Article Text

Abstract
Objectives Neuromyelitis optica is a devastating, relapsing, inflammatory, autoimmune disorder characterised in large part by attacks of optic neuritis and transverse myelitis causing blindness and plegia in many patients. Eighty-three per cent of patients with transverse myelitic attacks and 67% of patients with optic neuritis attacks have no or a partial recovery.
Methods Results from The European Group for Blood and Marrow Transplantation Autoimmune Diseases Working Party imply failure of autologous haematopoietic stem cell bone marrow transplantation.
Results and conclusion We present a case that despite eventual relapse, made a remarkable functional recovery after bone marrow transplantation which may justify bone marrow transplantation in severe cases.
- neuroimmunology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Neuromyelitis optica (NMO) is a devastating, relapsing, inflammatory, autoimmune disorder1 characterised in large part by attacks of optic neuritis (ON) and transverse myelitis (TM) causing blindness and plegia in many patients.2 Attacks are unpredictable and tend to be severe (a ‘neuro-immunological stroke’).3 Eighty-three per cent of patients with TM attacks and 67% of patients with ON attacks have no or a partial recovery.4 The initial presentation is 50% with TM, 35% with ON, ON with TM in 10% patients and 4% of patients with other syndromes.2 Up until recently, there was no proven agent to treat to prevent relapses. We now have three agent examined in phase 3 clinical trials for the treatment of NMO (eculizumab), an anti-C5 complement inhibitor,5 satralizumab (anti-IL-6R mAb)6 and inebilizumab (anti-CD19 mAb).7
The European Group for Blood and Marrow Transplantation Autoimmune Diseases Working Party reported after a median follow-up of 47 months with baseline Expanded Disability Status Score=6.5, 3 of 16 cases were progression and treatment free, while in the remaining 13 patients further treatments were administered for disability progression or relapse after autologous stem cell transplant. Altogether, relapse-free survival at 3 and 5 years was 31% and 10%, respectively, while progression-free survival remained 48% at 3 and 5 years.8 Whereas these results imply failure of autologous hematopoietic stem cell bone marrow transplant (AHSCBMT) with NMO, we present a case that despite eventual relapse, made a remarkable functional recovery after AHSCBMT, which may justify such treatment in severe cases.
Case review
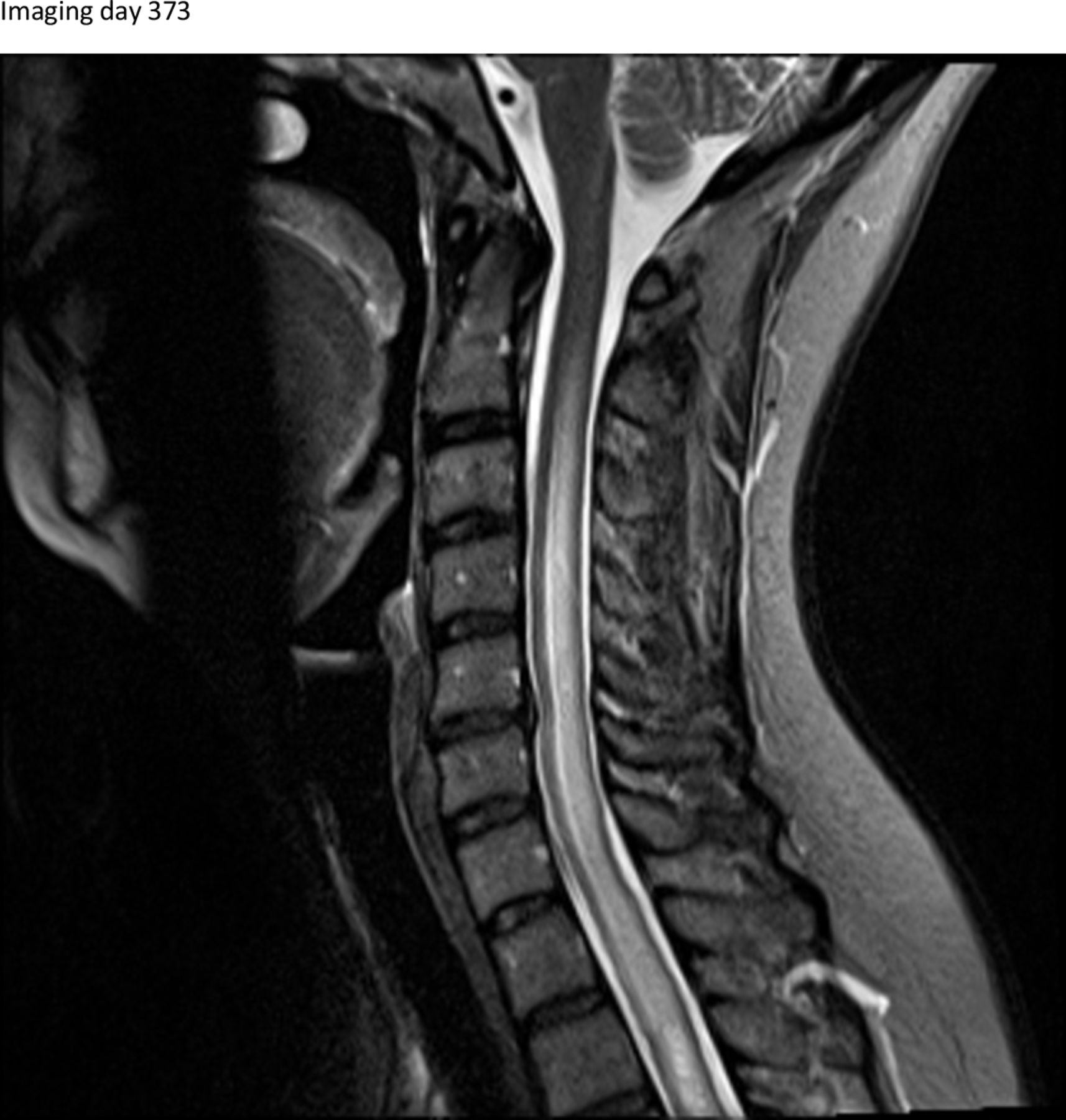
A 40-year-old women with history of irritable bowel syndrome, depression and anxiety presented to urgent care with report of bilateral foot paresthesia. She reported having a ‘rough year’ and she thought the symptoms could be due to her anxiety; she was discharged home. Ten months later (day 275) she presented with rib and back pain for 2 weeks and leg pain for 2 months. Her symptoms persisted an additional 2 months and she was referred to a spine care neurologist. At her initial evaluation (day 373) she reported mid thoracic pain, hyperesthesia in lower extremities and a buzzing sensation. MRI demonstrated a longitudinally extensive cord lesion extending from C2 to T12, concerning for a demyelinating process (figure 1 - cervical region). There was no evidence of optic neuropathy. She was treated with high dose intravenous steroids for 3 days and discharged home. Cell based NMO aquaporin-4 (AQP4) titre >1:100000.

T2 MRI demonstrated a longitudinally extensive cord lesion extending from C2 to the upper thoracic region on day 373 after initial symptoms.
Insurance denied rituximab (RTX) treatment initially and shortly after the patient returned to the emergency department (ED) with new right lower extremity weakness (day 411). She was admitted for five treatments of plasmapheresis and RTX 1000 mg infusion. Following treatment, she discharged to inpatient rehab and then home (day 432). Three days later, she returned to the ED again unable to walk, with lower extremity strength of 1/5. She was treated with an additional intravenous RTX 1000 mg infusion, Acthar Gel 80 IU subcutaneous times 5 days, and then Cytoxan 750 mg/m2 (day 442). She then continued intravenous Cytoxan treatment every 3 weeks.
The patient did not improve clinically; she was paraplegic and incontinent of bowel and bladder. She received five additional days of intravenous steroids and AHSCBMT was pursued. She received cyclophosphamide and granulocyte colony stimulating factor for stem cell mobilisation and autologous peripheral blood stem cells were collected for 3 days (day 645 to 647). Imaging showed marked cord swelling in the thoracic region (figure 2 - day 622).
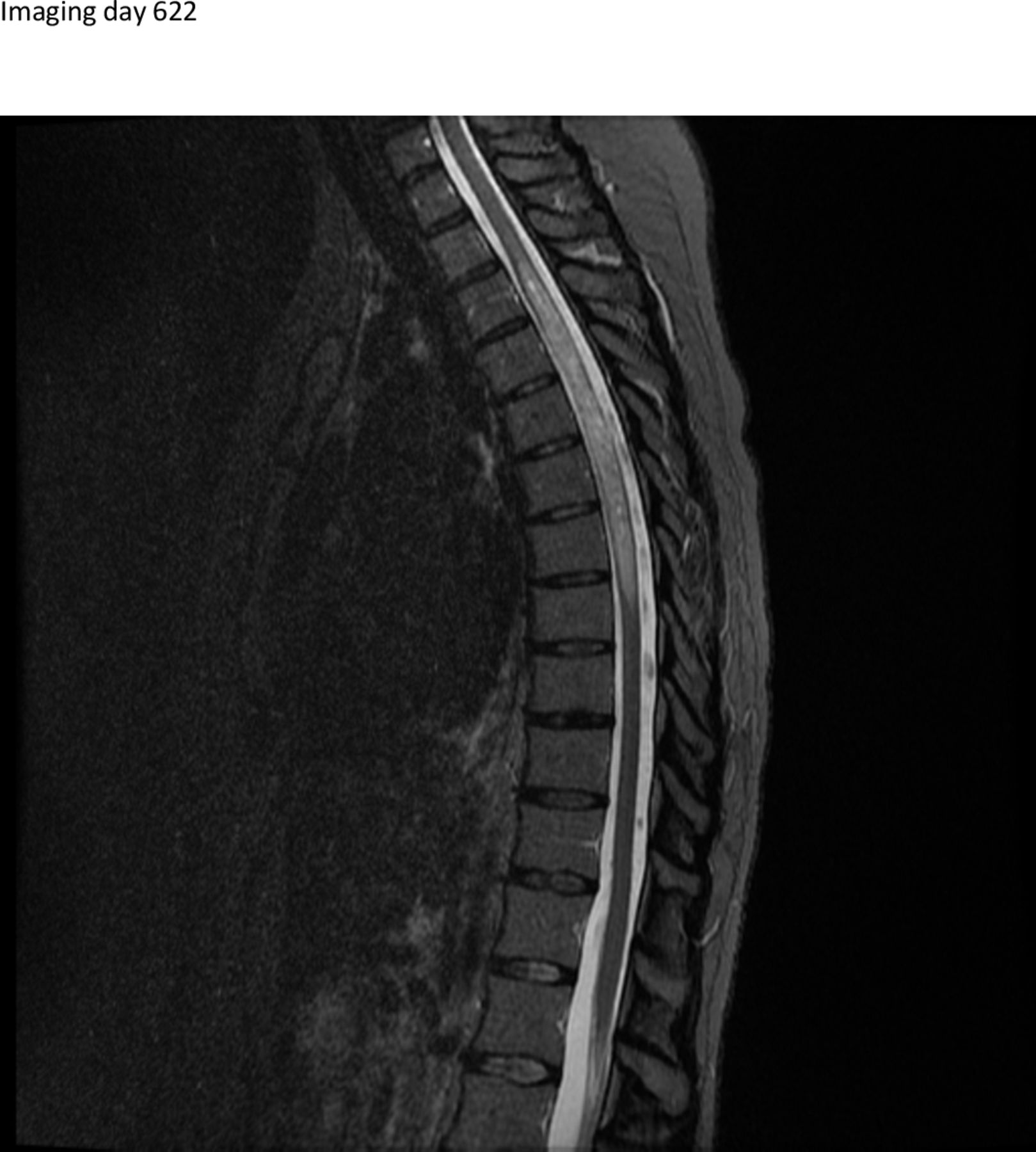
T2 MRI demonstrated marked cord swelling in the thoracic region on day 622 after relapse and just before autologous hematopoietic stem cell bone marrow transplant.
She was then admitted for AHSCBMT and received BEAM (BCNU/etoposide/cytarabine/melphalan) combined with anti-thymocyte globulin (rabbit ATG). Details of dosing are in table below. After autologous stem cell infusion she remained hospitalised for 14 additional days (day 679 to 692) until full engraftment.
At 4-month follow-up (day 819), she had made a marvellous recovery and imaging showed thoracic lesion resolution (figure 3). Clinical improvement occurs with decreased intensity in the cord imaging. She was ambulating and timed 25-foot walk (T25W) was recorded at 8.63 s. At follow-up 6 months later (day 1014), she was ambulatory, able to walk 3 miles and her T25W was 7.5 s. Cell based NMO AQP4 titre=0. The patient had recovered from an acute attack (day 622) resulting in severe disability and plegia after undergoing AHSCBMT.

{kind=link}
{kind=link}
{kind=link}
T2 MRI demonstrated showed thoracic lesion resolution at day 819, 4 months after autologous hematopoietic stem cell bone marrow transplant.
The patient returned to the ED almost 2 years after the AHSCBMT (day 1368) with new left lower extremity weakness and paresthesia. Repeat MRI of the spinal cord demonstrated a T5-6 Gd+ enhancing lesion (not shown). She was admitted and eculizumab was administered with a plan to continue every 2 weeks. At follow-up after two doses of 900 mg intravenous, 2 weeks later (day 1374), she reported she was 50% improved from her pre-relapse baseline and at most recent follow-up (day 1435) she reported she was at her baseline prior to the relapse except for endurance. The T25W had further improved to 5.6 s.
Our patient made a remarkable recovery over 4 months after AHSCBMT. The patient did have a mild relapse at 2-year post-transplant but was effectively treated back to her baseline. Despite the possibility of eventual relapse, our case shows that AHSCBMT can be effective treatment in reversing recent severe disability in neuromyelitis optica - disease modifying treatments (NMOSD). The estimated cost of AHSCBMT was less than US$4700 per quality-adjusted life year9 in multiple sclerosis. Complete reversal of plegia and employment would justify this expenditure. In terms of clinical safety, AHSCBMT is associated with a very low mortality (<1%), time limited morbidity which resolves in a short time period in the order of 2 to 3 months and improved long-term quality of life.10 How would we include AHSCBMT as a therapeutic option in the treatment of NMOSD? AHSCBMT could be used as salvage therapy for severe breakthrough disease after sequencing of NMO-DMTs. AHSCBMT could also be used as an induction therapy for severe initial presentations providing a safe segue for the initiation of long-term immunomodulation. After bone marrow transplant, patients treated with AHSCBMT should be monitored clinically for signs of relapse with consideration of transition to long-term alternative treatment.
Regimen
Footnotes
Contributors The planning, conduct and reporting of the work was shared equally by all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.