Article Text

Abstract
Background The syndrome of Headache and focal Neurological Deficits with cerebrospinal fluid Lymphocytosis (HaNDL) is considered a rare, idiopathic and self-limited condition.
Methods We present a patient with HaNDL who had unique findings of florid optic disc haemorrhages from bilateral central retinal vein occlusions.
Results Our patient made a full recovery with conservative management.
Conclusion It is important for medical attendants to recognise that HaNDL syndrome can be associated with neuro-ophthalmic complications.
- neuroophthalmology
- headache
- vision
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Case report
A 35-year-old Caucasian female presented with headaches and focal neurological symptoms, on a background of migraines with visual aura. Past medical history included depression and a motor vehicle accident aged 17. She had a normal body mass index, no history of recent overseas travel or hypertension.
While at work, 1 month prior to review, she developed fogginess in her head followed by a severe headache and blotchy white spots in her vision. Her symptoms resolved spontaneously during the course of the day. The following day she became unwell again, with subjective cognitive difficulties, low-frequency tinnitus bilaterally and further episodes of paraesthesia, which spread up the right arm into the face and sometimes involved her right leg. She continued to experience severe frontotemporal headaches. She also reported cognitive difficulties and had a CT brain, which was normal.
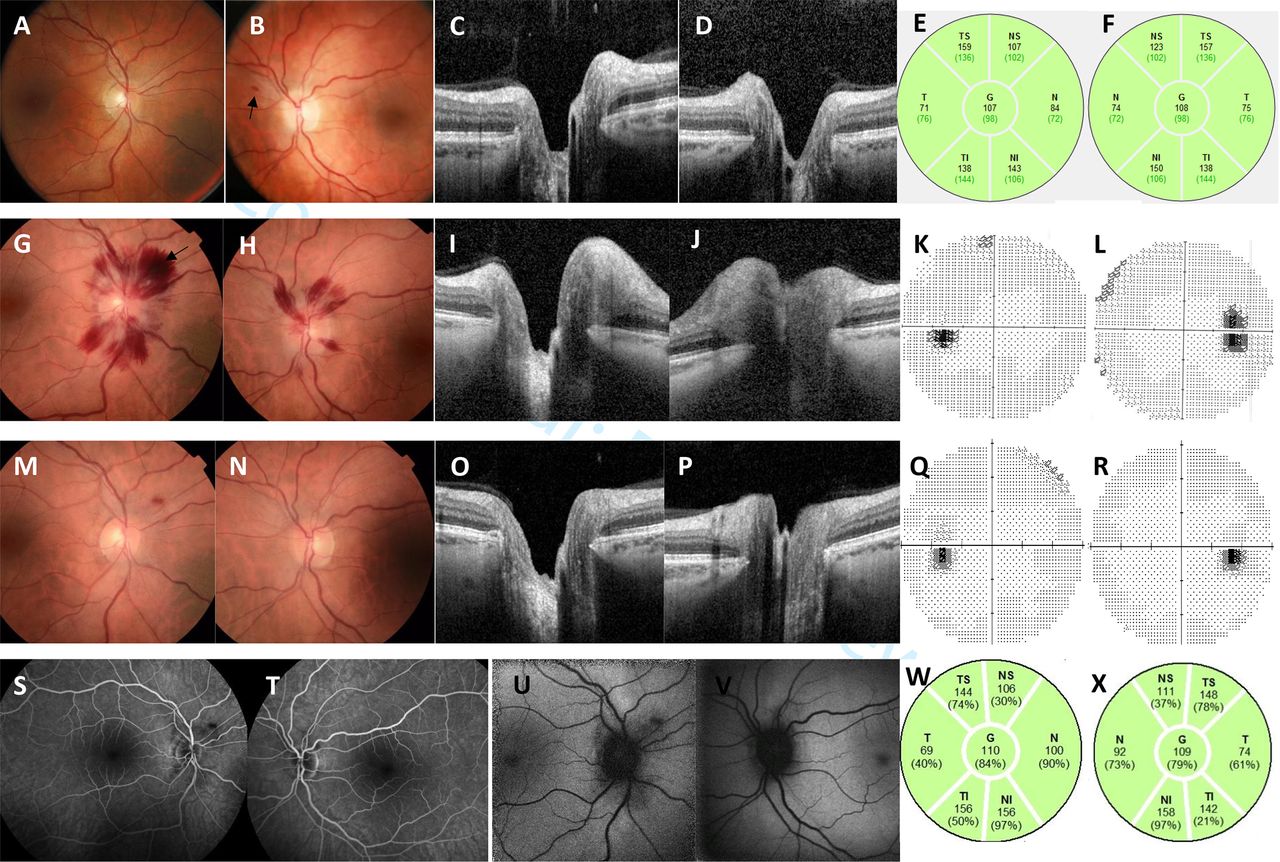
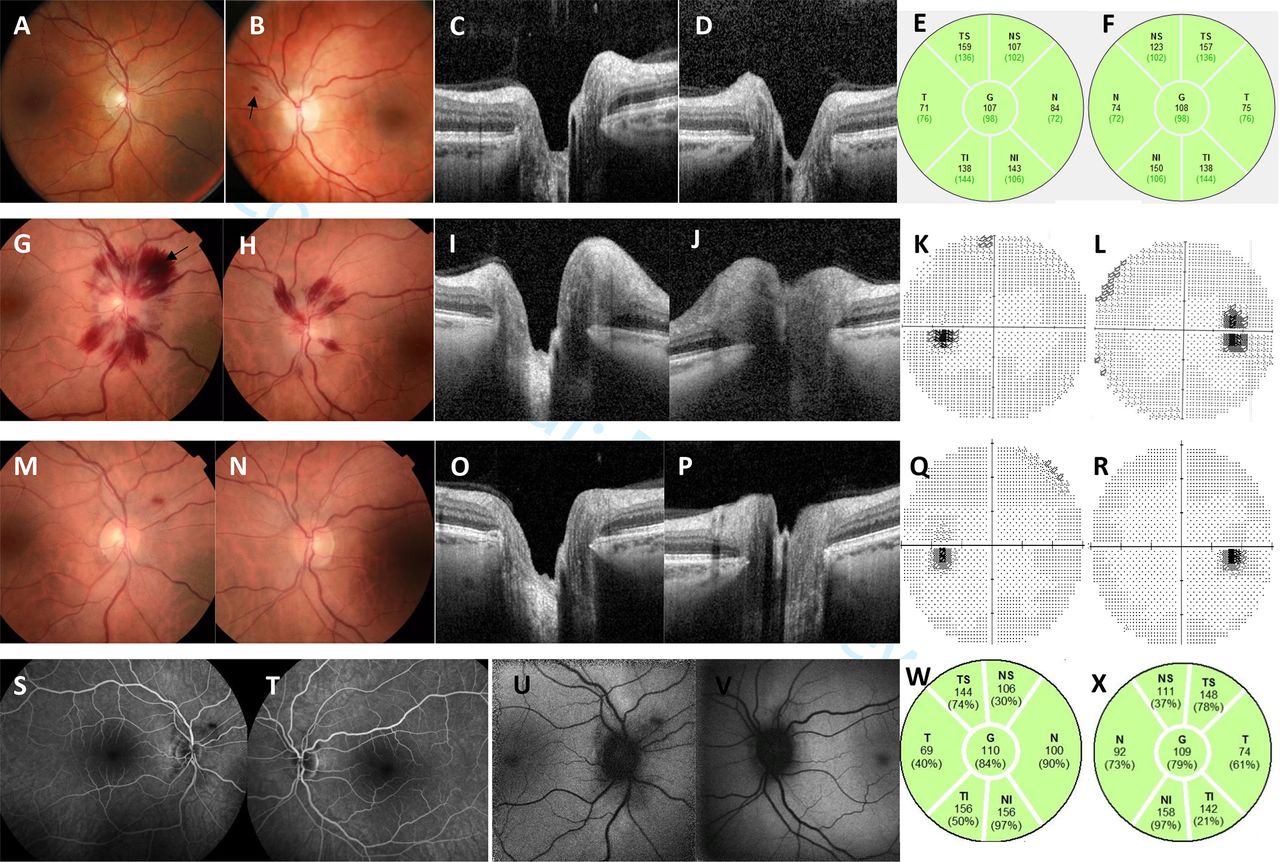
Lumbar puncture demonstrated mildly elevated opening pressure of 28 cm of water, 98 lymphocytes and an elevated protein of 0.83. Cerebrospinal fluid (CSF) glucose was normal and there were no polymorphs. Fundus photography showed a single, small flame haemorrhage nasal to the left optic disc (figure 1B) and optical coherence tomographic (OCT) scanning showed very subtle disc oedema (figure 1C,D). She was presumed to have a possible viral meningitis and elected to self-discharge against medical advice due to a desire to rest at home. The CSF viral panel, gram stain and culture were subsequently negative. She was treated with low-dose amitriptyline for headaches.
{kind=link}
A 35-year-old Caucasian female with HaNDL (Headache, Neurological Deficits and cerebrospinal fluid Lymphocytosis). At presentation 01 November 2018 colour fundus photographs of the right (A) and left (B) eyes show clinically normal discs and a single retinal nerve fibre layer haemorrhage in the left eye (arrow). Optical coherence tomographic (OCT) scanning of the right (C) and left (D) optic nerves shows subtle oedema, with OCT scanning of the retinal nerve fibre layer of the right (E) and left (F) eyes within normal limits. Three weeks later (23 November 2018) colour fundus photographs of the right (G) and left (H) eyes show optic disc margins are slightly blurred, central retinal veins are dilated and disc and retinal nerve fibre haemorrhages have developed in both eyes, with a deeper intraretinal haemorrhage (arrow) in the right eye. OCT scanning confirms more prominent disc oedema in the right (I) and left (J) eyes. Automated visual field testing is normal in the left eye (K) and shows an increased blind spot in the right eye (L). On review 2 months later colour fundus photography (M right eye, N left eye) shows residual intraretinal haemorrhage in the right eye, but is otherwise normal. OCT scanning shows resolution of oedema in the right eye (O) and a small amount of residual oedema in the left eye (P). Visual fields (Q left eye, R right eye) are normal. Fluorescein angiography demonstrates the right retinal haemorrhage (S) and is normal in the left eye (T). Fundus autofluorescence demonstrates increased hypoautofluorescence around the right optic disc (U) and to a lesser extent the left optic disc (V). OCT scanning of the retinal nerve fibre layer (W right eye, X left eye) is within normal limits.
Approximately 3 weeks later she redeveloped headaches and brief episodes of visual blurring. Visual acuity was 6/6 bilaterally with normal intraocular pressures. Funduscopy revealed slightly blurred optic disc margins, extensive disc and retinal nerve fibre layer haemorrhages, dilated retinal veins with elevated venous closing pressures and normal arterial closing pressures. The remainder of the neurological examination was normal. Blood pressure was 123/95. Automated visual field testing revealed an enlarged blind spot on the right (figure 1L) and OCT showed an increase in bilateral optic disc oedema (figure 1I,J).
She was admitted for further investigations to exclude raised intracranial pressure and other causes of meningitis although, on review, the fundus findings were felt to be more consistent with bilateral central retinal vein occlusions (CRVO). MRI brain and venography were normal. Full blood count, urea, electrolytes, creatinine, C-reactive protein, lactate, liver function tests, calcium, magnesium, phosphate, clotting studies and thyroid function tests were normal. Legionella, HIV, hepatitis, syphilis serology and autoimmune testing were negative. Mycoplasma and cytomegalovirus serology showed evidence of past infection. CSF opening pressure was 15 cm of water and CSF analysis showed normal protein and glucose; lymphocytes were elevated at 17 without accompanying granulocytes or erythrocytes. Cryptococcal antigen, gram stain, oligoclonal bands and viral panel (Epstein-Barr virus, herpes simplex virus, varicella zoster virus, enterovirus) were negative. She was treated with analgesia; the retinal vein occlusions did not require treatment. Her symptoms settled quickly over 2 days and she was discharged from hospital.
On review 1 month after discharge, she was feeling much better. She denied headaches or focal neurological symptoms and had returned to work in the past 3 weeks. Follow-up assessment demonstrated improvement in both funduscopic appearances and optic disc swelling on OCT (figure 1M–P). As she experienced episodes of migraine-like headaches associated with transient neurological deficits, which correlated with CSF lymphocytosis, without a better ICHD-3 (International Classification of Headache, version 3) diagnosis to account for her symptoms, she met the ICHD-3 diagnostic criteria for HaNDL (thesyndrome of Headache and focal Neurological Deficits with cerebrospinal fluidLymphocytosis).
Discussion
The aetiology of HaNDL remains unknown, although pathogenesis may relate to autoimmune, migrainous or post-viral conditions.1 Approximately 25% to 40% of patients experience a viral infection preceding their development of HaNDL syndrome,2 3 and possible associations with other infections should be sought, including human herpesvirus (HHV). Case reports have described separate patients who met diagnostic criteria for HaNDL, who were subsequently found to have serological evidence of recent infection with HHV-6 and HHV-7.4 5 In addition, separate paediatric patients with HHV-6 and varicella zoster virus (VZV) infections developed unilateral central retinal vein occlusion.6 7 HHV and VZV are not currently on the list of infections to be excluded for a diagnosis of HaNDL.8
Patients diagnosed with HaNDL are usually around 30 years old,9 but cases involving children have been described.10 Most patients have no history of migraine, although headaches in cases of HaNDL frequently involve migrainous features.8 HaNDL is characterised by the presence of CSF pleocytosis associated with a typically rapid onset headache and neurological deficits, most commonly dysphasia, hemiparaesthesia and hemiparesis.2 The heterogenous clinical presentations of HaNDL syndrome can mimic neurological conditions such as stroke, transient ischaemic attack, migraine and encephalitis.11–15 The diagnostic criteria of HaNDL as outlined by the International Headache Society are based on typical clinical features, association between CSF pleocytosis and headache, as well as the exclusion of secondary causes.8
CSF examination reveals lymphocytosis in the range of 10 to 760 cell/mm3, protein elevation up to 250 mg/dL in 91% to 96% of cases and an elevated opening pressure in 56% to 73% of measured cases.2 3 Imaging findings from different modalities have been reported. Non-specific T2 hyperintensities, CSF enhancement, reduced perfusion16 and reduced venous signal can be seen on brain MRI.17 Brain CT perfusion imaging performed during attacks typically show evidence of hypoperfusion.18 Single photon emission computed tomography may show reduced activity of affected brain regions and bilateral arterial vasospasm has been observed on transcranial doppler ultrasound. Electroencephalography studies performed during attacks can display focal or diffuse slowing.19
Currently the mainstay of management in HaNDL is supportive, as patients usually improve with time and without long-standing sequelae. Acetazolamide and other pressure-lowering therapies have been given to patients with high intracranial pressure, to try and reduce the risk of complications. There is limited evidence for other treatments, such as steroids or serial lumbar punctures. Despite our patient’s dramatic funduscopy appearances, her vision was minimally affected and she recovered fully without treatment.
The differential diagnosis for our patient’s optic disc appearances and retinal haemorrhages included CRVO and papilloedema secondary to raised intracranial pressure. Her funduscopic appearances were most suggestive of CRVO. There were dilated retinal veins and the venous closing pressure was elevated, while the arterial closing pressure and appearances were normal. If considering the possibility of papilloedema, the minor degree of optic disc margin blurring and normal CSF opening pressure at the time of repeat examination were inconsistent with the florid retinal haemorrhages.
The diagnosis of HaNDL should be considered in patients with headaches and transient neurological symptoms if there is no other apparent cause. We present a case of HaNDL syndrome with bilateral CRVO, which has not been described before in association with this condition. The course of HaNDL is usually benign, however medical attendants should be aware of potential ocular complications and the need to consider treatment in rare cases.
References
Footnotes
Contributors WW performed a literature review, wrote the draft manuscript and revised the paper as required. HM sourced the images/figures and wrote the figure legend. JW was the primary physician involved in the patient’s care and provided clinical information. OW, RS, HM and JW made suggestions and revisions to the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. Not applicable.