Article Text

Abstract
There have been many articles highlighting differences and similarities between complex regional pain syndrome (CRPS) and functional neurological disorders (FND) but until now the discussions have often been adversarial with an erroneous focus on malingering and a view of FND as ‘all in the mind’. However, understanding of the nature, frequency and treatment of FND has changed dramatically in the last 10–15 years. FND is no longer assumed to be only the result of ‘conversion’ of psychological conflict but is understood as a complex interplay between physiological stimulus, expectation, learning and attention mediated through a Bayesian framework, with biopsychosocial predisposing, triggering and perpetuating inputs. Building on this new ‘whole brain’ perspective of FND, we reframe the debate about the ‘psychological versus physical’ basis of CRPS. We recognise how CRPS research may inform mechanistic understanding of FND and conversely, how advances in FND, especially treatment, have implications for improving understanding and management of CRPS.
- complex regional pain syndrome
- reflex sympathetic dystrophy
- functional neurological disorder
- psychogenic
- conversion disorder
Statistics from Altmetric.com
- complex regional pain syndrome
- reflex sympathetic dystrophy
- functional neurological disorder
- psychogenic
- conversion disorder
Introduction
Complex regional pain syndrome (CRPS) is a disabling chronic pain condition that may follow physical injury to a limb, either through surgery or trauma. Previously, there were no clear diagnostic criteria, and a mixture of terminologies were used, such as ‘Reflex Sympathetic Dystrophy’ and ‘Causalgia’. In response to this, the International Association for the Study of Pain introduced a new terminology in an attempt to standardise diagnosis and management: CRPS type I, where there was no defined nerve lesion and type II, where there was a definite nerve lesion. These definitions have since been superseded by the Budapest clinical and research criteria (box 1).1 2 CRPS occurs in around 20 out of 100 000 patients, with more women than men being affected, most commonly in the 37–53 year age range. It is characterised by local inflammatory and autonomic dysregulation combined with trophic and motor dysfunction of the affected body part.2 Although its defining features (sensory, autonomic, motor and trophic) have been extensively studied, their pathophysiological nature and the role of the incipient event remain a matter of debate and research.2
Budapest clinical diagnostic criteria for CRPS,2 with features also seen in functional neurological disorder italicised
Continuing pain, which is disproportionate to any inciting event.
Must report at least one symptom in three of the four following categories:
Sensory: reports of hyperaesthesia and/or allodynia.
Vasomotor: reports of temperature asymmetry and/or skin colour changes and/or skin colour asymmetry.
Sudomotor/oedema: reports of oedema and/or sweating changes and/or sweating asymmetry.
Motor/trophic: reports of decreased range of motion and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic changes (hair, nail, skin).
Must display at least one sign at time of evaluation in two or more of the following categories:
Sensory: evidence of hyperalgesia (to pinprick) and/or allodynia (to light touch and/or deep somatic pressure and/or joint movement).
Vasomotor: evidence of temperature asymmetry and/or skin colour changes and/or asymmetry.
Sudomotor/oedema: evidence of oedema and/or sweating changes and/or sweating asymmetry.
Motor/trophic: evidence of decreased range of motion and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic changes (hair, nail, skin).
There is no other diagnosis that better explains the signs and symptoms.
In the debate surrounding CRPS, one conceptual schism stands out as particularly polarising and counterproductive: the role of psychological processes. This debate has typically been characterised over the years as a discussion between those who see CRPS as a genuine medical disorder and those who seek to define it as a ‘non-organic’ or ‘psychogenic’ disorder. Indeed, it was classified as hysteria minor by the so-called 'father of neurology' Jean-Martin Charcot in 1892. Within the umbrella of ‘non-organic’, there has often been little distinction between patients with a genuinely experienced functional neurological disorder (FND; also called psychogenic or conversion disorder) and those patients wilfully exaggerating symptoms for medical care or financial gain.3 4 Voluntary feigning of CRPS signs and symptoms is rarely found in cases of malingering or factitious disorder and must not be equated with FND.5
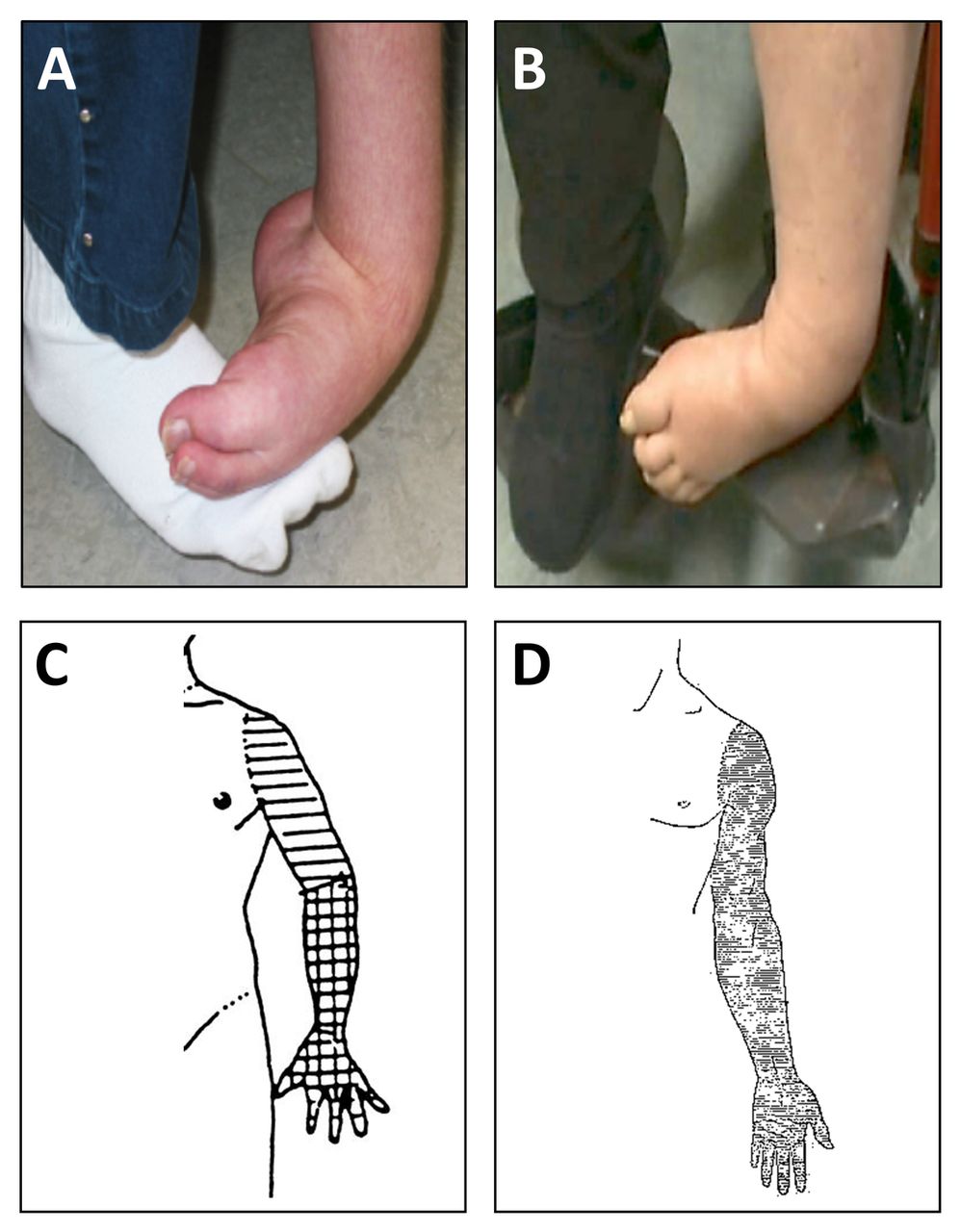
FND describes the presence of disabling and/or distressing motor and sensory symptoms which can be identified by the presence of positive evidence of internal inconsistency such as Hoover’s sign or tremor entrainment sign or other evidence of incompatibility with a structural disease process. Such positive motor and sensory signs have been consistently identified as also characterising the motor and sensory features of CRPS. For example, there is no clinical difference between the fixed dystonia characterised by a clenched fist or plantarflexed/inverted ankle seen in CRPS and that seen in FND without pain.6 Tremor,7 limb weakness8 and sensory disturbance9 have also been identified as having the same features in CRPS as in FND (table 1, online supplementary table references e1-e32, figure 1).10–13 Importantly, the need for antecedent psychological stressors has been removed from newer diagnostic criteria in DSM-5 for FND in recognition that, like CRPS, many patients do not have identifiable stressors or psychiatric comorbidity.14 15 This is important, since the absence of pre-existing or comorbid psychiatric problems has often been falsely interpreted as evidence against functional (psychogenic) processes in CRPS. Concurrently, there is now a large literature on changes in brain function in patients with FND, including differences to feigning, which is changing previous narrow purely ‘psychogenic’ thinking about the disorder.16
Supplemental material
Clinical overlap of CRPS and FND

However, in the face of multiple indicators of central and peripheral changes in CRPS, in contrast to a dualistic, anachronistic and traditionally poorly articulated idea of functional disorders as exclusively the domain of psychological disturbance (or worse still, malingering), it is perhaps not surprising that polarisation has persisted. In much of the literature, it is easy to detect, and understand, a defensive tone in which advocates for patients with CRPS defend the integrity of their patients against those who would ‘doubt’ them or accuse them of having a stigmatised psychiatric disorder. For example, Hill and colleagues summarised that ‘there is no indication that psychological factors cause the onset of pain, autonomic dysfunction, and movement disorders in CRPS patients’,17 whereas in another review, Ronald P. Pawl concluded that ‘(t)here is no convincing evidence that a primary organic dysfunction of the nervous system, in particular the autonomic nervous system, exists in (CRPS)’.18
The dualistic nosological line of separation between CRPS and FND has been drawn with such unanimous certainty that it extends well into the newest international diagnostic criteria, that see FND as a differential diagnosis which strictly precludes CRPS.1 19 Last, this polarised view is perhaps best exemplified in the recent UK guidelines which were authored without input from either neurologists or psychiatrists: ‘a combination of elements including inflammation, dysfunction within sympathetic and somatosensory nervous system, and cortical (not psychological) factors are thought to contribute to the generation and perpetuation of symptoms’ (emphasis added).20 With a recently reinvigorated interest in functional disorders of the nervous system, neurologists have been reasserting the conceptual proximity and physiological overlap of FND and CRPS21 but these have stopped short of challenging the dualistic thinking that has dogged both disorders.
Most current authors on CRPS tend to acknowledge a limited (secondary) role of psychological factors, without considering an alternative possibility—that the conventional divide between ‘organic’ and ‘non-organic’ disorders is no longer tenable in the face of what we know about the brain and body. Discarding this division allows for a new possibility: to have a disorder of nervous system functioning which presents with physical symptoms and which can exist independently of psychiatric comorbidity but in which cognitive and behavioural factors are still relevant.
This review will re-examine the clinical overlap and common pathology of CRPS and FND and will propose that the debate moves to this more productive middle ground. Providing first a brief overview of the pathophysiology of CRPS and FND (see figure 2), we will then go on to present a unifying framework for understanding these disorders and will review the implications for treatment. In doing so, we believe that patients, clinicians and researchers in both CRPS and FND could benefit.

{kind=link}
{kind=link}
An illustration of the pathophysiological overlap between CRPS and FND. *‘Paralysis’ stands in for any form of movement disorder typical of CRPS such as dystonia, tremor or weakness. CRPS, complex regional pain syndrome; FND, functional neurological disorder.
The overlaps between CRPS and sensorimotor FND
CRPS is a chronic pain disorder with a combination of sensory, motor, autonomic and dystrophic changes. These changes are usually triggered by an incipient event such as injury or surgery, but can occur spontaneously in a minority of cases.22 Although traditionally FNDs have been associated with psychological trauma, systematic studies have revealed that they very often arise from physical injury. In a systematic review of 869 cases, 37% of functional motor and sensory disorders had a history of physical injury, and in surgical settings, similar to CRPS, 79% of sensorimotor FND are preceded by a physical precipitant.23 In a prospective cohort of 50 patients with functional movement disorders (dystonia in 36%), as many as 80% reported a precipitating ‘physical’ noxious event within the preceding 3 months, with 38% fulfilling the criteria for panic attack in association with said event.24 The combination of immobilisation (reflexive due to acute pain or iatrogenic through plaster cast bandaging) and excessive anxiety is considered a potential precipitant for FND development. Stressful life events precede FND only in about a half of cases,14 and their importance has been downgraded from a diagnostic criterion to an optional risk factor in the revision of DSM-5.
Central to our argument is the nature of motor and sensory signs seen in both CRPS and FND (box 1, figure 1). In contrast to classic (idiopathic/primary) dystonia, functional dystonia is usually immobile (‘fixed’); develops acutely, often following minor injury; cannot be alleviated by sensory tricks (so-called geste antagoniste) but is instead intensified by any manipulation; is accompanied by other functional motor and sensory symptoms and is usually associated with regional pain.25 Even in functional paralysis without dystonic posturing, pain in the affected limb is reported in a third of cases.26 In their large series of ‘fixed dystonia’, Schrag and colleagues reported a 20% overlap of CRPS.6 Meanwhile, Mailis-Gagnon and colleagues found that among 54 presumed CRPS cases, experts determined 18% to be suffering from ‘psychogenic’ disorders.27 Limb weakness and bradykinesia are almost universally present in CRPS, with most having ‘give-way’ weakness8 28 and around 70% of patients develop movement disorders such as dystonic posturing, tremor and/or myoclonic jerks.7 28 Patients show reduced voluntary control and have problems initiating movement28 or assessing limb position.29 Sensory symptoms are often in a non-dermatomal distribution.12 Other positive diagnostic features used in the diagnosis of FND, such as distractibility, suggestibility, clinical inconsistency and physiological incongruity, can be found in patients with CRPS.
How can the clinical overlap between FND and CRPS be understood in terms of pathophysiology? The early alterations seen in CRPS are dominated by peripheral inflammatory changes and autonomic response.19 Local nerve injury is thought to underlie early neuropathic pain and can trigger neurogenic tissue inflammation mediated by neuropeptides such as substance P and calcitonin gene-related peptide.30 Driven also by proinflammatory cytokines such as TNF-a, IL-1b, IL-2 and IL-6, this inflammatory state is thought to underlie hyperalgesia, early allodynia and autonomic and dystrophic changes.31 Autonomic changes can include so-called sympatho-afferent coupling, whereby nociceptive fibres are thought to be activated by sympathetic nervous system activity.2 The neuroimmunological interplay is further complicated by the potential contributions of neural autoantibodies32 and small non-coding RNA molecules called microRNA.33 Importantly, such proinflammatory, autonomic and hyperalgesic regional tissue reactions can be observed reliably in (experimental models of) acute injury, transient immobilisation and chronic pain in general.34
So what keeps these proinflammatory processes in CRPS from abating normally over time, as they usually would after injury and temporary immobilisation? In CRPS, we hypothesise that the peripheral inflammation becomes interlocked with much wider-reaching nervous system maladaptations that are identical to those seen in FND (figure 2).
A temporary adaptation of movement to acute pain (or to the expectation of pain) is a physiological reaction and involves a redistribution of muscle activity that leads to stiffening, restriction and slowing of movement and favours relieving postures.35 Such adaptations, while normally only transient and largely under volitional control, can become entrenched in robust pathways through cycles of negative reinforcement until they are no longer within the reach of conscious control. Hypervigilance and avoidance based on anxious illness beliefs, catastrophising tendencies or excessive self-monitoring can imprint expectations of pain and immobility that can distort and even override incoming sensory information.36 Such failure to readapt has been proposed to underlying chronic dysfunction in FND and can just as well explain sensory and motor symptoms in chronic CRPS.
Studies of central nervous function using functional MRI and transcranial magnetic stimulation in both disorders have revealed subtle but comparable abnormalities of brain activations (see Aybek and Vuilleumier16 and Di Pietro et al 37 ,38 for review). Most studies examining central function in CRPS and FND are too heterogeneous to allow direct comparisons, but there is one group that has tested motor execution and imagery using the same paradigm in both CRPS39 and functional limb weakness (‘conversion paralysis’).40 Compared with healthy controls, patients with CRPS showed hypoactivation of the postcentral gyrus and inferior parietal cortex contralaterally during imagined movement of the affected hand.39 Similarly, patients with functional limb weakness (‘conversion paralysis’) showed decreased activity of the contralateral supramarginal cortex (part of the inferior parietal cortex) compared with controls on imagined movement in the affected hand.40 In van Velzen’s study of patients with CRPS,37 healthy controls and immobilised patients showed normal corticospinal activity during motor imagery and motor observation. The authors postulated that motor symptoms of weakness, slowness and dystonia in CRPS are due to abnormal afferent (peripheral) information processing and therefore treatment should be focused on normalising this by touch and use of the affected limb.41 However, other neurophysiological investigation of peripheral mechanisms of CRPS and motor FND have demonstrated inhibition of sensorimotor integration and reduced corticospinal activity in motor imagery but not motor observation, suggesting a central mechanism of movement inhibition. In all likelihood, both peripheral and central mechanisms are involved at different stages.
Neuroimaging of pain states has shown activation in motor areas of the brain.42 Central pain hypersensitisation has been demonstrated in experimental immobilisation43 and is reflected in the non-dermatomal distribution of sensory symptoms in CRPS.21 While sensory symptoms in motor FNDs have received woefully little attention in research so far, clinical experience shows that if inquired about, they will be reported by the majority of patients with functional weakness26 and other functional movement disorder. Interestingly, even characteristic autonomic changes such as regional limb temperature changes can be induced experimentally using protocols for disrupted sense of limb ownership (rubber hand illusion), emphasising the influence of top-down processes.44
Given the well-documented overlap in clinical presentation and the common pathophysiological pathways described above, why is CRPS considered so distinct from FND, or vice versa, and why have FND researchers devoted so little attention to sensory symptoms and inflammatory processes? The reason, we would argue, is in the historical framing and reframing of these disorders addressed in the introduction. Pain specialists, decidedly impressed by the evidence of tissue changes that immunologists and molecular biologists have provided, have come to see top-down cognitive and behavioural processes as secondary effects of CRPS pathology. Of course, phobic avoidance and anxiety are being recognised and treated, but they are not seen as driving factors of the disorder per se. Similarly, neurologists, often concerned with the differentiation of organic versus ‘non-organic’, tend to see FND, once identified, as a strictly psychogenic disorder. Sensory alterations and trophic changes are discarded as by-products of a unidirectional top-down disorder and receive little attention both clinically and in research. Thus, CRPS and FND seem to occupy opposing lanes of the highway, with all the same landmarks clearly visible, but, alas, never the twain shall meet.
However, this is not how organic systems work, especially recursive neuronal networks and their neurohumoural and neuroimmunological continuations. Bidirectional hierarchical models based on Bayesian inference have recently been formulated for both FND36 and CRPS.45 They necessitate a rethinking for both disorders in which outdated ideas of ‘psychogenic versus neurogenic’ have to be shaken off permanently. ‘Top-down processes’ do not refer to mysterious forms of subconscious symptom conversion. Rather, the expectation of pain will influence movement (kinesiophobia, avoidant disuse) and also pain perception itself, as any nocebo researcher will confirm.46 Furthermore, these reiterative cognitive-behavioural patterns of pain expectation and pain perception, kinesiophobia and disuse, will imprint themselves into the neural systems that underlie nociception and movement through synaptic and cortical plasticity, giving rise to central allodynia and functional limb weakness. Crucially, normalisation cannot often be forced purely bottom-up through analgesic drugs, but has to be achieved through some form of modulation of top-down influence.
Treatment
Understanding CRPS and FND in this way has potential benefits for treatment of both disorders. In FND, there have been recent promising randomised controlled trials of physiotherapy that emphasise the importance of establishing the potential for reversibility in FND, often through scrutiny of the motor signs themselves. Conversely, FND researchers have much to learn from mechanistic and treatment studies in CRPS.
In recent years, there has been an evolution in how clinicians approach the explanation of FND. Previously, patients may have been told they had a psychological problem and needed referral to a psychiatrist. Now many clinicians have advocated an emphasis on understanding the mechanism of the motor symptom itself and considering psychological comorbidities separately. Of central importance to this approach, and to the new DSM-5 diagnosis of FND, is to demonstrate to the patient the positive clinical signs, such as Hoover’s sign of functional leg weakness or tremor entrainment sign. The positive signs of FND emphasise profoundly therapeutic feature of the diagnosis: that the symptoms are due to a functional rather than structural problem, arise from the brain (and not the limb) and have the potential for reversibility. This ‘software rather than hardware’ framework for the patient to understand how and why the disorder has occurred, with a focus on correcting abnormal self-directed attention and movement expectation, appears in many cases to be key to successful treatment.
Two randomised controlled trials of physiotherapy have shown the potential success of this approach in FND.47 48 A recent randomised controlled trial (RCT) of 60 patients randomised either to specific FND therapy or a similar number of community physiotherapy sessions showed significant improvement in functional independence and mobility scores in the treatment vs control arms (72% vs 18%) even in patients with long duration of symptoms (5.8 years).47 Patients in the control arm only improved in 18% of cases and on 6-month follow-up, 32% had developed worsening symptoms (3% in the treatment arm). Another Randomised Controlled Trial (RCT), also of 60 patients with functional gait disorder, demonstrated the normalisation of gait in most patients despite a 9-month duration of symptoms.48 More than half of the patients in Nielsen et al’s 2016 study had pain or fatigue described as severe or extreme.47 Part of the treatment was education that the mechanisms for FND are similar to those for chronic pain, are not correlated with worsening structural damage and are potentially reversible by retraining.
An updated Cochrane review of physiotherapy for patients with CRPS found some evidence of improvement in pain and functional disability with graded motor therapy and improvement in impairment 1 year after multimodal physiotherapy; however, evidence for both was classed as very low quality.49 Perceived harmfulness of activities and pain-related fear predicts functional limitations in CRPS50 and patients with CRPS have increased phobic anxiety compared with patients with other types of chronic pain.51 Based on these principles, an RCT (n=46) of exposure vs pain-contingent treatments has demonstrating significant benefit in disability, reduced pain catastrophisation, pain intensity and increased physical and mental health-related quality of life at 6 months follow-up.52 Treatment for patients with chronic CRPS (average 5.1 years) involved reducing pain-related fear using exposure treatment with a similar paradigm as used in the treatment of anxiety disorders. Another treatment series of 106 patients with ‘end stage CRPS’ who had failed other CRPS treatments, described outpatient physiotherapy focused on achieving movement after an extensive explanation of CRPS as a ‘reversible deregulation of the nervous system’ and pain as a ‘false warning sign’ rather than something suggesting ongoing tissue injury.53 In these 106 patients, function improved in 95 patients and a full functional recovery occurred in 49 (46%) despite medications being stopped and some increase in pain during treatment. There is a clear overlap between these treatment approaches for CRPS and FND which mirrors the overlap in the disorders themselves.
Psychological therapy is a first-line therapy for patients with dissociative seizures and has some evidence for FND in general.54 Psychologists and psychiatrists play an important role in successful multidisciplinary for patients with FND.55 From our experience, the best outcomes in patients with motor FNDs occur when patients have treatment which challenges their top-down expectations, kinesiophobia and behavioural habits such as avoidance as well as physical therapy improving peripheral input. The technique of formulation of the mechanism of motor FND, taken from cognitive behavioural therapy, along with self-reflection and a personalised physical and mental management plan for dealing with exacerbations may be the key differences between successful and unsuccessful physical therapy in FND.47
In summary, a case series and randomised controlled trials based on communicating an understanding of both FND and CRPS as due to an abnormal, potentially reversible, malfunctioning nervous system, followed by physiotherapy focused on regaining function even if pain is transiently increased, have demonstrated positive outcomes. This suggests that patients’ understanding is key and demonstrates that improvement is possible even in those patients who have had CRPS or FND for many years. In our view, education-based physiotherapy which targets both top-down processes and expectations as well as bottom-up sensorimotor inputs with or without peripherally acting medication adjuncts should be the mainstay of treatment for both disorders.
Conclusion
Discussions involving CRPS and functional disorders have been adversarial in the past. We have a new understanding of what functional disorders are: centrally mediated processes of abnormal self-directed attention, often triggered by peripheral stimuli, with complex neural, emotional and social risk factors and perpetuation. Combining this with a removal of the suspicion of feigned symptoms from the conversation of what CRPS and FNDs are leads us to a new path of learning from each disorder. There is significant overlap between both CRPS and FND in new mechanistic understanding, motor symptoms, imaging and neurophysiology studies. In both CRPS and FND, explanation-based physical treatment, which encompasses understanding of the disorders as reversible, seems most positive. There is much for FND researchers to learn from the work already done into peripheral and central mechanism of CRPS with a greater focus on investigating ‘bottom-up’ input into the mechanistic model of functional disorders. Similarly, recognising shared social, emotional and cognitive risk factors and bidirectional input as mechanisms in CRPS symptom production could allow for more encompassing and optimistic explanation and treatment strategies. We hope that presenting the similarities and learning from both disorders will encourage researchers in CRPS and FND to see that historical antagonism should now be put to one side, in favour of reconciliation and collaboration on how to understand and treat these complex and important disorders.
References
Footnotes
SP and IH contributed equally.
Contributors SP and IH contributed equally to writing the first draft of the manuscript and conducting the literature search. LC, AJC and JS were involved in literature selection, editing and writing of the manuscript. All authors approved the final version of the manuscript.
Funding SP was supported by a scholarship from the FoRUM Forschungsreferat (research office) of the Medical Faculty of the Ruhr-University Bochum, Germany. IH is supported by an Association of British Neurologists/Patrick Berthoud Charitable Trust Clinical Research Training Fellowship. JS is supported by an NHS Scotland NRS Career Fellowship.
Competing interests SP and IH declare no conflicts of interest. LC has received honoraria for speaking at educational meetings to healthcare professionals on a range of chronic pain topics (Pfizer (October 2015); is an editor on the British Journal of Anaesthesia (receives an honorarium plus a contribution towards related departmental expenses (October 2010–to date)) and chairs the Scottish Pain Research Community (SPaRC/ NHS Research Scotland Pain Research Network, which has received non-promotional funding from Pfizer, Grunenthal and QDem to support the Annual Scientific Meeting. AJC reports giving independent testimony in court on a range of topics that include functional neurologic symptoms; being a paid editor at the Journal of Neurology, Neurosurgery, and Psychiatry and receiving lecture fees from a range of firms on general neuropsychiatric topics (total income in last decade less than £1500). JS reports giving independent testimony in court on a range of topics that include functional neurological symptoms and CRPS and having received royalties from UpToDate for articles on functional neurological disorder and runs a free non-profit self-help website, www.neurosymptoms.org, which discusses these issues.
Patient consent Not required.
Provenance and peer review Commissioned; externally peer reviewed.