Article Text

Abstract
Patients with functional neurological disorders (FND)/conversion disorder commonly present to outpatient clinics. FND is now a ‘rule in’ diagnosis based on neurological examination findings and semiological features. While neurologists may be more comfortable diagnosing patients with FND, there is only limited guidance as to how to conduct follow-up outpatient visits. Using clinical vignettes, we provide practical suggestions that may help guide clinical encounters including how to: (1) explore illness beliefs openly; (2) enquire longitudinally about predisposing vulnerabilities, acute precipitants and perpetuating factors that may be further elucidated over time; (3) facilitate psychotherapy engagement by actively listening for potentially unhelpful or maladaptive patterns of thoughts, behaviours, fears or psychosocial stressors that can be reflected back to the patient and (4) enquire about the fidelity of individual treatments and educate other providers who may be less familiar with FND. These suggestions, while important to individualise, provide a blueprint for follow-up FND clinical care.
- conversion disorder
- functional movement disorders
- psychogenic nonepileptic seizures
- neuropsychiatry
Statistics from Altmetric.com
Introduction
Patients with functional neurological disorders (FND)/conversion disorder are common outpatient neurology referrals.1 2 Recently, there have been significant advances in the diagnostic approach for FND, emphasising a ‘rule-in’ diagnosis based on neurological examination and semiological features.3–6 There is an emerging new standard of care, one that supports therapeutic roles for education,7 physical therapy,8 occupational therapy9 and psychotherapy (particularly conventional cognitive behavioural therapy and cognitive behavioural therapy-informed psychotherapy).10–12 Despite the prevalence of FND and the boom in research, many clinicians feel ill-equipped to manage this population.13–15
One area of difficulty demystified by Carson and colleagues lies in how to deliver the diagnosis of FND, including suggestions to enhance diagnostic acceptance and address patients’ doubts.16 While treatment begins with delivery of the diagnosis, we have encountered skilled clinicians who, nonetheless, also lack clarity in how to conduct follow-up visits in patients with FND. When patients return reluctant to accept the diagnosis, show limited engagement or report that the ‘treatment is not working’ despite adequate participation, the tendency may be to redeliver the diagnosis and provide reassurance that the treatment recommendations offer the best possibility for improvement. That approach, however, if performed in isolation, misses therapeutic opportunities. Instead, we recommend using follow-up visits to explore clinical progress, evaluate reasons for potential delayed improvement and help to catalyse effective treatment engagement.
In this article, we use a ‘photo story’ platform similar to Carson and colleagues16 to provide guidance on how to conduct follow-up visits in patients with FND. Through vignettes, we present commonly encountered scenarios including how to (1) encourage an open dialogue with patients who are not accepting the diagnosis; (2) explore the evolving complexity of predisposing, precipitating and perpetuating factors; (3) catalyse psychotherapy treatment by collaboratively identifying unhelpful thoughts, maladaptive behaviours, negative emotions and/or psychosocial stressors that can be taken back to psychotherapy for additional exploration and (4) enquire about other treatment details (eg, physical therapy activities, family therapy) and help to educate providers who may be less familiar with FND.
Vignette 1. Follow-up visit in a patient not accepting the diagnosis: facilitating self-efficacy
Even when the diagnosis is confirmed and delivery of a FND diagnosis goes reasonably well using validated principles,7 16 some patients remain reluctant to accept the diagnosis of FND. Patients who initially appear receptive can subsequently show a lack of follow through with physical therapy or psychotherapy or may report an alternative explanation for their symptoms. A lack of adherence to initial recommendations should raise concern that either the patient may not be ‘buying into’ the treatment plan or there are perpetuating factors (eg, family issues, financial concerns) that require exploration. The figure 1 vignette illustrates this, where the patient was diagnosed with a functional gait disorder, yet continued to pursue antibiotics for potential Lyme disease despite an appropriate negative infectious disease workup. Of note, despite a physician’s appropriate use of open-ended and focused questions during the initial visit, it is common for patients to disclose nuanced illness beliefs in follow-up.17–19 Furthermore, patients’ participation in other subspecialty clinics may not be immediately apparent, highlighting the importance of gathering an account of the complete treatment team and previous workup.

The patient that questions the diagnosis. This vignette focuses on an individual who initially appeared receptive to the diagnosis of functional neurological disorder (FND), but at follow-up has clearly not yet accepted the diagnosis and has been non-adherent to referrals. In this context, it is important to explore transparently and non-judgmentally the patient’s illness beliefs, while also conveying the message that buy-in to the diagnosis is a critical first step in the treatment.
A patient’s hesitancy to accept the diagnosis, whether overt or indirect, can present a barrier to treatment. Some providers may worry that differences of opinion regarding the diagnosis will escalate into an argument. As such, we recommend the following suggestions with such a patient:
Ask the patient for their current understanding of their diagnosis. If they remain unclear or ambivalent, ask what they remember about the initial visit and discussion of the diagnosis. If details are incorrect, revisit the diagnosis and rationale behind treatment recommendations.
For those who clearly articulate an alternative diagnosis despite recalling the initial encounter, directly—but non-judgmentally—bring up their hesitancy. For example, ‘It seems to me that you are not quite sure we are on the right track’. Alternatively, state, ‘I see that you have some doubts; it is okay that you do, and I would like to hear your concerns’. This approach encourages patients to express their illness beliefs and allows clinicians to address concerns and recount the neurological examination and adjunct tests that ruled-in the FND diagnosis.
After encouraging an open discussion, ask the patient to report back what they heard.
Transition to treatment by emphasising that, ‘Your condition is real and common and you play an active role in the process of getting better’.
An important point is to not ‘convince’ patients of the diagnosis. Describe the clinical examination signs that informed your diagnosis and, thereafter, allow them space to do some additional reflection, while emphasising that an important first treatment step is the patient’s willingness to consider a diagnosis of FND. If the patient continues to express significant doubt, we suggest encouraging the patient to further review educational materials on websites such as www.neurosymptoms.org and www.fndhope.org (or reading other resources such as the introductory chapter of a FND-related psychotherapy treatment manual) and ask them to consider if their condition is like that described in those materials.20 Arrange a follow-up visit with the plan to continue this discussion. Emphasise that communication between providers is key for the patient’s care. With permission, offer to coordinate with subspecialist(s) to discuss the rationale and framing of the patient’s FND diagnosis. At times, the patient may elect to pursue alternative diagnoses (and/or treatments). In our practice, patients can discharge themselves from clinic and we note that they are welcome to return if they would like to revisit the diagnosis of FND.
Vignette 2. Follow-up visits as an opportunity to continue assessing predisposing, precipitating and perpetuating factors: follow the affect
Patients commonly deny psychiatric symptoms and/or psychosocial stressors during the initial encounter. The reasons include time constraints, the actual absence of stressors, lack of awareness and concerns that acknowledging emotional disturbances and/or ongoing stressors will discredit neurological complaints. Furthermore, the complexity of the patient’s presentation often may not be fully appreciated at first despite a well-conducted interview. An essential element of developing a formulation in FND is identifying predisposing vulnerabilities, precipitating events and perpetuating factors that are contributing to the patient’s condition.21 Follow-up visits provide additional opportunities to ‘look under the hood’ and to guide patients in exploring these factors.22 23
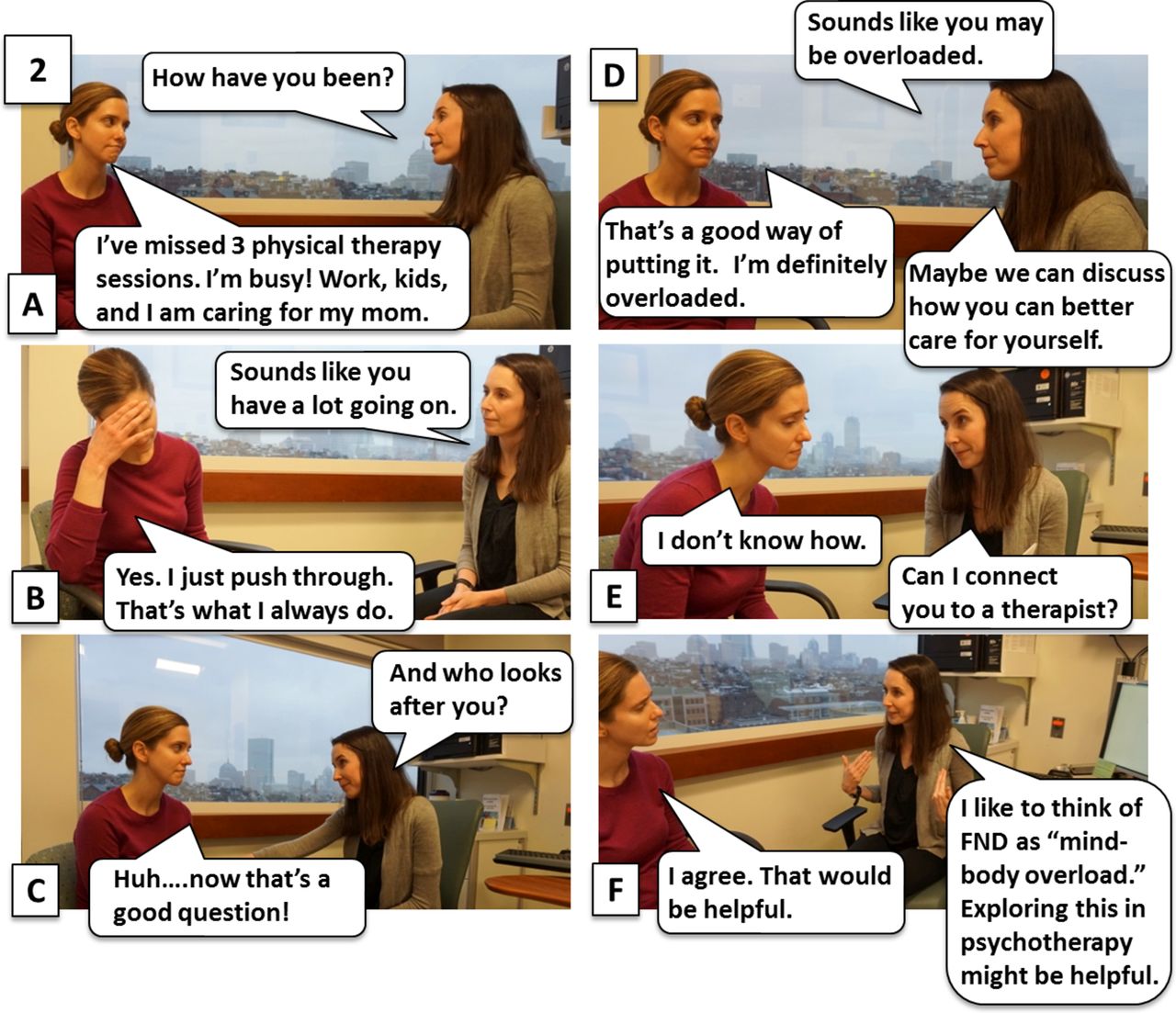
In the figure 2 vignette, we consider an individual with functional right arm tremor and weakness who has accepted the diagnosis of FND and is receptive to recommendations but reports difficulty making it to physical therapy and appears overwhelmed. She initially denied psychiatric symptoms or psychosocial stressors. Here, the physician acknowledges the patient’s affect and explores barriers to physical therapy attendance by leading with an empathic stance. By suggesting to the patient that she may be ‘overloaded’, a relatable term without stigma, the clinician can elicit relevant mood symptoms and psychosocial difficulties.
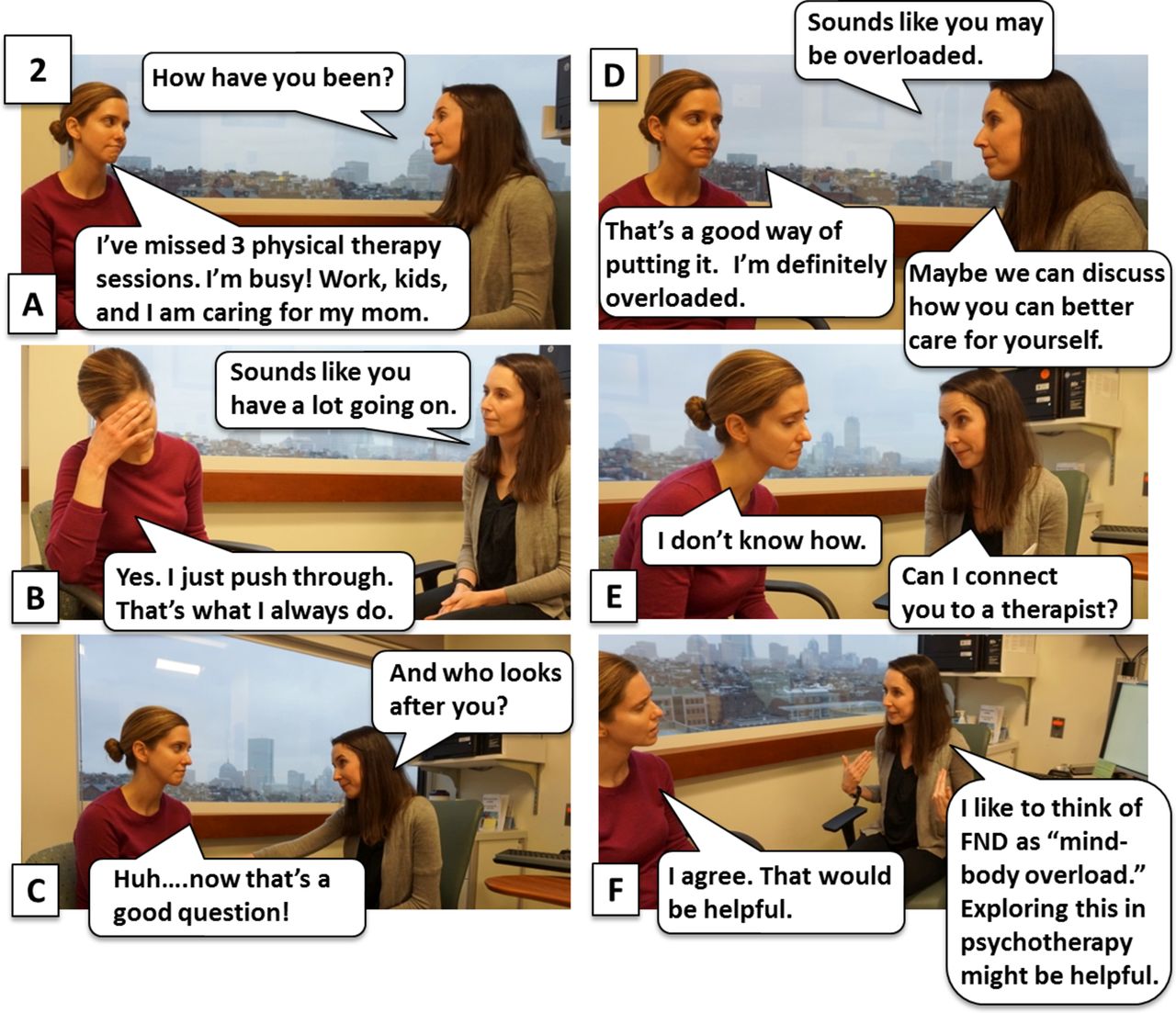
The importance of longitudinal assessments and the ‘mind–body overload’ concept. This vignette focuses on the importance of initially and longitudinally accessing for predisposing vulnerabilities, acute precipitants and perpetuating factors during outpatient care. This patient initially denied depression and anxiety; however, at follow-up, she showed an overwhelmed affect and missed several physical therapy sessions. The patient discloses that she has been caring for her ill mother. The physician takes an empathic stance and acknowledges the negative affect. She then introduces the concept of ‘mind–body overload’. This discussion allows for a well-received referral to psychotherapy. FND indicates functional neurological disorder.
This vignette highlights several perpetuating factors: the lack of social support, work-related stress and caregiver responsibilities for an elderly parent. Perpetuating factors, which among other possibilities can also include lack of acceptance of the diagnosis (first vignette) or physical deconditioning (fourth vignette), are factors that can impede or delay recovery. It is useful to listen for predisposing, precipitating and perpetuating factors throughout longitudinal care. Although exploring these factors is important for recovery, the physician should avoid explicitly identifying factors FOR the patient, but rather aid patients in making the connections for themselves. Here, the physician acknowledges the patient’s affect, introduces the ‘mind–body overload’ concept and makes a referral to psychotherapy. Lastly, the vignette briefly introduces the identification of a predisposing vulnerability for the development of FND, a tendency towards deprioritising oneself while diligently meeting others’ needs.
Vignette 3. Patient with psychogenic non-epileptic seizures in psychotherapy but not improving: physician as catalyst for psychotherapy efficacy
Having established the diagnosis of psychogenic non-epileptic seizures and having started psychotherapy, some patients report little or no improvement in seizure severity or frequency. At this point, it is useful to enquire about the details of psychotherapy sessions to ensure the fidelity of treatment and identify what can be improved. While some non-mental health clinicians may not be delivering psychotherapy directly, he or she may act as a facilitator of patient engagement in therapy. Also, discussing neurological symptoms during office visits allows a ripe opportunity to assist patients in exploring connections between seizures and maladaptive thoughts, behaviours, emotions and psychosocial factors. As the figure 3 vignette briefly illustrates, important information to gather includes:

The role of the clinician as catalyst for treatment efficacy. This vignette depicts a patient with psychogenic nonepileptic seizures in psychotherapy reporting that therapy is ‘not helping’. The focus of this conversation is an enquiry about the content discussed during psychotherapy to assess treatment fidelity. It also provides the opportunity to listen actively for brief statements that potentially reflect maladaptive thoughts, behaviours and/or fears that can be reflected back to the patient and highlighted for further exploration in psychotherapy.
The content being discussed during psychotherapy. Patients commonly focus on life stressors while not discussing the relationship to their seizures or the context in which seizures are occurring.
The patient’s understanding of the basic concepts of psychotherapy. One evidence-based modality commonly used in FND leverages cognitive behavioural therapy principles directed at target symptoms. This psychotherapy examines relationships between FND symptoms (eg, seizures) and thoughts, emotions, and behaviours/actions. If a patient shows limited ability to describe a basic cognitive behavioural therapy model midway through treatment, this warrants discussion with the patient’s therapist.
The patient’s appreciation of early warning signs or triggers, associated anxiety or fear, etc. Though not always obvious, FND may be associated with emotional and psychosocial stressors and other potentially modifiable environmental and relational factors. Such connections should be reflected back to patients with encouragement to further discuss in psychotherapy.
The patient’s use of and adherence to evidence-based treatment manuals.20 24 25 Manualised psychotherapy is common and requires the patient to work actively according to a specific protocol. Asking patients to bring in their workbook for follow-up office visits can be a practical and easy way of ensuring entry-level adherence to psychotherapy recommendations.
The physician’s interview style is also important. Certain techniques can bolster communication, enhance rapport and aid treatment adherence. Since FND can be associated with anxiety, fear, depression and psychosocial stressors, effective communication requires empathy. The patient may require validation and normalisation of their concerns so they feel encouraged and empowered. An empowered patient is better equipped for the self-exploration that effective psychotherapy demands. Asking the patient what they are learning in treatment, or how they are changing thought or behavioural patterns can encourage self-reflection and build rapport. Lastly, communication between the physician and therapist may also help to enhance efficacy and convey a unified message. For neurologists who commonly see patients with FND, it may be advisable to read one of the readily available FND workbooks to increase familiarity with and proficiency in psychotherapy principles.
Vignette 4. Inquiring about physical therapy details when a patient reports that ‘treatment is not working’: the details matter
Despite apparent adherence to physical therapy and/or occupational therapy, patients with functional movement disorders may claim that the ‘treatment is not working’. For such people, it is important to enquire about the details of each treatment modality. This requires that providers are familiar with core elements of physical and occupational therapies for FND as outlined in published recommendations8 9 to enable physicians to make a ‘big-picture’ determination about the fidelity of a given treatment.
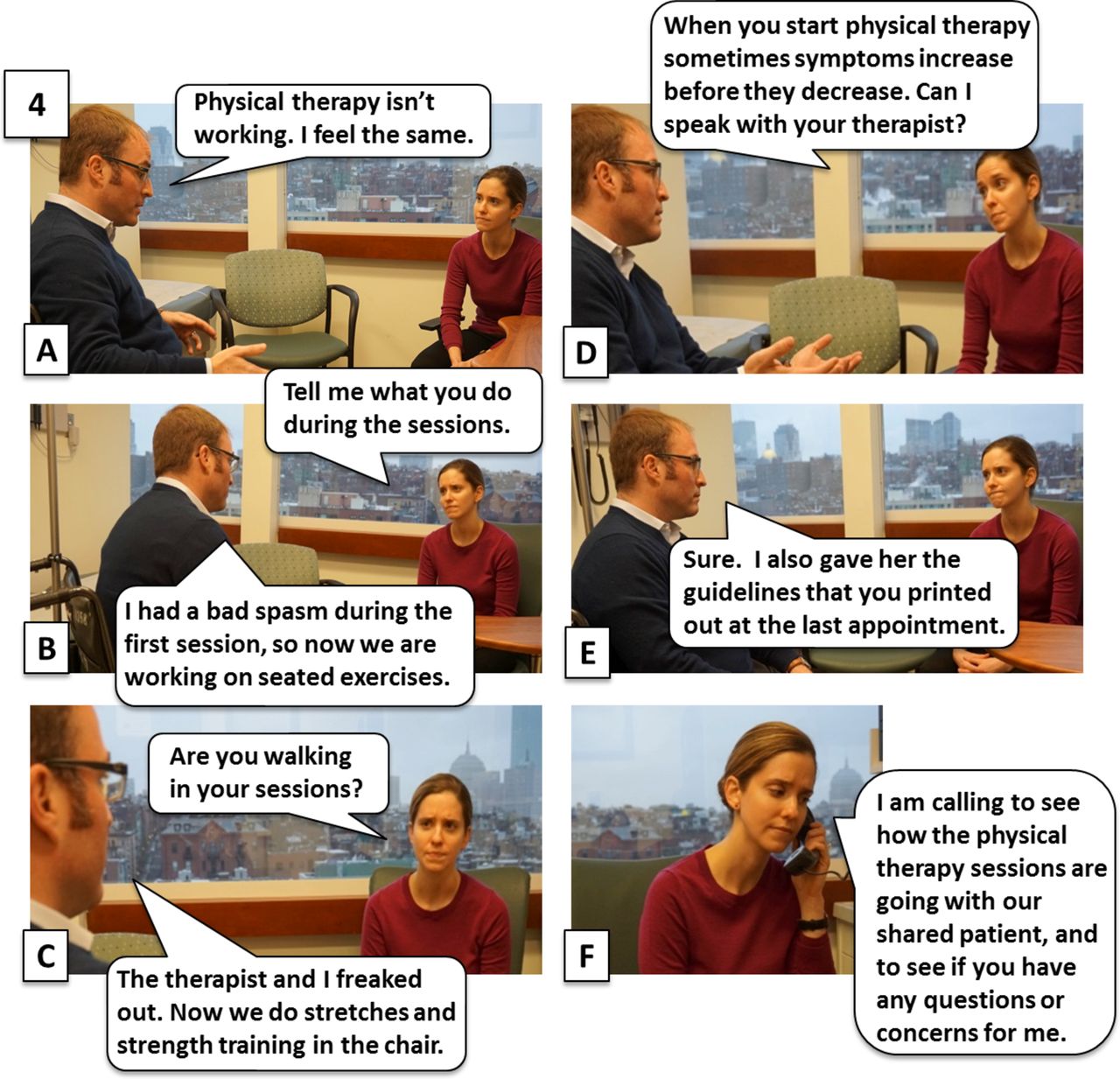
In the figure 4 vignette, the patient describes an intense full-body shaking event occurring on initial gait evaluation. Both the patient and the physical therapist at an outside facility were un-nerved; notably, the physical therapist had not previously encountered a patient with such violent shaking. Despite the patient’s clinically established functional gait disorder, subsequent physical therapy sessions focused on strength-training exercises while the patient remained seated. This identifies a perpetuating factor in patients with FND: the patient and/or physical therapist engaging in avoidance behaviours that impede recovery.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The importance of enquiring about the details of each treatment. This vignette identifies a patient reporting that physical therapy is not working. The physician asks about the specific details of sessions and learns that the therapy has been largely limited to seated exercises in the context of avoidance on the part of the patient and therapist. The physician discusses the theme of avoidance with the patient, mentioning that symptoms sometimes increase before they decrease. She then reaches out to the physical therapist to provide education and coordinate care.
For physical and occupational therapies occurring at centres less familiar with FND, we generally recommend printing the published recommendations and asking patients to provide their therapists with a copy of the pertinent article.8 9 This communicates the diagnosis of FND to the clinician and highlights the guiding treatment principles in their respective disciplines.
Patients may expect that with attendance comes improvement; however, if the therapy itself promotes maladaptive avoidance, it is unlikely to be successful. We have found it helpful to address the possibility of avoidance when making new treatment recommendations. As such, we note that, ‘sometimes symptoms increase before they decrease’ and directly highlight for patients that if FND symptoms initially ‘flare up’ this does not necessarily mean that a given treatment should be modified. For the patient in this vignette who is already engaged in avoidance behaviours, it may be helpful to address transparently the limited gait activities occurring during physical therapy and to offer to speak to the physical therapist to hear concerns and encourage effective strategies. Speaking to the physical therapist promotes interdisciplinary care and encourages an element of shared expertise important in the management of patients with FND.
Conclusion
In summary, the effective treatment of FND is a multifaceted process. It requires the clinician, who overseas treatment, to access and address issues at several levels. These may include exploring the patient’s acceptance of the diagnosis, knowledge of basic psychotherapy treatment principles and the nature of FND-specific physical or occupational therapy. Taking an empathic, non-judgmental stance and using non-pejorative language, while also acknowledging patients’ affective responses, helps to maintain therapeutic alliance. Longitudinal follow-up care may aid the identification of predisposing, precipitating and perpetuating factors. We hope to encourage clinicians, particularly neurologists, to engage this patient population in longitudinal care and to view themselves as catalysts for treatment effectiveness as part of an interdisciplinary team-based approach to the management of FND.
Key points
Clinicians are often unclear on good practices for follow-up care in patients with functional neurological disorders.
Explore transparently and non-judgmentally illness beliefs and other barriers to treatment engagement.
Continue the longitudinal exploration of predisposing vulnerabilities, acute precipitants and perpetuating factors.
Enquire about the details of psychotherapy, physical therapy and occupational therapy to ensure adherence with updated good practices.
Listen for references to unhelpful thought patterns or maladaptive behaviours that can be gently reflected to the patient to help to catalyse the efficacy of psychotherapy.
Acknowledgments
We thank Maurissa McGeary for her participation in figure 3. Additional photo credits by vignette: (1) physician: DLP, patient: CA; (2) physician: CA, patient: ENM; (3) physician: JA, patient: Maurissa McGeary; (4) physician: ENM, patient: DLP.
References
Footnotes
Contributors DLP developed the concept for this article. All authors contributed to the literature review, drafting and critical review of the manuscript.
Funding DLP was supported by the Sidney R. Baer Jr. Foundation and the Massachusetts General Hospital Physician-Scientist Development Award.
Competing interests WCL has served on the editorial boards of Epilepsia, Epilepsy and Behavior and Journal of Neuropsychiatry and Clinical Neurosciences; receives editor’s royalties from the publication of Gates and Rowan’s Nonepileptic Seizures, 3rd ed. (Cambridge University Press, 2010) and 4th ed. (2017); author’s royalties for Taking Control of Your Seizures: Workbook and Therapist Guide (Oxford University Press, 2015); has received research support from the NIH (NINDS 5K23NS45902 [PI]), Department of Defense, Rhode Island Hospital, the American Epilepsy Society (AES), the Epilepsy Foundation (EF), Brown University and the Siravo Foundation; serves on the Epilepsy Foundation Professional Advisory Board; has received honoraria for the American Academy of Neurology Annual Meeting Annual Course; has served as a clinic development consultant at University of Colorado Denver, Cleveland Clinic, Spectrum Health and Emory University and has provided medico legal expert testimony.
Patient consent Not required.
Provenance and peer review Commissioned; externally peer reviewed. This paper was reviewed by Jon Stone, Edinburgh, UK.
Other content recommended for you
- Diagnosis and management of functional neurological disorder
- Systematic review of psychotherapy for adults with functional neurological disorder
- Recognising and explaining functional neurological disorder
- Corticolimbic fast-tracking: enhanced multimodal integration in functional neurological disorder
- Myths and facts about functional neurological disorders: a cross-sectional study of knowledge and awareness among medical students and healthcare professionals in Iraq
- Decade of progress in motor functional neurological disorder: continuing the momentum
- Complex regional pain syndrome and functional neurological disorders – time for reconciliation
- Functional (psychogenic non-epileptic/dissociative) seizures: why and how?
- Functional neurological disorders: effective teaching for health professionals
- Functional neurological disorders: the neurological assessment as treatment