Article Text

Abstract
Background and aims Vertigo is a common presentation to the emergency department (ED) with 5% of presentations due to posterior circulation stroke (PCS). Bedside investigations such as the head impulse test (HIT) are used to risk stratify patients, but interpretation is operator dependent. The video HIT (v-HIT) provides objective measurement of the vestibular-ocular-reflex (VOR) and may improve diagnostic accuracy in acute vestibular syndrome (AVS). We aimed to evaluate the use of v-HIT as an adjunct to clinical assessment to acutely differentiate vestibular neuritis (VN) from PCS.
Methods 133 patients with AVS were consecutively enrolled from the ED of our comprehensive stroke centre between 2018 and 2021. Patient assessment included a targeted vestibular history, HINTs examination (Head Impulse, Nystagmus and Test of Skew), v-HIT and MRI>48 hours after symptom onset. The HINTS/v-HIT findings were analysed and compared between VN, PCS and other cause AVS. Clinical course, v-HIT and MRI findings were used to determine diagnosis.
Results Final diagnosis was VN in 40%, PCS 15%, migraine 16% and other cause AVS 29%. PCS patients were older than VN patients (mean age 68.5±10.6 vs 60.1±14.2 years, p=0.14) and had more cardiovascular risk factors (3 vs 2, p=0.002). Mean VOR gain was reduced (<0.8) in ipsilateral horizontal and (<0.7) anterior canals in VN but was normal in PCS, migraine and other cause AVS. V-HIT combined with HINTs was 89% sensitive and 96% specific for a diagnosis of VN.
Conclusions
V-HIT combined with HINTs is a reliable tool to exclude PCS in the ED.
- CEREBROVASCULAR DISEASE
- NEUROOTOLOGY
- STROKE
- VERTIGO
Data availability statement
Data are available on reasonable request. Please contact corresponding author for requests for data sharing.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Posterior circulation stroke (PCS) is often misdiagnosed in the emergency department which may cause excess morbidity and mortality.
Bedside clinical examination with head impulse testing and Head Impulse, Nystagmus and Test of Skew (HINTS) is effective at improving diagnostic rates of PCS in the hands of experienced clinicians.
Video head impulse testing is able to accurately differentiate vestibular neuritis from PCS.
WHAT THIS STUDY ADDS
This study demonstrates that routine use of video head impulse testing improves on the HINTS examination in the exclusion of PCS in the acute setting.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
This study supports the use of video head impulse testing in conjunction with the HINTS assessment for more accurate exclusion of a diagnosis of PCS in the emergency department. Further research on feasibility may be warranted to support widespread, routine use of video head impulse testing in the emergency department.
Introduction
Vertigo and/or dizziness is a common presentation to the emergency department (ED) accounting for approximately 3%–4% of all presentations.1 The spectrum of potential causes is broad and may include vestibular, neurological, cardiovascular or other systemic disorders. The acute vestibular syndrome (AVS) is more narrowly defined as acute dizziness or vertigo, associated with nystagmus, nausea/vomiting and gait ataxia lasting at least 24 hours.2 The most common cause of AVS is vestibular neuritis (VN), a benign diagnosis in comparison to the less common and more serious differential of posterior circulation stroke (PCS), which accounts for approximately 3%–5% of dizziness presentations to the ED.1
PCS is commonly misdiagnosed in the ED as the signs and symptoms may be subtle3 4 and MRI can miss 20%–50% of posterior fossa infarctions within 48 hours of symptom onset.5 Several techniques have been described to improve diagnosis of AVS, most notably the bedside head impulse test (b-HIT) and the Head Impulse, Nystagmus and Test of Skew (HINTS) examnation. The HIT is a simple clinical manoeuvre performed at the bedside to test the function of the horizontal semicircular canals.6 The HINTS examination has demonstrated greater sensitivity than early MRI for diagnosis of PCS.7
While the b-HIT and HINTS examinations allow for accurate diagnosis of PCS when performed by experts, their routine use in clinical practice may not be as reliable.8 9 The development of the video HIT (v-HIT)10 has allowed accurate and quantifiable assessment of the vestibulo-ocular reflex (VOR) in all six semicircular canals. V-HIT can be performed using portable and relatively inexpensive equipment at the bedside. There is increasing evidence to support the use of v-HIT alongside expert clinical assessment for diagnosis of vestibular disorders in the ED.11 There are also ongoing clinical trials12 investigating the use of v-HIT in the acute clinical setting.
V-HIT measurement of VOR gain, refixation saccade prevalence and amplitude are reliable discriminators of VN from PCS.13 An abnormal v-HIT test defined by the presence of reduced VOR gain and catchup saccades, provides objective evidence of unilateral peripheral vestibular dysfunction. This is most commonly caused by VN. Unilateral vestibular dysfunction is rare in PCS, however, isolated infarcts in the vestibular nucleus or the anterior inferior cerebellar (AICA) and/or labyrinthine artery, may demonstrate unilateral vestibular dysfunction on both b-HIT and v-HIT testing.14 The HINTS, and ‘HINTS plus’ (HINTS+) assessment, where acute hearing loss is also considered, is designed to reduce the likelihood of falsely excluding a PCS when the b-HIT is abnormal. Skew deviation is more common with a pontine or medullary infarct than VN and infarction of the cochlear nerve from an AICA stroke is associated with acute hearing loss.
In this prospective observational study, we examined consecutive AVS patients referred by ED physicians. A b-HIT and HINTs were performed by senior neurology trainees and v-HIT by audiologists. We examined the accuracy of b-HIT vs HINTS vs v-HIT in excluding a diagnosis of PCS in patients with AVS. MRI brain was performed >48 hours after symptom onset in all patients and used as the gold standard for stroke diagnosis. Our hypothesis was that v-HIT is more accurate than b-HIT and HINTS examination performed by non-expert clinicians for diagnosis of VN in a real-world application.
Methods
We prospectively recruited consecutive patients presenting with AVS between February 2018 and September 2021 to Liverpool Hospital ED, Sydney, Australia, a comprehensive stroke centre offering 24/7 acute stroke services including advanced imaging, thrombolysis and endovascular clot retrieval. The study was designed and manuscript prepared following recommendations from the Standards for Reporting Diagnostic Accuracy statement.15
Patients presenting with symptoms of dizziness, vertigo or gait unsteadiness were initially screened by ED physicians and referred to investigators. The primary investigators (AS, AV, CB and JOT) were senior neurology trainees with 1–3 years of experience in performing the HIT but without formal neuro-otology training. Patients not meeting criteria for isolated AVS2 after initial history taking and examination by study investigators were excluded from further analysis. Patients with additional focal neurological deficits consistent with acute stroke, were managed as per our local acute stroke protocol and excluded from further analysis.
Patients underwent a full neurological examination by a primary investigator (AS, AV, CB or JOT) of the cranial nerves, upper and lower limbs, as well as vestibular assessment consisting of b-HIT, cross-cover test for skew deviation and nystagmus assessment with static and dynamic manoeuvres. Dix-Hallpike test for benign positional vertigo (BPPV) was performed if BPPV was clinically suspected and patients with confirmed BPPV were excluded from the study. Assessment of nystagmus and skew was performed using basic diagnostic equipment such as a handheld ophthalmoscope and penlight, whereas Frenzel goggles, prisms and retinal photography were not routinely used. Initial clinical examination was also summarised as either HINTS peripheral (abnormal HIT AND absence of direction changing nystagmus AND negative test of skew) or HINTS central (normal HIT OR nystagmus other than unidirectional horizontal nystagmus OR positive test of skew).
Following bedside examination, patients underwent a v-HIT (ICS Impulse USB goggles, Otometrics, Taastrup, Denmark) performed by audiologists trained in use of this device. Patients presenting outside normal business hours of 08:00–17:00 hours Monday–Friday were assessed on the first business day following admission. V-HIT studies were performed during business hours only. VOR gains and presence of catchup saccades for six semicircular canals were recorded as per the protocol described by MacDougall et al.10 The v-HIT result was classified as abnormal in the presence of unilateral reduced gains in the horizontal canal <0.8, or <0.7 in anterior and posterior canals as described by Calic et al13 and Pogson et al16 along with visually determined frequent large amplitude catchup saccades. This is consistent with normal data obtained from healthy controls at our institution. The recruitment of 30 AVS cases due to PCS was calculated to have >80% power to detect a significant difference between PCS and VN using these criteria.
All patients underwent MRI at least 48 hours after onset of symptoms (General Electric 1.5 or 3T MRI, 5 mm axial slice thickness, 0.5 mm slice spacing) with T2, Fluid attenuated inversion recovery, diffusion-weighted imaging (DWI) and apparent diffusion coefficient (ADC) sequences as a minimum requirement. Patients unable to undergo or tolerate MRI, were excluded from further analysis.
VN was diagnosed in patients presenting with acute persistent vertigo with nystagmus that obeyed Alexander’s Law (unidirectional nystagmus maximal in amplitude when gaze directed to unaffected side), abnormal b-HIT or v-HIT, a negative test of skew, no evidence of diffusion restriction on >48 hour MRI and no other diagnosis deemed more likely.
PCS was diagnosed by the presence of a hyperintense lesion on DWI with corresponding hypointensity on ADC maps within a vascular territory as assessed by a neuroradiologist blinded to the v-HIT results. Any equivocal results were reviewed by a second independent neuroradiologist.
Patients were diagnosed with migraine if they presented with a syndrome lasting up to 72 hours of acute vertigo associated with migraine type headache and a personal history of migraine without evidence of acute vestibular hypofunction or MRI changes. We did not require five or more similar episodes as suggested by the Barany Society/International Headache Society diagnostic criteria for vestibular migraine17 due to acute workup of patients and variable follow-up duration in our study.
Statistical analysis was performed using IBM SPSS Statistics for Macintosh (V.27, IBM). Descriptive statistics were reported as means±1 SD unless otherwise stated. Data were tested for normality using Shapiro-Wilks tests and means between groups were compared using one-way analysis of variance or Kruskal-Wallis tests.
Comparison of proportions was performed using Fisher’s exact test. We performed post hoc analysis for non-parametric data using Mann-Whitney U tests with Bonferroni correction if a statistically significant difference (p<0.05) between means was noted. Comparisons of sensitivity and specificity between b-HIT, v-HIT and HINTS were performed using McNemar’s test for paired samples. Agreement between v-HIT and b-HIT was assessed using Cohen’s kappa.
Results
Between February 2018 and September 2021, 279 patients were referred for assessment. One hundred and forty-six were excluded from further analysis with a history inconsistent with isolated AVS, another cause for presentation readily apparent or an inability to undergo MRI (figure 1).
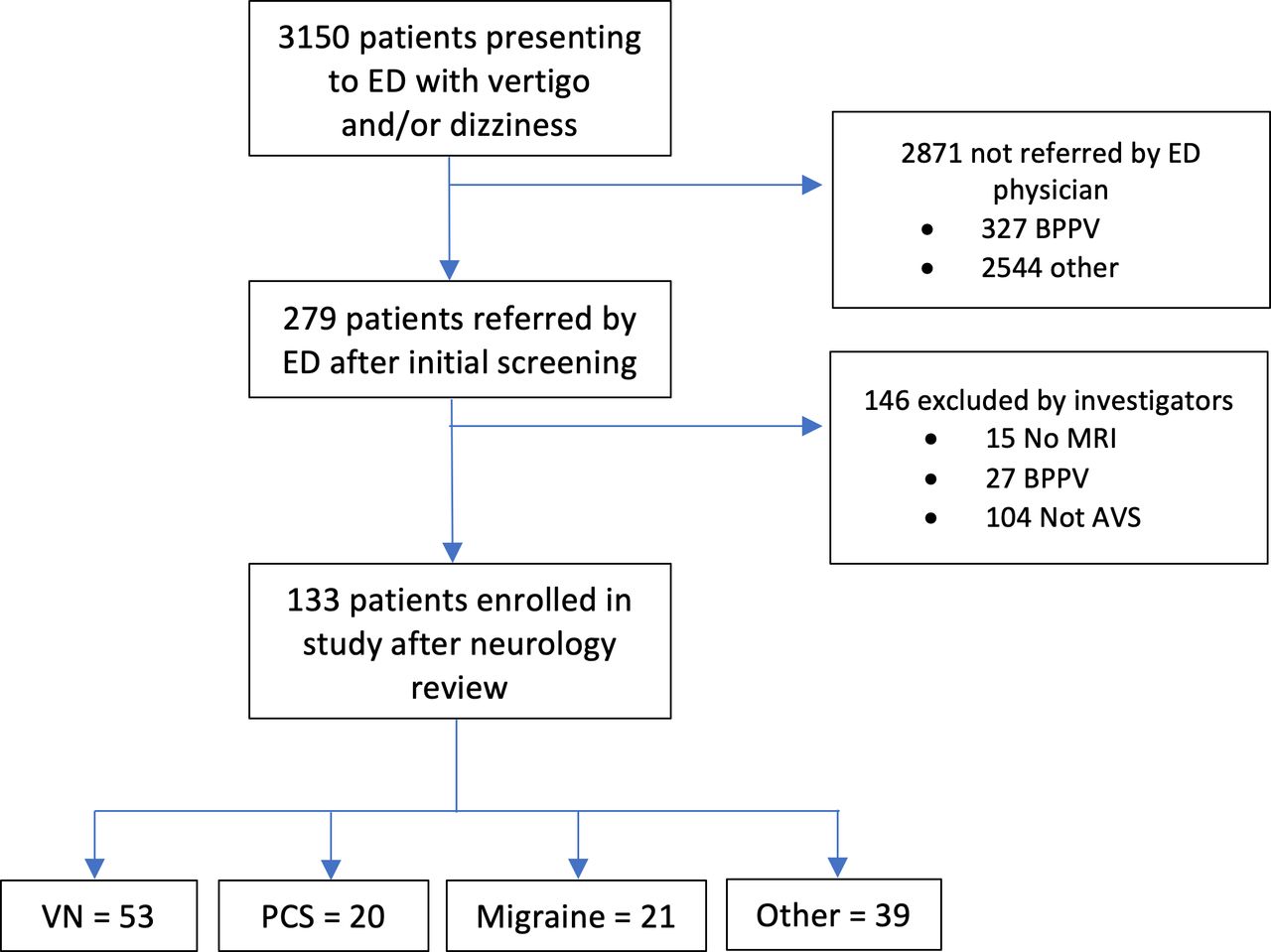
Study enrolment flow chart. AVS, acute vestibular syndrome; BPPV, benign positional vertigo; ED, emergency department; PCS, posterior circulation stroke; VN, vestibular neuritis.
One hundred and thirty-three patients were included in the study; the mean age was 62 years and 54% were male. Baseline characteristics and vascular risk factor profiles are summarised in table 1. Fifty-three patients (40%) were diagnosed with VN, 20 (15%) with PCS, 21 (16%) with migraine and 39 (29%) with other causes of AVS. Other causes included unspecified peripheral vestibular dysfunction (with a diverse range of diagnoses such as acute on chronic vestibulopathy, persistent perceptual postural dizziness and bilateral vestibulopathy) (n=19), orthostatic hypotension (n=8), anticonvulsant or other drug toxicity (n=5), cardiac dysrhythmia (n=4), Meniere’s disease (n=2) and vestibular paroxysmia (n=1). Other clinical features were similar between groups (table 2). No adverse effects were recorded following either b-HIT or v-HIT.
Baseline characteristics, cardiovascular risk factors and length of inpatient stay of patients enrolled with acute vestibular syndrome
Symptoms, examination and investigation findings
In comparison with patients with VN, those with PCS tended to be older (mean age=68.5 ±10.6 vs 60.1±14.5, p=0.14), and had more cardiovascular risk factors (mean 3.0 vs 1.6, p=0.002). Patients with PCS had higher rates of smoking, diabetes mellitus, prior stroke and ischaemic heart disease. Patients with migraine were younger than those with PCS and VN (53.7±15, p=0.006). The mean length of stay did not significantly differ between groups (VN 3.3±2.8, PCS 2.8±4.7, migraine 2.3±1.9, other cause vertigo 3.3±3.0 days).
There was moderate agreement between b-HIT and v-HIT (κ=0.64, p<0.0001) in the diagnosis of VN. The standard HINTS had a sensitivity of 83%, specificity of 86% and a false positive rate of 13.8% for the diagnosis of VN (table 3). The v-HIT had a higher sensitivity 94% than b-HIT and HINTS and a lower false positive rate of 6.3% for the diagnosis of VN. The ‘v-HINTS’ (HINTS examination with v-HIT substituted for b-HIT) was superior to the standard HINTS with a sensitivity of 89% and a specificity of 96% for diagnosis of VN. There was a false positive rate of 3.8% (table 3).
Accuracy of assessments for diagnosis of vestibular neuritis
Mean VOR gains in ipsilateral (or both when lesion was not lateralised) horizontal canals were significantly lower in VN (0.56±0.29) compared with PCS (0.88±0.28 p<0.001) or migraine (1.00±0.18 p<0.001). Similar results were seen for anterior canal gains but there was no significant difference between posterior canal gains. This is consistent with the pattern of VN involving the superior vestibular nerve thus affecting the anterior and horizontal canals (table 4).
v-HIT horizontal canal gains and saccade prevalence by final diagnosis
Supplemental material
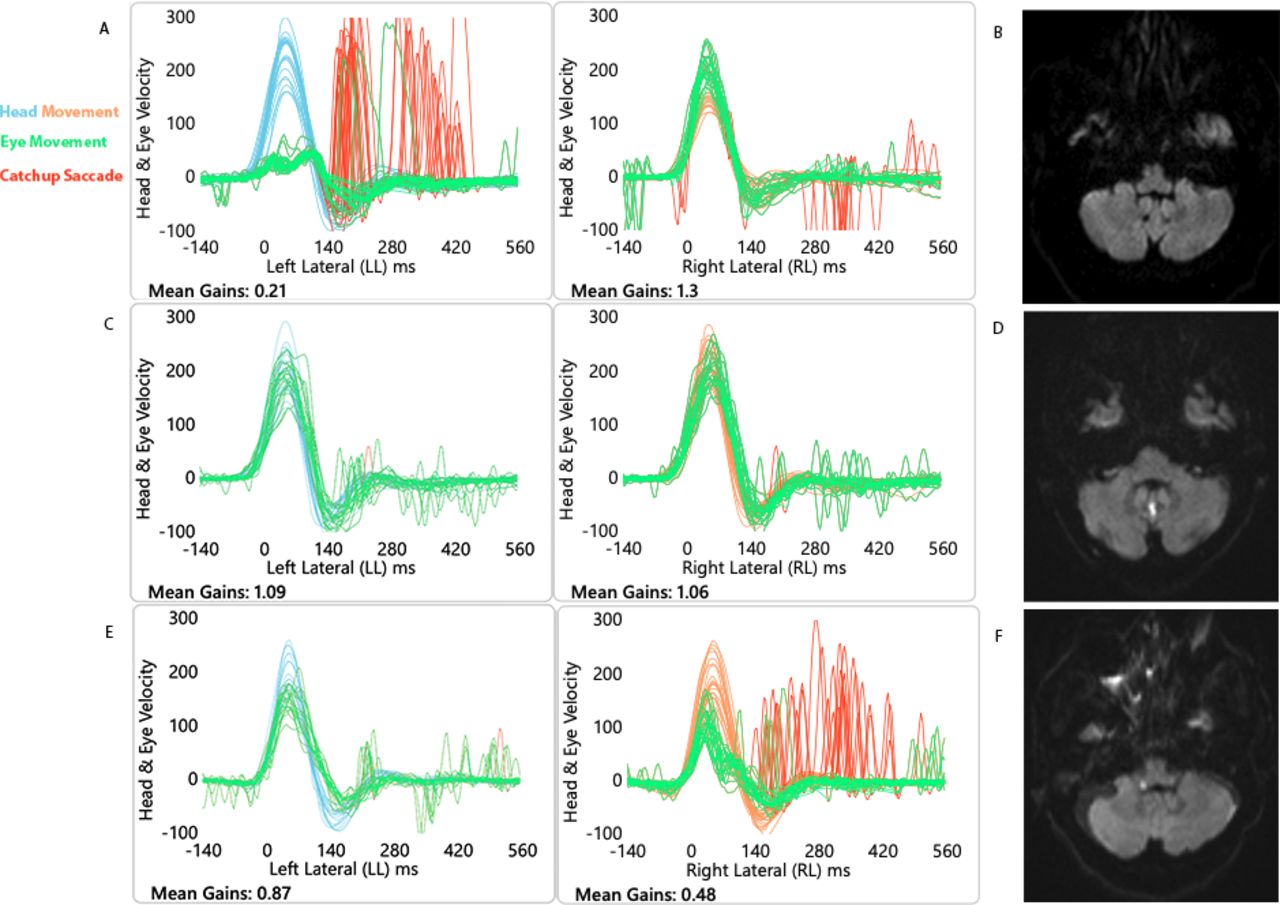
PCSs were located in the medulla (n=6, 30%), cerebellar hemisphere (n=10, 50%), cerebellar vermis (n=2, 10%) and pons (n=2, 10%). There were four strokes with an abnormal v-HIT and these were located in the dorsolateral medulla (n=2), cerebellar hemisphere (n=1) and cerebellar vermis (n=1) (figure 2). Of these, three also had a peripheral HINTS examination.
{kind=link}
{kind=link}
v-HIT traces from horizontal (lateral) canals and DWI MRI scans. (A, B) VN with classical v-HIT result and normal MRI, (C, D) Cerebellar vermis stroke with normal v-HIT, (E, F) Dorsal medulla stroke with abnormal v-HIT (false positive). DWI, diffusion-weighted imaging; v-HIT, video head impulse test.
Discussion
Our study was a pragmatic assessment of the use of v-HIT as an adjunct to clinical assessment of vertigo in the ED of a large metropolitan comprehensive stroke centre. This is the largest prospective study of the use of v-HIT by non-neuro-otologists in routine practice to differentiate VN from a diagnosis of PCS. We used a definition of abnormal v-HIT that has been validated in the literature13 and combined this with the previously validated clinical HINTS examination.7
The sensitivity of both the v-HIT alone and the HINTS exam was lower than that reported in the original studies of the HINTS assessment7 but comparable to results reported when the examination was performed by clinicians with a variable neuro-otology experience.8 9 18–20 The v-HIT assessment offered improvement in sensitivity over the standard HINTS assessment (94% vs 83%). The use of v-HIT in combination with the HINTS exam was the most reliable tool to rule out PCS in our cohort with a false positive rate of only 3.8% compared with 21% relying on b-HIT alone, 6% on v-HIT alone and 14% with HINTS testing. Therefore, the most reliable diagnosis of VN, and thereby exclusion of PCS, was a combination of v-HIT and HINTS examination, a so-called v-HINTS or quantitative HINTS. The additional presence of acute hearing loss (v-HINTS plus), a feature that may suggest ischaemia of the territory of the AICA/labyrinthine artery,21 did not improve the diagnostic accuracy of the v-HINTS assessment. Although we found HINTS to have a higher false positive rate than a v-HINTS assessment, it remains a valuable clinical tool in suspected cases of PCS.
Our study inclusion criteria were broad and included a range of diagnoses for AVS including migraine, Meniere’s disease and drug toxicity. In many cases, an alternative diagnosis of AVS was not made until several days later after further investigations such as drug levels and continuous blood pressure monitoring became available. This reflects real world clinical practice in a busy metropolitan ED with a large culturally and linguistically diverse population. Clear description of the clinical syndrome was often confounded by language barriers or in patients with cognitive deficits. We used a definition of AVS that did not require the presence of spontaneous nystagmus as many patients were referred for assessment after either significant delay and/or after being prescribed antiemetic medications which may have impacted on clinical assessment. Identification of subjects who fulfilled diagnostic criteria for VN did not significantly influence length of hospital stay, which averaged 3 days in both stroke and non-stroke patients, in part due to the acute symptomatic nature of VN, which often requires in-patient hydration, antiemetic therapy and gait physiotherapy.
PCS was the underlying cause of AVS in 15% of our cohort. Although v-HINTS was abnormal, suggestive of a peripheral lesion, in only four of the PCS patients, these strokes were not necessarily limited to the vestibular nuclei and/or complex which are well described to be associated with an abnormal ‘peripheral’ b-HIT.21 In two PCS patients, the cerebellar hemisphere and/or vermis were involved. Our findings are consistent with previous studies demonstrating abnormal VOR gain from focal cerebellar lesions presumably due to disturbed modulation and/or inhibition of target neurons in the cerebellum on ipsilesional vestibular nuclei.14
The limitations of our study were that recruitment was halted prior to the prespecified number of PCS cases (n=30) due to the uncertain impact of the ongoing COVID-19 pandemic. As mentioned earlier, a large proportion of our patients were treated with potential vestibular suppressant medication, most commonly intravenous prochlorperazine for management of acute nausea and vomiting. This may have impacted both the assessment of nystagmus as well as the accuracy of the v-HIT assessment. We performed the study during business hours due to limitations of available personnel after hours. This may have overestimated the proportion of patients with severe symptoms and/or PCS as healthy patients with mild symptoms may have been discharged directly from the ED if they presented outside of business hours. This may also explain the similar length of stay between groups, as those patients admitted after hours and referred during business hours may be more likely to have severe symptoms or other barriers to discharge from the ED. Unlike PCS, there is no gold standard definition of VN. We incorporated b-HINTS and v-HINTS in our definition of VN. The interpretation of our calculated sensitivity and specificity is therefore problematic for both. However, our demonstration of a greater sensitivity and specificity for v-HINTS compared with b-HINTS is an observation which has important implications for the diagnosis of VN by non-experts.
A further limitation is that v-HIT may not be readily available in acute or resource-poor settings.
Conclusion
In a prospective real-world cohort reflecting clinical practice, the v-HIT is a useful adjunct to bedside clinical examination for the diagnosis of acute peripheral vestibulopathy and to rule out PCS. The v-HIT was superior to the b-HIT and HINTS assessment by non-expert clinicians. However, to achieve the lowest false positive rate, and thus most accurate exclusion of PCS, the v-HIT should be used in combination with HINTS assessment. Future studies are needed to determine the cost–benefit of using v-HIT in the acute setting, considering factors such as patient length of stay and ED workflow.
Data availability statement
Data are available on reasonable request. Please contact corresponding author for requests for data sharing.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by South Western Sydney Local Health District Human Research Ethics Committee (HREC/13/RPAH/591). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We wish to acknowledge the assistance of Dr. Wei Xua, senior biostatistician for help with our analysis. We also wish to thank Dr. Ramesh Cuganesan, neuroradiologist, for assistance reviewing imaging.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @JThomasNeuro, @Scientosis
Contributors JOT performed data collection, data analysis, drafting of manuscript and was involved in final design of study. AS, AV, CB and NO were involved in ongoing data collection and participant recruitment. AS was involved in initial conception of study. DC and CC-S were involved in initial conception of study as well as review and processing of data, critical review of and final approval of the manuscript. CC-S is the author acting as guarantor. MW, ZC, PMM and PW were involved in initial conception of study and review of final manuscript.
Funding Partial funding was provided by Sydney South West Local Health District, Health Beyond Research Innovation Grant for purchase of equipment.
Competing interests No, there are no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.