Article Text

Statistics from Altmetric.com
Case 1
A 53-year-old independent woman developed a severe headache 10 days following her first ChAdOx1 vaccination that progressed to right-sided weakness a week later. The patient had an autoimmune background of polymyalgia rheumatica and cutaneous lupus erythematosus on long-term prednisone. A CT acute stroke protocol demonstrated an extensive left common carotid thrombus extending into the left internal carotid artery (ICA) with a large penumbra of the left middle cerebral artery territory. There was an incidental finding of bilateral segmental pulmonary emboli on the CT angiogram arch circle of Willis. The patient was administered intravenous alteplase and transferred for emergency endovascular clot retrieval.
En route, the patient was found to have marked thrombocytopenia (platelet count 40×109/L), an elevated D-dimer of 8.55 mg/L (normal <0.50 mg/L) and fibrinogen level at the lower limit of normal (2.1 g/L, reference 2–4 g/L). Thrombolysis was promptly ceased given the severe thrombocytopenia and she underwent endovascular clot retrieval with excellent angiographic result. Post-thrombectomy, low-dose argatroban was commenced (due to its short half life given she had been thrombolysed), aiming for a below-conventional target activated partial thromboplastin time (APTT) as well as 1 g/kg intravenous immunoglobulin (IVIg) for two consecutive days. She had no ongoing neurological deficit following thrombectomy and partial thrombolysis, and no bleeding complications.
During her admission, she developed lower limb pain and arterial duplex studies demonstrated a non-occlusive popliteal arterial thrombus. PF4/polyanion IgG antibody was borderline positive by immunoassay (Stago ELISA) on day 4 of admission, and a diagnosis of vaccine-induced thrombotic thrombocytopenia (VITT) was made. Functional VITT assays demonstrated mixed results with a positive serotonin release assay (SRA) but negative customised flow cytometry and Multiplate platelet aggregation tests.
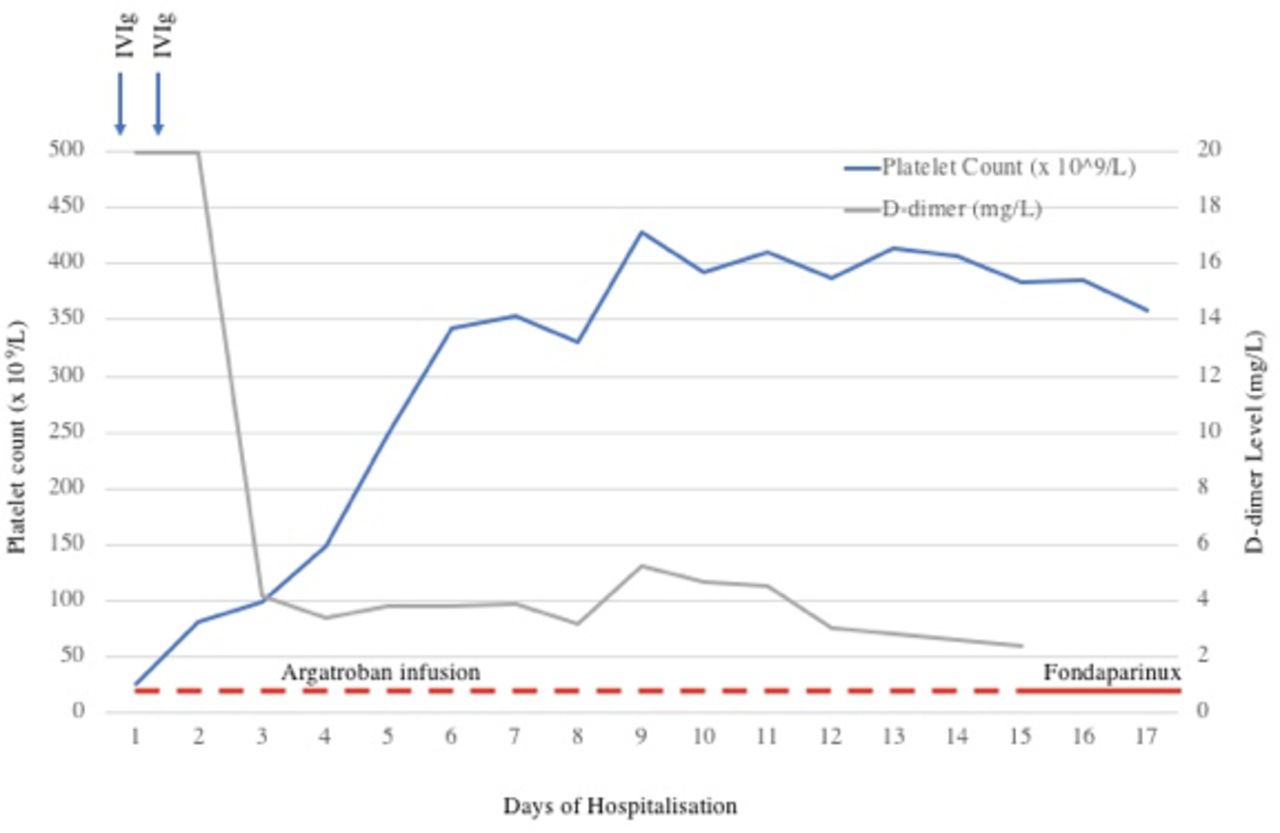
The patient’s coagulation parameters steadily improved over the course of 11 days on argatroban and a further two doses of 0.5 g/kg IVIg (figure 1). She was transitioned to apixaban 5 mg two times per day on day 9 after initial presentation and was able to be discharged home the following day with no deficits. Three months later, she remained clinically well with ongoing improvement in her platelet count with mild ongoing thrombocytopenia.

Consumptive coagulopathy trend for patient 1 during hospitalisation. IVIg, intravenous immunoglobulin.
Case 2
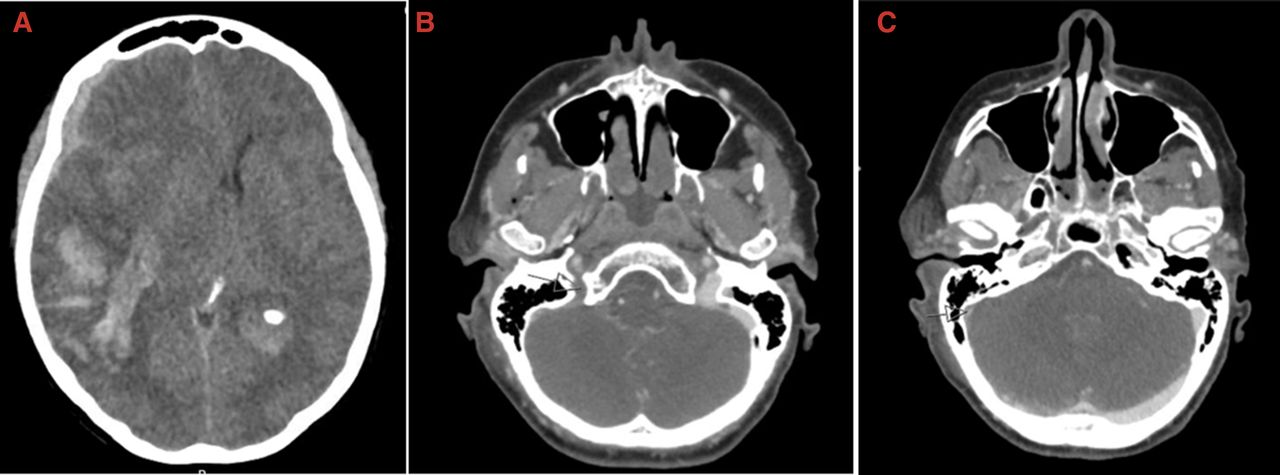
A 67-year-old woman with no comorbidities presented to a regional hospital with a 1-week history of severe headache following her first ChAdOx1 vaccination 17 days prior. Initially, she was alert and oriented; however, she became acutely obtunded. CT brain demonstrated extensive right-sided temporal lobe haemorrhage with mass effect (figure 2). Of note, there was also a hyperdense focus seen abutting the right transverse sinus suspicious for venous sinus thrombosis.

Axial slices of CT brain demonstrating (A) intraparenchymal haematoma within right temporal lobe extending into the occipital lobe with extra-axial haematoma adjacent to frontal, temporal and parietal lobes. (B, C) Axial CT venogram with images showing partial thrombosis of superior aspect of the right internal jugular vein.
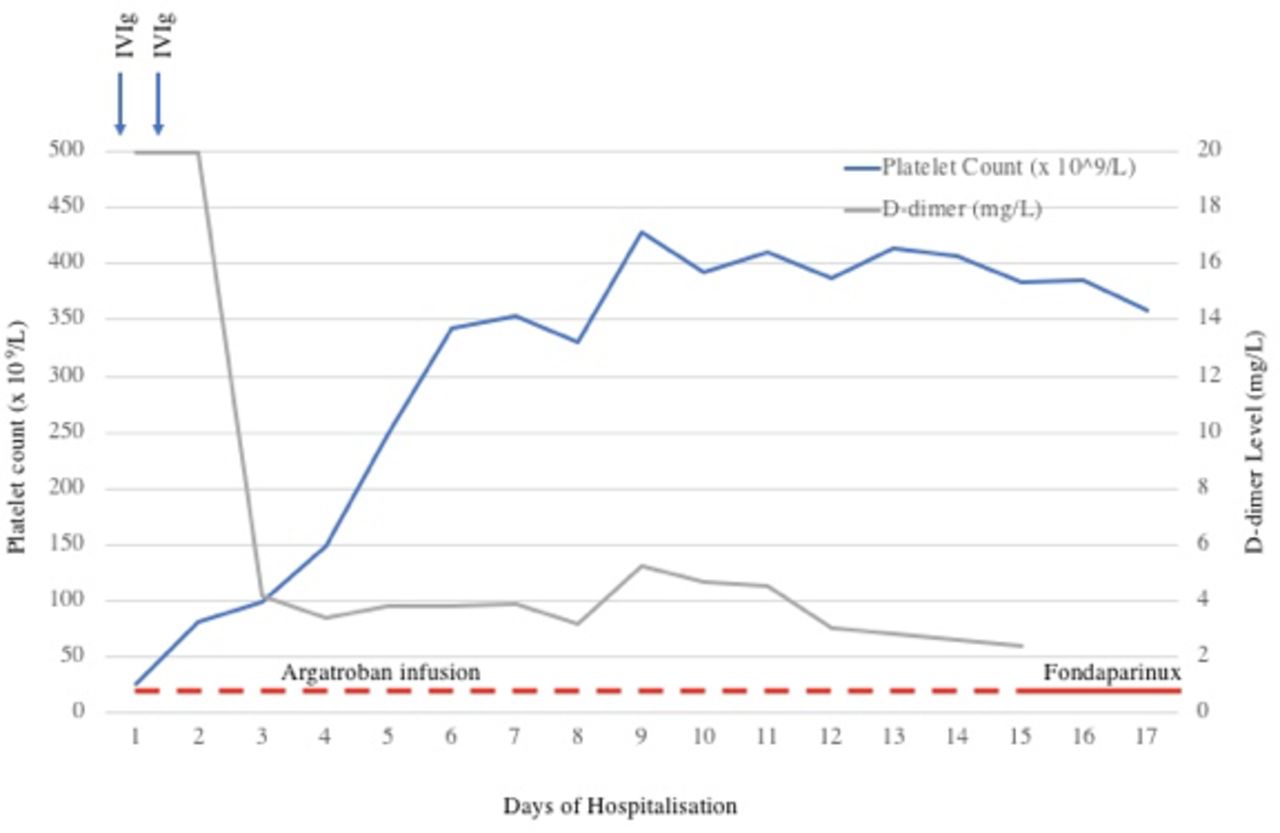
The patient was intubated then transferred to a tertiary centre with neurosurgical expertise where she underwent an emergency right-sided decompressive craniectomy and temporal intracranial haemorrhage removal. Cortical venous thrombosis of the vein of Labbe was noted at her craniectomy. Initial pathology demonstrated evidence of a severe thrombocytopenia (platelet count of 26×109/L), markedly elevated D-dimer >20 mg/L and a low fibrinogen level at 0.9 g/L (figure 3). She was administered two consecutive daily doses of 1 g/kg induction IVIg and was commenced on a low-dose argatroban infusion on day 1 postoperatively.
{kind=link}
{kind=link}
{kind=link}
Coagulopathy trend for patient 2 during hospitalisation. IVIg, intravenous immunoglobulin.
Despite maximal multimodal intensive care unit (ICU) therapy for control of her raised intracranial pressure, progress CT brain and CT venogram 3 days later demonstrated ongoing extensive parenchymal brain haemorrhage and severe cerebral venous sinus thrombosis (CVST). Her APTT targets were lowered. While in ICU, the patient was noted to have limb mottling with poor peripheral pulse and found to have occlusive thrombi in the posterior tibial artery, radial artery and soleal vein.
Significant platelet increment, rising fibrinogen and decreasing D-dimer levels were noted following IVIg (figure 3). PF4 heparin ELISA testing was negative but SRA returned a low positive result. The remainder of her thrombophilia screen was negative. She was diagnosed with VITT given the high clinical suspicion and positive functional VITT assay.
The patient was extubated on day 14. Progress CT brain and venogram demonstrated stable multicompartmental haemorrhage, resolution of mass effect and partial resolution of CVST. She was transitioned from argatroban to fondaparinux on day 15 after removal of the intracranial pressure monitor with subsequent stable anti-Xa levels. She was discharged to a rehabilitation unit 1 month after presentation. Continued improvement ensued over several months, and at last follow-up 3 months after admission she was independently mobile but requiring some assistance from family members, exhibiting mild left-sided neglect and a hemianopia.
Case 3
A 57-year-old usually well woman presented to a regional hospital with convulsive status epilepticus requiring intubation with a propofol infusion and phenytoin loading. This was on a background of having a first dose of the ChAdOx1 nCoV-19 vaccination 10 days prior. CT brain and venogram demonstrated extensive CVST with a large left temporo-occipital haemorrhagic transformation of a venous infarct with a mild degree of midline shift and transtentorial herniation. A hyperdensity within the left ICA from the cavernous to cervical segments was thought to reflect intraluminal thrombosis. Bloods revealed severe thrombocytopenia (platelet count 14×109/L), low fibrinogen (1.6 g/L) and elevated D-dimer (42 mg/L). She was transferred to a tertiary centre with neurosurgical and haematology expertise. Given the suspicion for VITT, she was administered 1 g/kg IVIg, 1 g of methylprednisolone and commenced on a low-dose argatroban infusion.
Urgent cerebral angiography demonstrated complete occlusion of the left ICA from the cervical segment, non-occlusive thrombus within the proximal right ICA and extensive CVST. Thrombectomy of the right cervical ICA and left internal jugular vein (IJV) was performed, with mild residual non-occlusive clot persisting in the right ICA and near complete recanalisation of the dural venous sinuses and minimal residual clot within the inferior left IJV. Surgical evacuation of the intracranial haematoma was not performed due to the severity of thrombocytopenia.
Two further days of intravenous methylprednisolone was followed by weaning high-dose prednisone and a further dose of 1 g/kg IVIg. The day after presentation and clot retrieval, she became peripherally cold with limb mottling. Given the concern for extensive clot burden, imaging of her vasculature was performed which demonstrated bilateral segmental pulmonary emboli, non-occlusive thrombi of the descending aorta and extensive occlusive thrombi of the arterial and venous system of the right upper limb. There was no evidence of splanchnic thrombosis.
Given the severity of her thrombosis, she also underwent plasmapheresis for 2 days with steady improvements in her platelet count and coagulopathy. Her argatroban infusion was continued. Repeat CT brain on days 2 and 5 of admission demonstrated stable multicompartmental haemorrhages.
PF4/polyanion IgG antibody was detected by immunoassay (Stago ELISA) confirming the diagnosis of VITT. The patient was able to be extubated 10 days after presentation with deficits of right hemiplegia, global aphasia and right-sided neglect. She was transitioned to apixaban 3 weeks after presentation.
Discussion
VITT syndrome is a rare complication following the ChAdOx1 nCoV-19 recombinant adenoviral vector vaccination.1–3 While venous thrombosis is well recognised, predominantly in the form of CVST, arterial involvement is thought to be rare.4 Our cases were selected from a larger cohort of patients presenting with VITT with neurological involvement at our centre. The cases demonstrate that in addition to venous involvement, the clinical spectrum of VITT can also commonly include arterial thrombosis.
Our results are consistent with a recent case series5 published in late May 2021 that described three patients, all under the age of 45, who each presented with ischaemic stroke on days 11–21 following ChAdOx1 immunisation. Two of these patients, like our cases, also had venous thrombosis with either cerebral venous sinus or portal vein involvement. Similarly, another case series of three patients in Canada treated with IVIg therapy also had arterial thrombosis, with two patients presenting with limb artery thrombosis and the third patient having cerebral venous and arterial thrombosis.6
In June 2021, the Scottish national population-based analysis of 2.53 million people who received their first doses of SARS-CoV-2 vaccines was published.7 This study found that for ChAdOx1 nCoV-19 vaccination, there was evidence suggestive of an association with arterial thromboembolic events. Furthermore, this finding was replicated in a recent descriptive analysis of VigiBase, the world’s largest pharmacovigilance database, that demonstrated the increased risk for venous thromboembolism was evenly shared with arterial thrombotic adverse events for patients who had received the ChAdOx1 immunisation.8
Following on from these studies, the largest comprehensive series of VITT cases reported to date by Pavord et al9 was published which also supports the view that arterial thrombosis occurs in VITT more commonly than previously recognised, with 21% of cases having one or more arterial thrombotic events. Akin to our case series, the most common arterial thromboses were aortic thrombosis or ischaemic limb (12%, n=26) and cardiac or cerebral arterial events (12%, n=26).
Overall, the recent population studies and our cases suggest that there may be an increased risk of CVST and arterial events with ChAdOx1 nCoV-19 vaccination. Moreover, the arterial involvement may be severe. Of note, there are also reports of VITT following the Ad26.CoV2.S vaccination (Johnson & Johnson/Janssen), which, similar to the ChAdOx1 nCoV-19 vaccine, contains replication-incompetent adenoviral vectors, suggesting a pathogenic role of the adenovirus vector rather than viral spike protein in syndrome aetiology.10 In contrast, the two mRNA-based vaccines, BNT162b2 (Pfizer/BioNTech) and mRNA-1273 (Moderna), thus far have not been associated with thrombosis.11
The presentation of this complication with arterial thrombosis causing stroke poses special difficulties in acute management. Thrombolysis is often given in the emergent patient with a neurological deficit, often well before blood results have demonstrated the characteristic abnormalities. However, vigilance is warranted in these situations with an awareness of the possibility of VITT, as thrombocytopenia, especially if it is significant, is a contraindication to thrombolysis. Nevertheless, in certain other scenarios, such therapy is warranted, as in massive pulmonary embolism with circulatory compromise.12 Endovascular clot retrieval, if possible for large vessel occlusive stroke, is preferred but still poses threats given the bleeding and rethrombosis risk.
In summary, while venous thrombosis is well recognised in VITT, our cases highlight that arterial involvement is also common. However, the increased risk of arterial thromboembolic events with VITT appears to remain much lower than the rate of arterial thrombosis seen with COVID-19 infection,13 which may partially explain less recognition with non-occlusive thrombi being asymptomatic. However, given the rarity of VITT, vaccination with ChAdOx1 nCoV-19 should still be considered, taking into account the likelihood of COVID-19 infection as well as other available vaccine types and their inherent risks in that community.
Ethics statements
Patient consent for publication
Footnotes
Contributors Planning, conduction, reporting, conceptualisation and design: SC, GAM, RC, KD, CW, KN. Acquisition and interpretation of data: SC, GAM, KN. SC and KN had full access to the data and are responsible for the overall content as guarantors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.