Article Text

Abstract
Background/Purpose Cardiac arrest is a common cause of death and neurological injury; therapeutic cooling for neuroprotection is standard of care. Despite numerous and ongoing trials targeting a specified cooling temperature for a target duration, the concept of temperature dose—the duration spent at a given depth of hypothermia—is not as well explored.
Methods In this retrospective study, we examined 66 patients 18 years of age or older undergoing therapeutic hypothermia for cardiac arrest between 2007 and 2010 to assess the relationship of temperature dose with outcomes. Demographic, clinical, outcome and temperature data were collected. Demographic and clinical data underwent bivariate regression analysis for association with outcome. Time-temperature curves were divided into pre-determined temperature thresholds and assessed by logistic regression analysis for association with outcome. A second, multivariate regression analysis was performed controlling for factors associated with poor outcomes.
Results Old age was significantly associated with poor outcome and a shockable arrest rhythm was significantly associated with positive outcome. Subjects spent an average of 2.82 hours below 35°C, 7.31 hours ≥35°C to ≤36.5°C, 24.75 hours >36.5 to <38.0°C and 7.06 hours ≥38°C. Logistic regression analysis revealed borderline significant positive association between good outcome and time at a cooling depth (35°C–36.5°C, p=0.05); adjusted for old age, the association became significant (p=0.04).
Conclusion Controlling for old age, longer durations between >35°C, ≤36.5°C during therapeutic hypothermia for cardiac arrest were significantly associated with good clinical outcomes. Time spent within a given temperature range may be useful for measuring the effect of temperature management.
- CLINICAL NEUROLOGY
- INTENSIVE CARE
Data availability statement
Data are available on reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Therapeutic temperature management for cardiac arrest has been shown to improve neurological outcomes; however, the depth and duration of cooling are areas of active investigation. In this retrospective study, we examined the concept of temperature dose—the duration spent at a given depth of hypothermia—and its association with outcome, as a novel measure of temperature management.
What this study adds
Our study demonstrates an association between longer dosing durations at moderate cooling temperatures (>35°C, ≤36.5°C) and positive outcomes after cardiac arrest, when controlled for old age; the analysis of time spent within a given temperature range represents a more granular measure of temperature dose.
How this study might affect research, practice and/or policy
Our study is consistent with mounting evidence supporting the efficacy of moderate temperature cooling strategies for cardiac arrest, and it represents a proof-of-concept for measuring time-temperature dose in hypothermia studies.
Introduction
Cardiac arrest is a common cause of death, and in survivors, neurological complications can be devastating. Studies have shown that therapeutic hypothermia improves neurologic outcomes in patients with out-of-hospital cardiac arrest.1–3 More recent data suggests moderate temperature management to a target of 36.0°C results in similar outcomes to targeting 33.0°C.4 While meta-analyses have debated the salutary effect of targeted temperature management, it has gained wide adoption.5–7
Existing studies have investigated the effect of mild hypothermia compared with controlled euthermia.3 5 Despite numerous and ongoing trials on optimal cooling depth, the concept of temperature dose—the duration at a given depth of hypothermia—is not as well explored. While there has been some investigation into prolonged cooling beyond 24 hours, the focus has generally been on the effect at a fixed temperature, not the relative impact of different phases of cooling.8 9 In this retrospective study, we analysed 66 patients undergoing therapeutic hypothermia between 2007 and 2010 for cardiac arrest to determine the impact of temperature dose on outcomes.
Methods
Primary research question
In a retrospective review of patients suffering cardiac arrest and being treated with our institution’s therapeutic hypothermia protocol, is there a relationship between outcome and thermal dose (defined as time spent in a temperature range)?
Subject selection
Subjects were initially screened through the Duke Enterprise Data Unified Content Explorer (DEDUCE). Inclusion parameters included 18 years of age and older, treatment with therapeutic hypothermia in the setting of coma after cardiac arrest between 2007 and 2010, and use of EEG monitoring during cardiac arrest (the EEG parameter was associated with a separate analysis and was a surrogate for hypothermia patients receiving protocoled care under the guidance of neuro-intensivists during this study period). Initial DEDUCE results were manually screened, and patients receiving therapeutic hypothermia for other indications and patients misdocumented as having undergone cardiac arrest were excluded. Patients were included regardless of the aetiology of cardiac arrest or arrest rhythm. Patients initially treated at an outside facility and transferred to our institution were also excluded.
Data abstraction
Demographic data (age at time of arrest, gender, inpatient vs outpatient arrest location and time to return of spontaneous circulation (ROSC) when available) were manually collected from the electronic health record. As a retrospective cohort, Ulstein variables (such as witnessed cardiac arrest, lay CPR) were not consistently documented in this sample group, as such surrogate markers for arrest severity and resuscitation quality, including defibrillation-eligible arrest rhythm, presenting lactic acid, and pH were collected.10 Outcomes were identified on basis of discharge disposition and were dichotomised as poor (skilled nursing facility, hospice or death discharge) or good (home or rehab discharge). Temperature‐time coordinates were manually abstracted for each patient, from the first post‐arrest temperature on file to the last documented temperature prior to death, discharge or 48 hours postrewarming to 37.0°C (figure 1). When multiple temperature sources were available, temperatures were recorded from core temperature sources in the following preferential order: urinary bladder, rectum, oesophagus, mouth, axilla. Since the timing of temperature recording was not consistent, temperatures were recorded as available and not at fixed intervals. Given the limitations of electronic hospital record format at the time of the study, time-temperature data was collected manually.
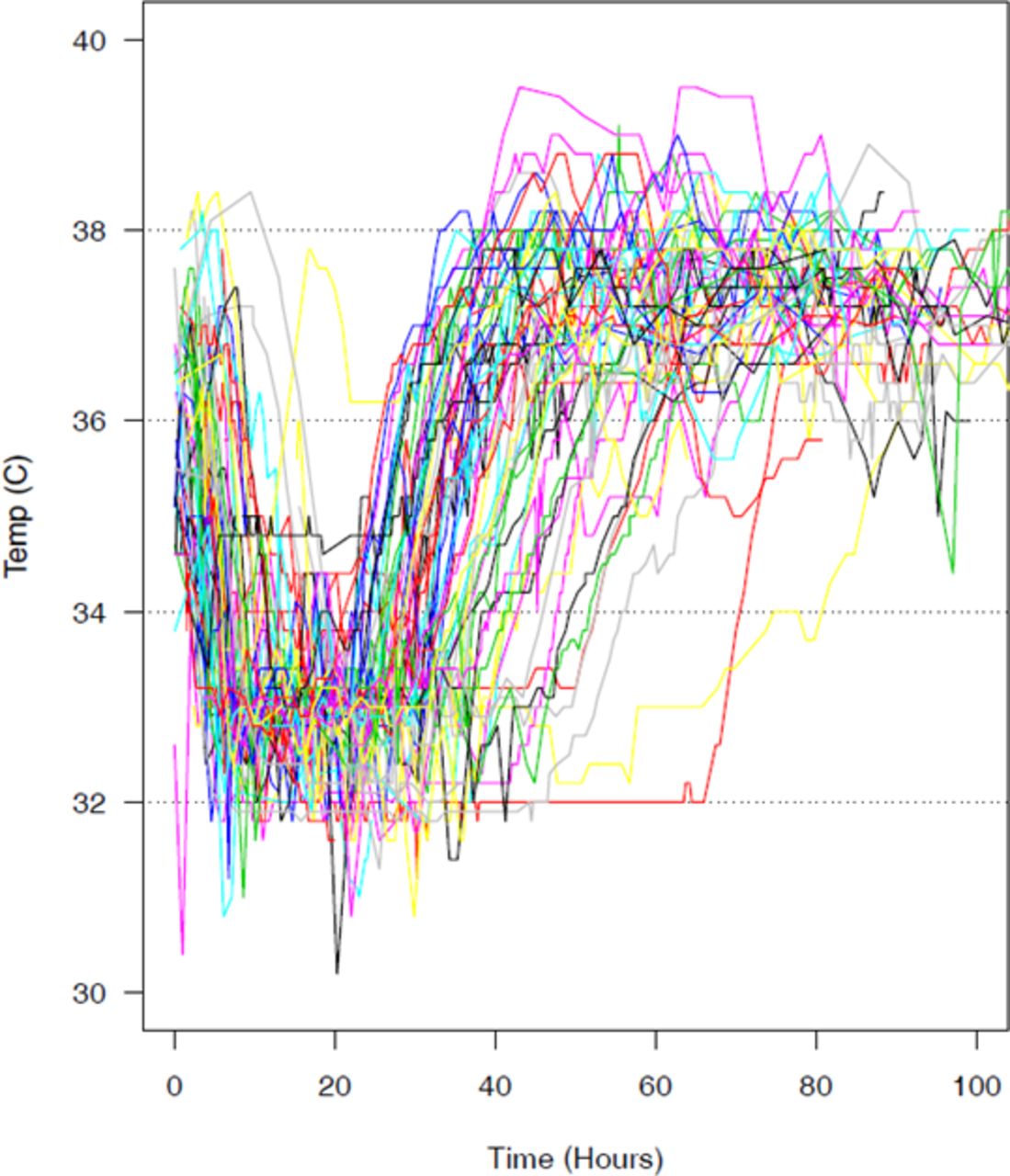
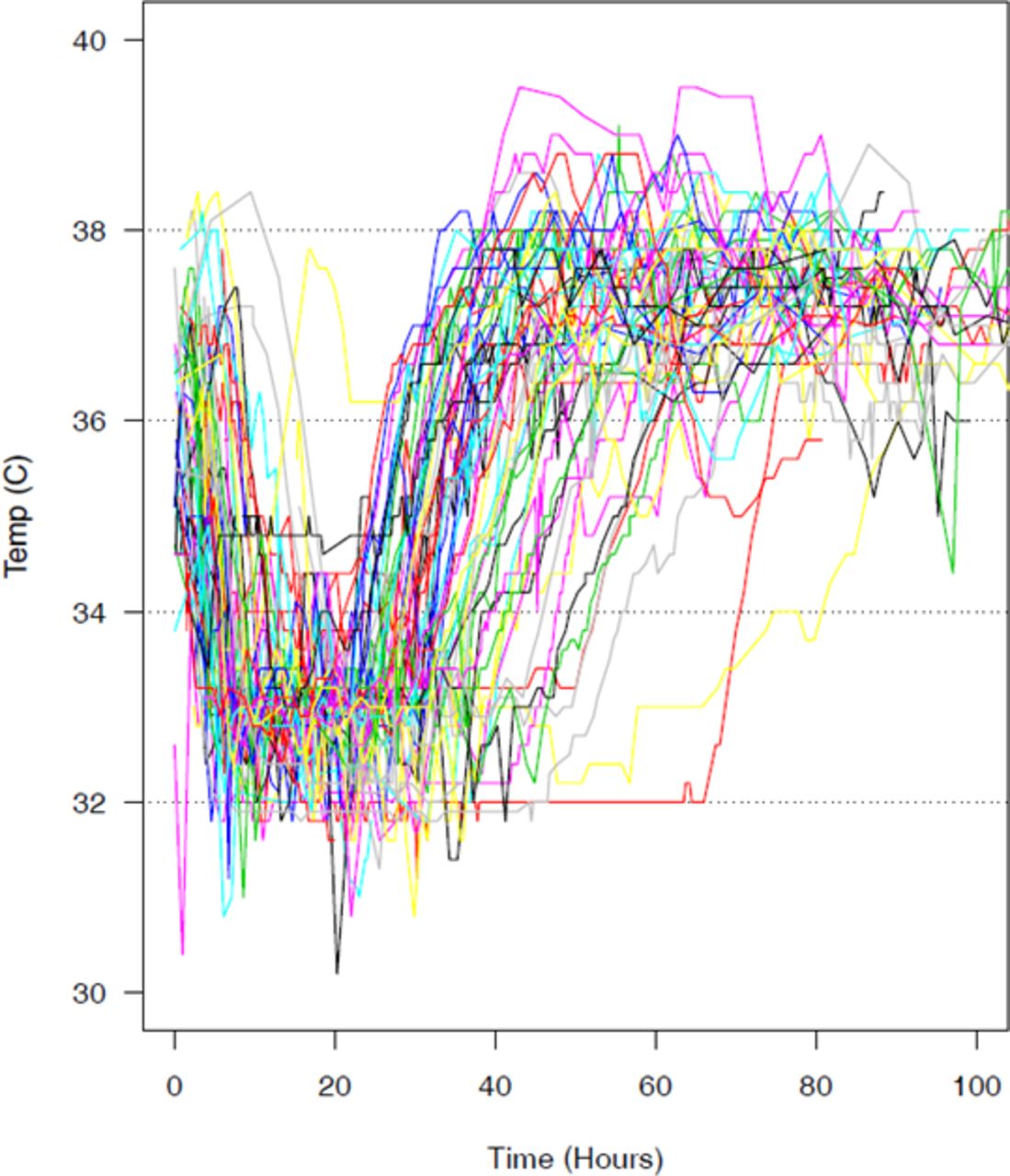{kind=link}
Time-temperature curves for the 66 patient cohort.
Data analysis
Demographics
Statistical analysis was performed using R Core Team, 2014.11 Continuous demographic and clinical variables were summarised qualitatively. Patients were divided into age terciles (young ≤51 years, middle=52–65 years, old >65 years). Initial postarrest pH and lactic acid, deepest cooling temperature, variation at target temperature, warming rates, and overall duration of hypothermia (time below 37°C) was summarised by quartiles. Demographic variables were assessed for association with outcome by bivariate logistic regression analysis.
Temperature data
Given manual data abstraction and possibility of nursing record error, outlier data points were identified algorithmically and set to ‘missing’ in subsequent analysis, but were maintained in the data record. Cooling dose was summarised by time in hours spent in predetermined temperature thresholds (deep cooling <35°C, mild cooling ≥35°C to ≤36.5°C, euthermia >36.5°C to <38.0°C, fever ≥38°C), and was derived for each temperature time course. Durations of time within each of the four predetermined temperature ranges was assessed individually for association with positive or negative outcome using bivariate logistic regression analysis. A second, multivariate regression analysis was performed controlling for demographic factors identified as having significant (p<0.05) associations with poor outcomes.
Results
Our 66 patients had a median age of 55.5 years, with a range of 19–93; 56% were male (table 1). The population was closely divided between shockable and non-shockable arrest rhythms. The cohort demonstrated a median initial lactate of 7.9 mm/L and a median initial pH of 7.20. 39% of patients were discharged under a dichotomised good disposition, of which 33% of patients went to rehabilitation units and 6% went home. Sixty-one per cent of patients were discharged with poor dispositions, of which 6% went to a skilled nursing facility and 45% died or were discharged to hospice.
Critical demographic data for patient receiving protocoled therapeutic hypothermia for cardiac arrest
Among demographic variables, (table 2), only old age (>65 years old), was significantly (p<0.05) correlated with poor outcomes (LOR=‐1.95, CI=(−3.39 to –0.50), p<0.01). Among clinical variables, a shockable arrest rhythm (ventricular fibrillation or tachycardia) was significantly associated with positive outcome (LOR=2.53, CI=(1.32, 3.74), p<<0.01). Gender, post‐arrest pH and lactic acid, cooling method, and other age groups were not statistically associated with outcome.
Bivariate regression analysis of demographic factors with patient outcome
The mean temperature nadir for the study group was 32.88°C, with a mean temperature variability at target depth of 0.17°C (table 3). Patients warmed at a mean rate of 0.30°C/hour. The mean duration for cooling for the study group was 22.49 hours (table 4). The patients spent an average of 2.82 hours below 35°C, 7.31 hours between ≥35°C to ≤36.5°C, 24.75 hours >36.5°C to <38.0°C and 7.06 hours ≥38°C. Bivariate logistic regression models of outcome against cooling depth, variability, warming rate and time spent in each of the temperature categories demonstrated a borderline significant positive association only between good outcome and longer cooling at temperatures greater than 35°C and less than or equal to 36.5°C (LOR=0.07, 95% CI=(0.00 to0.14)) p=0.05; table 4), with the log-OR expressing an effect per-hour spent within a temperature range.
General characteristics of therapeutic hypothermia within the cohort including mean depth of cooling and mean temperature variation at target temperature (in degrees centigrade), and mean warming rate (in degrees centigrade per hour)
Duration spent within temperature control categories
Given the strong association between age and outcome, a second set of logistic regression analyses were performed between outcome and each of the temperature characteristics while controlling for age (table 5). When adjusted for the influence of old age, the association of positive outcome and time spent ≥35°C to ≤36.5°C became significant (LOR=0.08, 95% CI=(0.01 to 0.16), p=0.04). In contrast, depth of cooling (LOR=0.34, 95% CI=(−0.92 to 1.74), p=0.60), time spent below 35°C (LOR=−0.06, 95% CI=(−0.18 to 0.04), p=0.27), time spent above 36.5°C and less than 38°C (LOR=0.01, CI=(95% CI −0.03 to 0.16), p=0.52) and time spent febrile (≥38°C; LOR=−0.05, 95% CI=(−0.12 to 0.02), p=0.16) did not demonstrate statistically discernable effects on outcome after adjusting for old age.
Univariate regression analysis of outcomes with regards to depth of cooling, variability at target temperature, warming rate, and time within cooling interval, with the coefficient expressing a log-OR, first without adjustment for impact of old age and subsequently with adjustment
Discussion
In this retrospective analysis of 66 patients undergoing protocoled therapeutic hypothermia after cardiac arrest, we studied the effect of temperature dosing on patient outcome, which we defined as time spent within predetermined temperature thresholds during treatment. When controlling for patient age, the strongest univariate predictor of poor outcome in our cohort, the length of time spent between >35°C and ≤36.5°C was associated with improved outcomes. While the change in log-odds ratio for time spent in this temperature group is numerically small (LOR=0.08), it expresses a per-hour effect. For example, 2 hours spent in this temperature range would be associated with a log-odds ratio 0.16, or about a 17% increase in the odds of a favourable outcome (OR=exp(0.16)=1.174). This duration-dependent association suggests the potential for greater effect with longer cooling periods.
In human studies, the bulk of prospective investigations examine the impact of depth of cooling.3 4 There is animal data suggesting better neuronal protection with longer durations of cooling and a positive impact on survival.12 Prospective trials have been conducted on prolonged cooling depth at 33°C for 48-hours over 24-hours, without significant benefit over shorter durations, and potentially worse cognitive impairment.8 13 Given the lack of prospective human investigations and our retrospective study associating improved outcomes with longer durations of mild temperature management (temperatures of 36°C±1°C), further research on longer temperature management may be warranted.
In our study population, the duration of cooling with temperatures >36.5°C or ≤35°C had no statistically significant association with improved outcomes. These results are consistent with the Targeted Temperature Management trial, which showed that cooling to 36°C was effective in the management of cardiac arrest.4 The relative lack of impact from deeper cooling is consistent with mounting data suggesting that temperature control is more significant than maximal depth of cooling.7 14 These results are also consistent with a prospective study demonstrating that there were no significant differences in outcomes for survivors of out-of-hospital cardiac arrest maintained at target temperature of 33°C for 24 and 48 hours.8
Further, duration of posthypothermia fever was not found to have an association with outcome. This is similar to the findings of Gebhardt et al, which showed that fever has a negative survival impact, but only in patients not treated with therapeutic hypothermia.15
Our study does have its limitations, most notably that it is retrospective and is based on a relatively small patient population, which includes patients suffering from both shockable and non-shockable arrest rhythms. Hence, our failure to detect certain associations may be a matter of statistical power. Despite our small sample size, our use of logistical regression models is sound: based on a simulation study, Peduzzi et al find logistic regression models to be stable when the number of events per variable (EPV) exceeds 10.16 The models we fit have EPVs >10, as we observe 26 events and include one or two covariates.
The retrospective data collection, along with the mixed inpatient and outpatient population, was also limited in the collection of some Ulstein variables, inconsistently documented in the patient charts, notably lay-rescuer CPR, witnessing of cardiac arrest and ROSC; while not as robust, we did collect and assess surrogate measures of arrest severity, such as postarrest serum lactate and pH. Further, demographics and outcomes data are comparable to a recent temperature management trial examining patients suffering from non-shockable arrest rhythms, supporting our study’s generalisability.17
Second, without adjustment for age, our finding of improved outcomes in moderate cooling only borders on significance (p=0.05). However, given the a priori expected and statistically discernable effect of old age in our relatively small patient population, the statistical adjustment is reasonable. Another potential concern is the age of the data set; the dates of sample collection were during a period of more clinical practice heterogeneity for hypothermia management in our institution. This permitted a wider range of time-temperature courses for our assessment.
Conclusion
While both depth and total duration of cooling have been investigated, our analysis uniquely approaches the impact of time spent within given temperature ranges. When controlled for old age, longer durations spent between >35°C, ≤36.5°C during therapeutic hypothermia for cardiac arrest were significantly associated with good clinical outcomes in our patient population. The analysis of time spent within a given temperature range represents a more granular measure of temperature dose and may be useful for measuring therapeutic interventions using temperature management. While this small retrospective analysis is limited in and of itself, it represents a proof of concept for more granular time-temperature dose assessments. Further prospective investigation into the optimal time-temperature dosing of hypothermia after cardiac arrest is warranted.
Data availability statement
Data are available on reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
Approval for this study was obtained through the Duke Health Institutional Review Board (protocol number Pro00031926). Given retrospective nature of the study, the absence of identifiable patient information collected, and the high proportion of decedents expected in the data set, consent was waived.
Acknowledgments
We would like to extend our thanks to thanks to Ms. Christina Yancey for her initial participation in case screening. We would like to thank the 2015 Spring Semester Duke University Statistical Consulting Class for their contribution to statistical methodology.
References
Footnotes
Contributors MWL contributed to the study concept, data collection, data interpretation, manuscript outlining, writing and revision. CG contributed to the study concept, data interpretation, and critical revision of the manuscript for content. BGM contributed to the study concept, data collection, and critical revision for content. JP contributed to the study concept, data collection, and critical revision for content. EI contributed to statistical analysis, interpretation of the study data and critical revision for content. BK contributed to the study concept, data collection, data interpretation, manuscript outlining, writing, and critical revision for content. All named authors take responsibility for the integrity of the work as a whole, have given final approval for its publication. MWL accepts full responsibility for the finished work and is guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.