Article Text

Abstract
Case A 39-year-old man with thymoma-associated acetylcholine receptor antibody myasthenia gravis (MG) presented with fevers, night sweats, abdominal pain and weight loss. Marked splenomegaly and intra-abdominal lymphadenopathy were found. Biopsies confirmed disseminated Mycobacterium genavense infection. Despite antimicrobials and reduced immunosuppressive medications, he worsened. We suspected a thymoma-associated cytokine inhibitory antibody. The addition of subcutaneous interferon-gamma (IFN-γ) induced clinical and radiological improvement. His antimicrobials were able to be ceased. MG remained stable. Subsequent testing demonstrated an endogenous interleukin-12 (IL-12) inhibitor, likely inhibiting the IL-12/IFN-γ axis crucial for defence against mycobacterial infections.
Discussion This case illustrates the autoimmune manifestations that can occur with thymoma. It illustrates the benefit of exogenous IFN-γ in overcoming the immune deficit. In this case, its use did not exacerbate existing autoimmune disease or trigger others. We raise awareness of the need to consider cytokine pathway defects as a contributing factor to refractory atypical infections in patients with thymoma-associated MG.
- MYASTHENIA
- INTERFERON
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Thymoma is linked with loss of immune self-tolerance and the presence of autoimmunity. Manifestations includes myasthenia gravis, and increased prevalence of anti-cytokine antibodies.
WHAT THIS STUDY ADDS
We present a rare case of refractory Mycobacterium genavense infection due to the presence of an IL-2 inhibitor in an individual with thymoma-associated myasthenia gravis on immunosuppression. We highlight the challenges in the diagnosis of an underlying immunodeficiency in this setting and discuss the role of exogenous interferon as a management strategy.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
We raise awareness of the need to consider cytokine pathway defects as a contributing factor to refractory atypical infections in patients with thymoma-associated myasthenia gravis.
Case report
A 39-year-old Caucasian man presented in 2009 with an 8-week history of fevers, night sweats, nausea, abdominal pain and distension and 5 kg weight loss. He reported no respiratory or other gastrointestinal symptoms and did not have any unwell contacts or history of overseas travel. He cared for an aviary of Gouldian finches (Erythrura gouldiae), which included cleaning and removing dead birds. There is no personal or family history of recurrent or opportunistic infections.
Three years earlier, he was diagnosed with acetylcholine receptor (AChR) antibody-positive myasthenia gravis (MG) after presenting with ptosis, dysarthria and dysphagia. A type B2 thymoma was confirmed on surgical resection and treatment with prednisolone and pyridostigmine was commenced.
In 2008, he suffered a myasthenic crisis with severe bulbar and respiratory muscle involvement necessitating a feeding tube (Myasthenia Gravis Foundation of America (MGFA) grade 4b). This improved with treatment (3-weekly plasma exchange, cyclosporine 150 mg two times per day, azathioprine 50 mg daily and prednisolone 25 mg alternate days) and he remained clinically stable until this presentation. At presentation, he had mild residual bulbar features, including dysarthria, dysphagia and fatigable chewing.
On examination, he was afebrile, and had splenomegaly, periumbilical and epigastric tenderness. There was no palpable lymphadenopathy.
Full blood examination showed haemoglobin of 111 g/L (130–170 g/L) and lymphocytes of 1.0×109/L (1.2–2.7 x 109 /L). C reactive protein was 63 mg/L.
Lymphocyte subsets, including CD4 T-cell counts, were all within normal limits except for reduced CD19 pan B-cell count at 0.03×109/L (0.05–0.41×109/L). Immunoglobulin levels were not reduced, and HIV screen was negative. Bacterial and mycobacterial blood cultures were unrevealing.
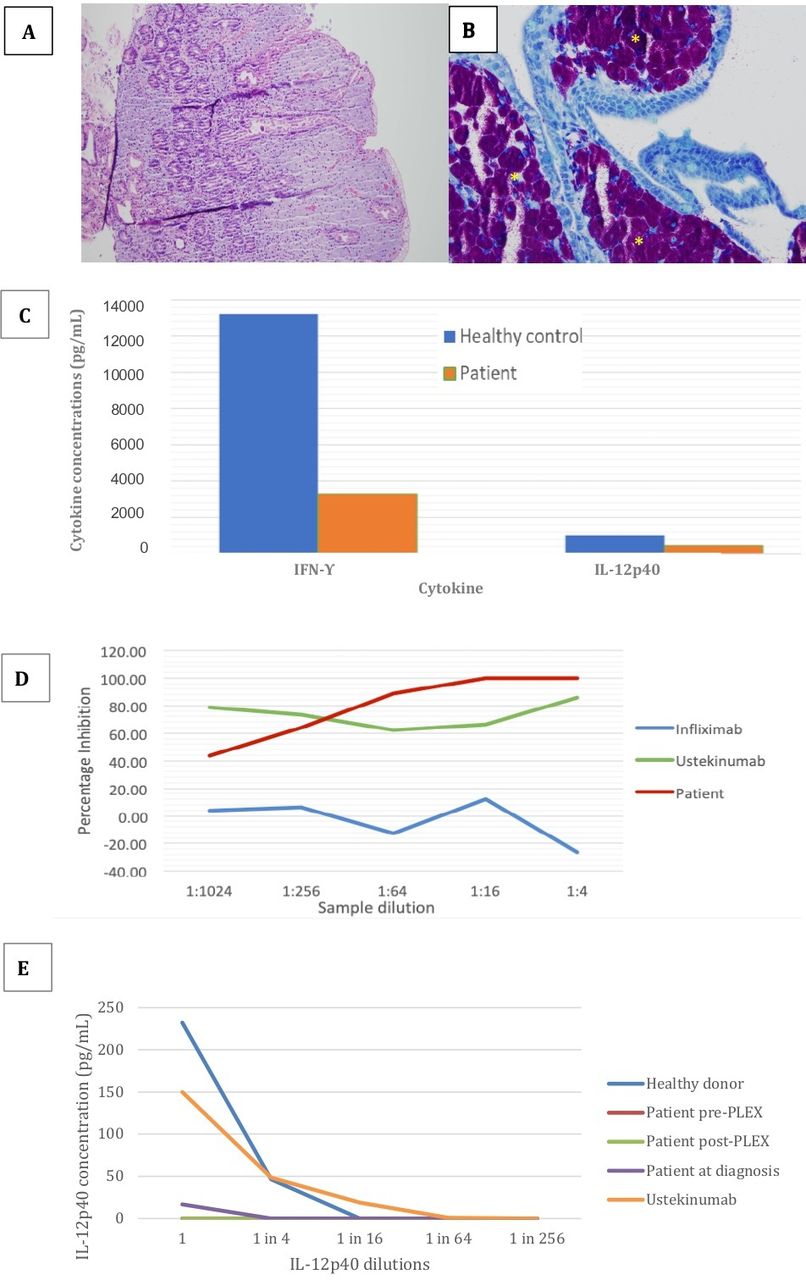
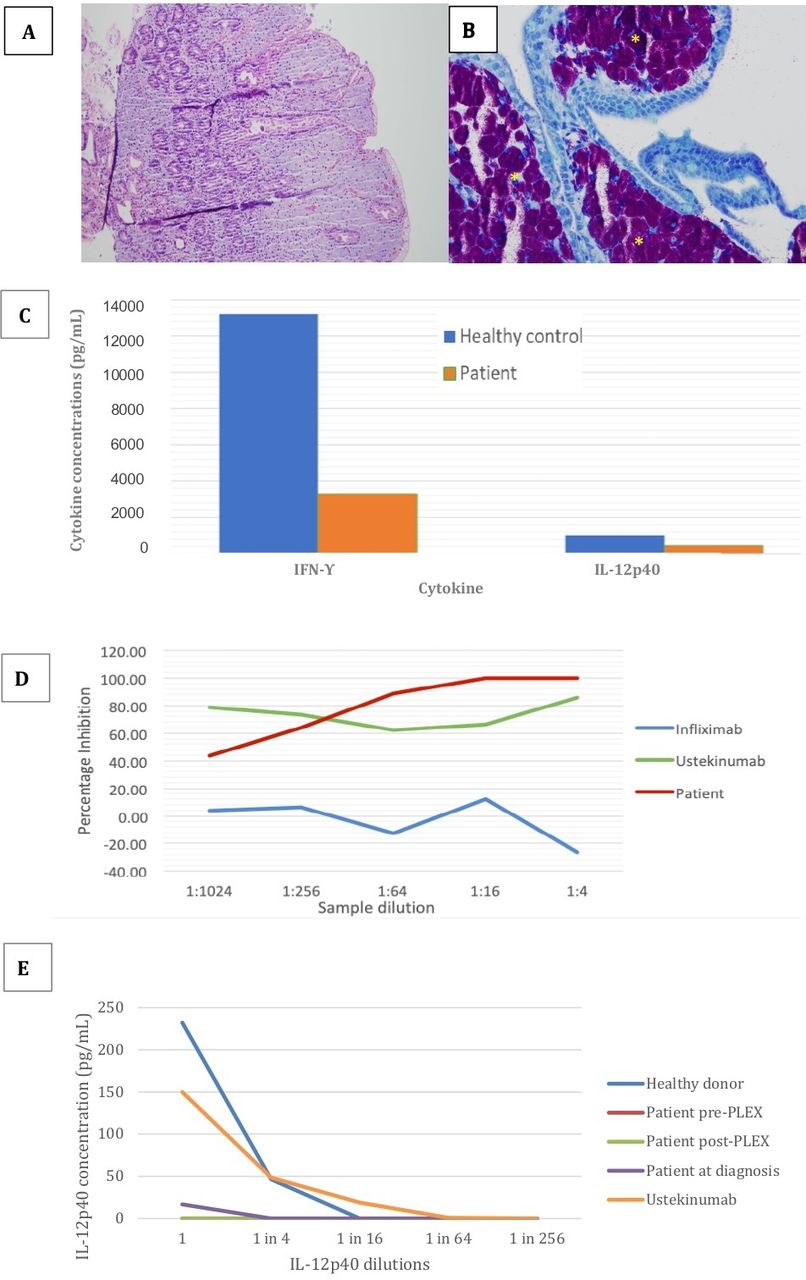
CT scan demonstrated splenomegaly (15 cm) and periaortic and mesenteric lymphadenopathy with no evidence of thymoma recurrence or residual thymic tissue. Gastroscopy showed a macroscopically abnormal duodenum with a fine, nodular appearance. Gastric and duodenal biopsies revealed broad, shortened villi (figure 1A) and marked diffuse to confluent infiltrates of histiocytes in the lamina propria. Innumerable acid-fast bacilli were seen on Ziehl-Neelsen stain (figure 1B). Mycobacterium genavense was identified on molecular sequencing, leading to a diagnosis of disseminated M. genavense infection in an immunocompromised patient. Empirical therapy with rifampicin, ethambutol, moxifloxacin and clarithromycin was started. Cyclosporine and azathioprine were discontinued and the frequency of plasma exchange was increased with sequential intravenous immunoglobulin.
{kind=link}
(A) Duodenal biopsy—H&E stain. (B) Duodenal biopsy—Ziehl-Neelsen stain (400×) showing numerous, almost confluent acid-fast bacilli (dark purple areas indicated by asterisk). (C) Cytokine production in response to mitogen stimulation. (D) Inhibition of IL-12p40 detection. Detection of IL-12p40 is completely inhibited when patient plasma is added at dilutions of 1:16 and above. Monoclonal antibodies were used as controls: Ustekinumab (anti-IL-12/23, positive control) and infliximab (anti-tumour necrosis factor-alpha (TNF-α), irrelevant negative control). Inhibition was compared with healthy human immunoglobulin. (E) Amount of IL-12p40 recovered after mixing serum samples with different dilutions of IL-12p40. This showed that our patient’s samples prevented recovery of IL-12p40, with no difference pre- and post-plasma exchange (PLEX). (These red and green lines are overlapping on the graph.) IFN-γ, interferon-gamma; IL-12, interleukin-12.
Despite treatment, interval abdominal CT scan revealed progressive splenomegaly (17.8 cm) and intra-abdominal lymphadenopathy, raising concerns of refractory infection or lymphoma, as well as potential splenic rupture. Further biopsies of the mesenteric lymph nodes, stomach and duodenum demonstrated countless mycobacteria, consistent with ongoing infection. Drug sensitivities were unavailable as M. genavense could not be cultured.
Following a multidisciplinary discussion, subcutaneous interferon-gamma (IFN-γ) was trialled, resulting in substantial fever. Dose was reduced to induce only low-grade fevers and chills (25 μg three times a week). Over the next 12 months, the patient’s symptoms resolved. Repeat CT scan demonstrated a reduction in the degree of splenomegaly and intra-abdominal lymphadenopathy. Antimicrobials were slowly weaned off over 6 years and he remains well 11 years later, with controlled myasthenia.
Given the rare opportunistic infection, stored and newly collected blood samples were investigated for cytokine antibodies producing immunodeficiency. Due to ease of use and wide availability, the tuberculosis IFN-γ release assay was used to screen for reduced IFN-γ production. After incubation, a multiplex assay was used to measure cytokine production within the supernatant. The patient’s sample showed a markedly reduced IFN-γ response to mitogen stimulation compared with healthy controls (figure 1C). Moreover, the analysis also revealed a reduced concentration of interleukin-12 (IL-12).
Research-based inhibition studies showed that adding the patient’s sample to IL-12p40 resulted in inhibition of analyte recovery at sample concentrations above 1:16 (figure 1D), suggesting the presence of an IL-12p40 inhibitor. This inhibitory effect was similar to that seen with ustekinumab, a human monoclonal antibody specifically directed against the p40 subunit shared by IL-12 and IL-23. Interestingly, plasma exchange did not substantially reduce inhibition (figure 1E), suggesting that the patient had a very high inhibitor concentration.
Discussion
M. genavense is a fastidious, non-tuberculous mycobacterium that is ubiquitous in the environment. It has been isolated from tap water,1 birds including Gouldian finches2 and the gastrointestinal tract of healthy individuals.3 Unlike Mycobacterium avium complex, M. genavense infections tend to affect the gastrointestinal tract.4
M. genavense was first recognised as an opportunistic infection in HIV-affected individuals with a CD4 count of <100 cells/µL. More recently, infections have been reported in individuals with cellular immunodeficiency, including solid organ transplant recipients, those with haematological malignancies and those on immune-modulating medications.5 6 To date, infections with M. genavense have not been reported in individuals with thymoma.
The IL-12/IFN-γ axis plays a central role in defending against mycobacterial infections by bridging the innate and adaptive immune response.5 7 8 After encountering mycobacteria, antigen-presenting cells secrete IL-12, which induces the activation and differentiation of T and NK cells and stimulates them to produce IFN-γ. IFN-γ then activates macrophages leading to increased tumour necrosis factor-alpha (TNF-α) production. This step is vital to granuloma formation and the destruction of ingested mycobacteria within macrophages.9 10
Anti-IL-12 antibodies disrupt this axis by preventing IL-12-mediated induction of IFN-γ,11 12 resulting in poor clearance of mycobacteria by macrophages.13 Although IFN-γ may be produced through IL-12-independent pathways, the concentrations are too low to prevent mycobacterial infection or reactivation, as shown in patients with inherited defects of IL-12 pathway.8 9 14 Furthermore, a higher threshold of bacteria may be required to induce macrophage and T-cell responses.13 These may explain why some individuals with impaired immunity present late, with a high burden of mycobacterial disease.
In this case, we initially attributed the M. genavense infection to the potent immunosuppression that the patient was receiving for his MG. Persistent ongoing infection despite reduced immunosuppression and 8 months of antimicrobials prompted an evaluation into possible IL-12/IFN-γ axis defects. This suspicion was confirmed by the reduced IFN-γ production seen in the IFN-γ release assay.
Subsequent laboratory analysis revealed an inhibitory factor against IL-12, similar to ustekinumab. This inhibitor likely accounted for the patient’s failure to clear the mycobacterial infection. The absence of fever and demonstration of mycobacterial-laden macrophages on biopsy prior to exogenous IFN-γ administration supports a functional impediment caused by the IL-12 inhibitor on endogenous IFN-γ production.
As M. genavense could not be cultured,15 multidrug resistance cannot be excluded as a cause for treatment failure. However, the identification of an IL-12 inhibitor and the prompt response to exogenous IFN-γ make this less likely.
Thymoma has been linked with the loss of immune self-tolerance and the presence of autoimmunity, with MG being the most well-described association. Individuals with thymoma have also been found to have an increased frequency of anticytokine antibodies, including those against IFN-α, IL-17, IL-12 and IL-22.16 17 Given the level of these anticytokine antibodies neither correlate with the AChR antibody titre or the clinical severity of MG,16 the control of myasthenic symptoms does not preclude new or ongoing anticytokine antibody production. As our patient had a prior thymectomy and no evidence of residual thymic tissue on imaging, we postulate that the anti-IL-12 inhibitor identified in our case was being produced in a non-thymic lymph organ and that immunosuppression was unable to suppress its production. This hypothesis is supported by a prior study reporting persistent anti-IL-12 antibody despite thymectomy and immunosuppression with prednisolone.18
The decision to use exogenous IFN-γ to overcome a presumed IL-12/IFN-γ blockade was based on data reported by others.19 In our case, only a low dose of IFN-γ was required to elicit an inflammatory response and facilitate clearance of M. genavense. This observation makes the presence of an endogenous IFN-γ autoantibody unlikely, as this would have necessitated much higher doses of IFN-γ to achieve a clinical response. The use of IFN-γ is associated with a theoretical risk of destabilising control of MG by increasing pathogenic AChR antibody production.12 Fortunately, this did not occur.
Serious opportunistic infections are not common in patients with thymoma-associated MG despite the high frequency of anticytokine antibodies and concurrent use of immunosuppressive agents. It has been postulated that (1) the targets of anticytokine antibodies and their corresponding titres are different between individuals; (2) the biological activity of an antibody in vivo is heterogeneous depending on epitope specificity and whether the antibodies are binding or neutralising; and (3) the overlapping human cytokine pathways, with inbuilt redundancies, may partially compensate for possible defects.11 12
Diagnostic tests for cytokine antibodies are not routinely available despite its potential utility. Neutralising autoantibodies against type I interferons were recently shown to be present at disease onset in at least 10% of patients with life-threatening COVID-19 pneumonia, compared with 0% in patients with asymptomatic or mild disease,20 suggesting that the presence of anticytokine antibodies may be more frequent than assumed.
In summary, we present a rare case of refractory M. genavense infection due to the presence of an IL-12 inhibitor in an individual with thymoma-associated MG on immunosuppression. We highlight the challenges in the diagnosis of an underlying immunodeficiency in this setting and discuss the role of exogenous IFN-γ as a management strategy. We also raise awareness of the need to consider cytokine pathway defects as a contributing factor to refractory atypical infections, even in patients who are receiving immunosuppression.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Concord Repatriation General Hospital Research Ethics Committee, local reference number: CH62/6/2020-177. Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Correction notice The article has been corrected since it was published online. The authors would like to notify that the co-author Dr. Hannah Hu was inadvertently omitted from the authorship list. Dr. Hu is affiliated to Department of Immunology, Concord Repatriation General Hospital, Concord, New South Wales, Australia.
Contributors JC contributed to acquisition of data and drafting the manuscript. MN contributed to conception of the work, acquisition of data, analysis and interpretation of data. DSR, EC and SR contributed to conception of the work and interpretation of data. All authors contributed to revision of the manuscript for important intellectual content and approved the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.