with IgG anti-β2-GPI of different avidity is shown in table 1.
Distribution of clinical and laboratory features of 32 patients with anti-β2-glycoprotein antibodies of high, heterogeneous, or low avidity
Thrombosis was the main clinical feature associated with high avidity anti-β2-GPI; this was predominantly venous (p<0.05 and p<0.02, respectively, v low avidity anti-β2-GPI). Kidney disease, according to the criteria for SLE, was statistically more common in the combined high + heterogeneous avidity anti-β2-GPI group than in the low avidity group (p<0.05). The limited number of patients did not allow us to correlate the avidity of anti-β2-GPI with different types of glomerulonephritis according to the WHO classification. Renal thrombotic microangiopathy was included in the section “thrombosis–microvascular changes”. It was present in one patient in each of the avidity group. Higher frequencies of livedo reticularis and central nervous system involvement were found in the group with high avidity anti-β2-GPI, but the differences compared with the low avidity group were not significant (p<0.09 and p<0.07, respectively) (table 1).
DISCUSSION
The avidity of presumably pathogenic antibodies and their affinity maturation over the disease course may have important clinical implications. Anti-β2-GPI are the most abundant among the aCL, which are serological hallmarks of APS. So far, anti-β2-GPI have generally been considered to be of low affinity, requiring bivalent binding to the antigen.4,5,10
Although great heterogeneity in avidity among samples was found, our results clearly showed that high avidity anti-β2-GPI were not rare in APS. In five of 18 APS patients (28%), they were the predominant subset of IgG anti-β2-GPI (table 1). The results of Vlachoyiannopoulos et al,8 who found a greater resistance to urea of anti-β2-GPI in APS sera compared with sera from patients with non-APS autoimmune diseases, can be interpreted in the same way. The differences in the methodology of avidity determination could account for discrepancies between our results and those reported by Arvieux et al,10 who found high avidity anti-β2-GPI in leprosy but not in APS.
In our study calculation of the “exact” dissociation constant was omitted, and the chaotropic test of a binding strength was used instead, similar to the one used by Saraux et al30 for rheumatoid factor. When the avidity of immunoglobulins of the same class is measured using the chaotropic test, the results depend only on affinity, and comparison of results within a particular analysis is thus possible. To prove that immunoglobulins other than IgG did not interfere with the binding of high avidity IgG anti-β2-GPI to the antigen, analyses were carried out for selected samples in which whole sera, IgG fractions, and isolated anti-β2-GPI from the same patients were run simultaneously. We were able to detect the presence of high avidity IgG anti-β2-GPI in whole sera, regardless of the concomitant presence or absence of the IgM isotype. We also showed that the antibody concentration (isolated anti-β2-GPI, IgG fraction, or serum) did not influence the results of the chaotropic test.
In 12 of the 32 patients an increase in antibody avidity was observed over a period of between four and 12 years. We hypothesise that autoantibody avidity was low at the start of the disease, and then increased owing to affinity maturation during the disease course. The study was not designed to correlate maturation of the anti-β2-GPI affinity with clinical features (only two samples were obtained from each patient). Affinity maturation is believed to be clinically less important in diseases where avidity of antibodies is not relevant for pathogenicity—for example, anti-acetylcholine receptor antibodies in myasthenia gravis.31 The avidity of anti-dsDNA antibodies remains constant over time,32 but their high avidity is important in the diagnosis of SLE, while low avidity anti-dsDNA can be found in other inflammatory diseases.33,34 In such cases information about affinity/avidity of the measured antibodies is essential.
We found that there were significantly more APS patients in the high avidity anti-β2-GPI group than in the low avidity group, while the opposite was true for SLE in the absence of APS. The presence of high avidity anti-β2-GPI was associated with thrombotic history, in particular with venous thrombosis. In addition, none of the 12 patients with only low avidity anti-β2-GPI experienced venous thrombosis. The lack of an association between antibody avidity and obstetric disorders may be a false negative result owing to the small number of patients with such manifestations. It is also possible that non-thrombotic pathogenic mechanisms, presumably involved in obstetric disorders, have blurred the relation between antibody avidity and pregnancy complications.35 Central nervous system involvement, livedo reticularis, and renal disease had a tendency (though this was not statistically significant) to associate with high avidity anti-β2-GPI. To clarify the relation between anti-β2-GPI avidity and non-thrombotic clinical features, studies on larger groups of patients are needed.
We noted that none of the 13 anti-Ro/anti-La positive patients possessed high avidity anti-β2-GPI. Any assumption drawn from this observation would be premature.
Conclusions
In summary, to measure the avidity of IgG anti-β2-GPI we set up a chaotropic ELISA method which is simple, reproducible, and accessible to all clinical laboratories. Its application may be useful for discriminating between high avidity anti-β2-GPI, which are predominantly present in APS patients with thrombotic events, and low avidity antibodies occurring in SLE patients without APS. Monitoring of avidity may help elucidate the role of anti-β2-GPI affinity maturation in the pathogenesis of APS.
Acknowledgments
This work was partially supported by the Ministry of Education, Science and Sport of the Republic of Slovenia, grants Nos J3-3414 and J3-3357. We express our appreciation to Aleš Ambrožič MD for his assistance in providing patients and material.