Article Text

Abstract
Introduction Cerebral small vessel disease (CSVD) frequently occurs in individuals with vascular risk factors. This condition might go unrecognised or result in only mild functional deficits.
Objective To evaluate the relationship between cardiovascular (CV) risk calculated with the HEARTS app and CSVD burden in a population without cardio-cerebrovascular diseases, and to estimate the prevalence of CSVD in low risk (LR) individuals.
Methods Asymptomatic subjects with vascular risk factors were included from primary health areas in Havana. The WHO’s revised CV disease risk prediction chart (HEARTS app) was applied to all individuals, who were classified into two groups: LR and moderate/high risk (M/HR). Brain MRI was performed in all subjects.
Results 170 patients were included: 43 (25.3%) classified as low CV risk and 127 (74.7%) had M/HR CV risk. Half of the neurologically healthy individuals included displayed cerebral small vessel involvement (51.2%). White matter hyperintensities (WMH) and enlarged perivascular spaces were the most frequent lesions observed in both groups. WMH were more severe and more severe global score for CSVD were more frequent in the M/HR group (57.5%). It was noteworthy that 32.6% of LR-patients also exhibited more severe CSVD. The multivariate regression analysis revealed an independent association of arterial hypertension and age with the severity of CSVD.
Conclusions CV risk stratification through the HEARTS app has limited utility for predicting brain health in individuals with low CV risk. Identifying silent CSVD in individuals with apparently low CV risk is important, especially if they suffer from arterial hypertension.
- MRI
- CARDIOLOGY
- CEREBROVASCULAR DISEASE
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Asymptomatic cerebral small vessel disease (CSVD) frequently occurs in individuals with vascular risk factors, but previous studies have not evaluated if low cardiovascular risk is associated with the absence of this condition.
WHAT THIS STUDY ADDS
For the first time, the calculation of cardiovascular risk with the HEARTS app, revealed the occurrence of CSVD in one third of individuals with low cardiovascular risk.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study evidences the importance of timely detecting this condition, especially in hypertensive individuals, to avoid future neurological complications.
Introduction
Cardiovascular (CV) diseases are the leading causes of mortality worldwide and were responsible for an estimated 17.8 million deaths in 2017, affecting mainly the ageing population. Together, cardio-cerebrovascular diseases make up over 350 million disability-adjusted life-years; that is, years lived in good health lost globally, per year. A large proportion of these deaths and disability in survivors appears to be preventable.1 2
Treatment of cerebrovascular disease due to large artery pathology is well established, but the management of small vessel disease has not received the same level of attention. This is mainly due to the variability of the clinical expression of cerebral small vessel disease (CSVD), which can go under-recognised during the initial stages, and the technical difficulties for its diagnosis in the community.3 4
CSVD is one of the most common vascular diseases of the brain as a result of the subtle and sustained action of vascular risk factors during decades on brain tissue.5 It is a syndrome with clinical and imaging features that in most cases is asymptomatic, but can be recognised in its advanced stages once its symptomatic sequelae develop. CSVD is also a global and dynamic disease, which is not focused on an initial-single lesion, but rather results in widespread lesions with disruptions in structural and functional network connectivity.4 6 7 For that reason, it could be responsible for the development of ischaemic/haemorrhagic strokes, mood disturbances, cognitive impairment, depression, motor and gait dysfunction and is considered the most important contributor to vascular dementia and severity of Alzheimer’s disease.3 8 Brain lesions characteristic of CSVD are best visualised employing magnetic resonance imaging (MRI), which is the gold standard for diagnosis.4 7 9
Several studies have extensively demonstrated the impact that ageing and vascular risk factors have on brain parenchyma, especially arterial hypertension, and brain damage is known to be more frequently present than cardiorenal damage.3 10 11 Nevertheless, the guidelines for diagnosis and treatment of hypertension only include cardiorenal function for routine target organ damage assessment, while the brain is left out.12 13 The reasons for this are obvious, considering that the brain requires highly sensitive imaging techniques (MRI) to demonstrate subclinical brain damage, which are expensive and are not available to screen relatively large populations at risk.3 4
CV diseases and CSVD share common risk factors, and the association between these two conditions has been adequately documented.3 6 8 Thus, an association of CV risk with the severity of CSVD would be expected, and could be useful as a first filter to predict subclinical CSVD in the general population. Furthermore, it would be necessary to establish if neurologically healthy subjects with low CV risk are in fact free from CSVD.
Several risk prediction models have been designed to identify subjects at high risk of CV diseases in order to reduce and control its global burden.14 Recently, the World Health Organization (WHO) developed revised CV disease risk prediction charts that have been adapted to the circumstances of 21 global regions.15 This initiative is active in 21 countries and 1045 primary health centres throughout Latin America and the Caribbean, including Cuba. The main component of this improved application is a calculator (HEARTS app) that is easily applied and widely available; and is expected to help optimise CV risk assessment.16 17
The aim of the present investigation was (1) to evaluate the relationship between CV risk calculated according to the HEARTS app and CSVD burden in a population without cardio or cerebrovascular diseases and (2) to determine the prevalence of CSVD in low risk (LR) individuals.
Patients and methods
Subjects
An observational, descriptive study was conducted in asymptomatic subjects with vascular risk factors. Two hundred and twenty-six patients who attended a CV risk consultation organised in three primary healthcare areas in Havana, Cuba, were consecutively recruited by a general practitioner. The inclusion period extended from January 2015 to June 2018, lasting 6 months in each healthcare area, without overlapping in time. The following criteria were considered for inclusion: both sexes, age ≥35 years, at least one vascular risk factor (arterial hypertension, diabetes mellitus, smoking habit, obesity, hyperlipidaemia) and no known history of cardio-cerebrovascular diseases, kidney dysfunction or malignancies. Forty-three patients were excluded: age <35 years—5; history of cardio-cerebrovascular diseases—21; chronic kidney disease—7; malignancies—5; not willing to participate in the study—5. All subjects complying with these criteria (n=183) were referred for a specialised neurological and general clinical examination by a trained neurologist (MAP) at the Institute of Neurology and Neurosurgery (INN). Patients with clinical signs of cerebrovascular disease, cognitive impairment or with any other neurological impairment, as well as those with ischaemic heart disease or other cardiac diseases identified during the inclusion process were excluded. Eleven patients were excluded: moderate cognitive impairment—2; neurological impairment (movement disorder, focal neurological signs, epilepsy)—3; CV diseases—3; chronic kidney disease—2; malignancy—1. Of the 172 patients evaluated, brain MRI could not be performed in two. The recruiting procedure is summarised in figure 1.
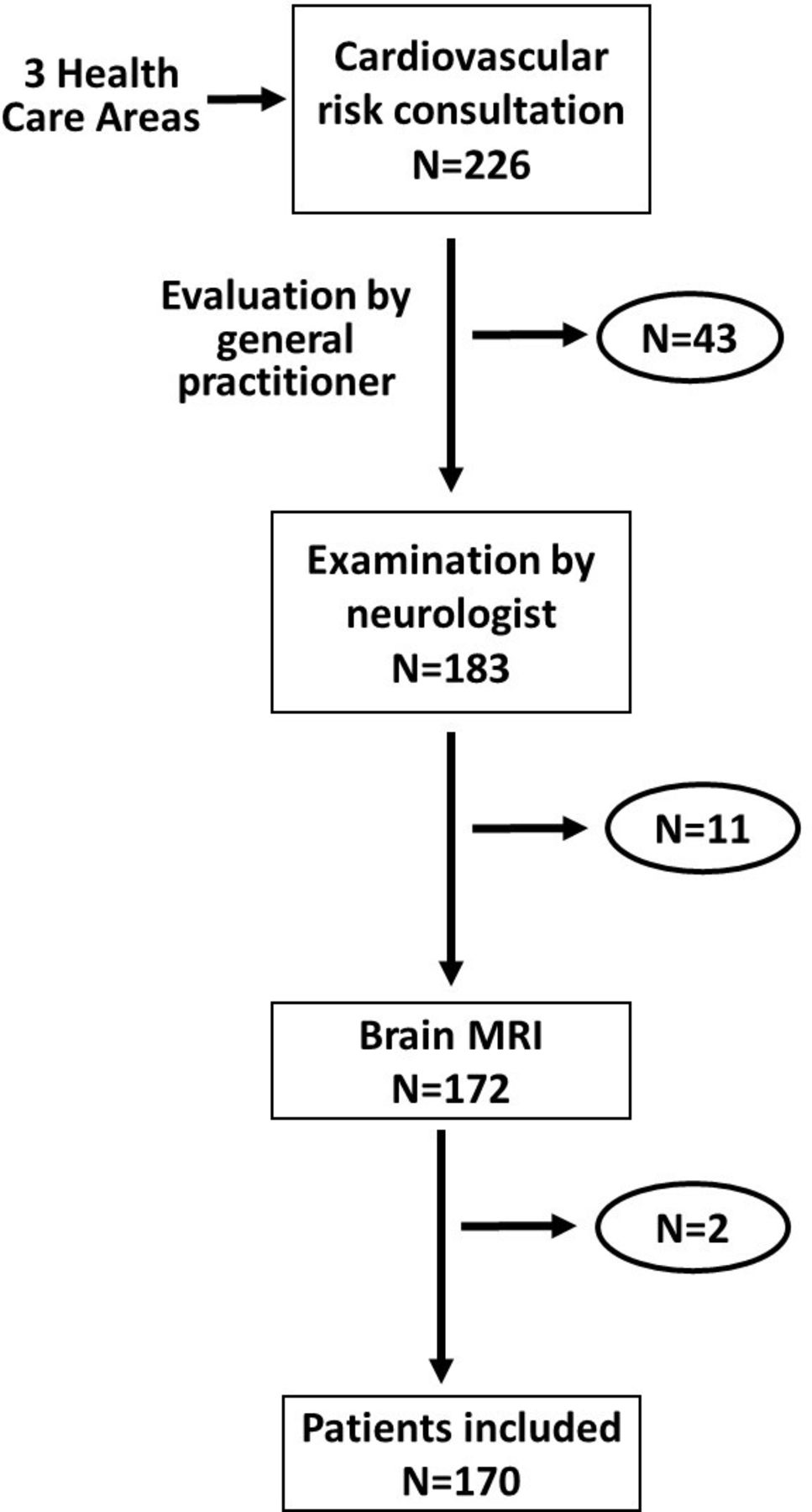
Diagram of the recruiting procedure.
Procedures
At the INN, systolic and diastolic blood pressure were measured as previously described,18 and CV risk evaluation was performed as detailed below. Fasting venous blood was obtained in the morning for routine blood workup with standardised procedures. Brain MRI scanning was performed in all cases within the time frame of the study in each healthcare area.
CV risk assessment
The WHO CV risk prediction chart for Latin America and the Caribbean, which stratifies the risk prediction from an LR value (<5%), to a critical risk value (≥30%), was applied to all subjects included.15
(https://www.paho.org/en/hearts-americas/cardiovascular-risk-calculator-app) This calculator estimates the risk of first time relevant CV disease (myocardial infarction, angina, stroke) in 10 years, for individuals over 40 years of age, including the following variables: sex, age, smoking, SBP, cholesterol levels and the presence of diabetes mellitus. CV risk was then classified in two categories: low CV risk (≤5%) (LR-patients) and moderate+high + very high+critical CV risks (>5%) (M/HR-patients).
Brain MRI protocol
All patients included (n=170) underwent MR imaging on a 3T Magnetom Allegra, Siemens, Germany (n=151) at the Cuban Neurosciences Center and on a 1.5T Magnetom Aera Siemens, Germany (n=19) at the International Center of Neurological Restoration. For each patient conventional MR imaging sequences, such as T1, T2 and FLAIR (fluid-attenuated inversion recovery) were performed, as well as axial T2*-weighted echo-planar imaging (EPI) or SWI (susceptibility-weighted imaging) and DWI (diffusion-weighted imaging) sequences. Scanning time: 26–35 min.
Parameters for the 3T sequences in this study were the following: T1-3D MPRAGE (magnetisation-prepared rapid gradient-echo): TE (echo time), 26 ms; TR (repetition time), 2000 ms; TI (inversion time), 900 ms; section thickness, 0.8 mm; FOV (Field-of-view), 256×204 mm; in-plane voxel size, 0.8×0.8×1 mm; total acquisition time, 9.19 min; T2-weighted: TE, 101 ms; TR, 8020 ms; section thickness, 1.2 mm; FOV, 256×256 mm; in-plane voxel size, 0.5×0.5×2; total acquisition time, 5.37 min; FLAIR 3D: TE, 353 ms; TR, 4800 ms; TI, 1650 ms; section thickness, 1 mm; FOV, 256×256 mm; total acquisition time, 8.24 min.; T2*: TE, 20 ms; TR, 650 ms; section thickness, 1.0 mm; in-plane voxel size, 0.86×0.86×4; total acquisition time, 2.43 min; DWI: double spin EPI sequence; TR, 6300; TE, 81 ms, flip angle, 90°; contiguous slices, 2.4 mm isotropic voxels; matrix 128×128; diffusion-sensitising encoding gradients, 41 directions; b-value 0 and b-value 1000 s/mm2; total acquisition time, from 5 to 10 min.

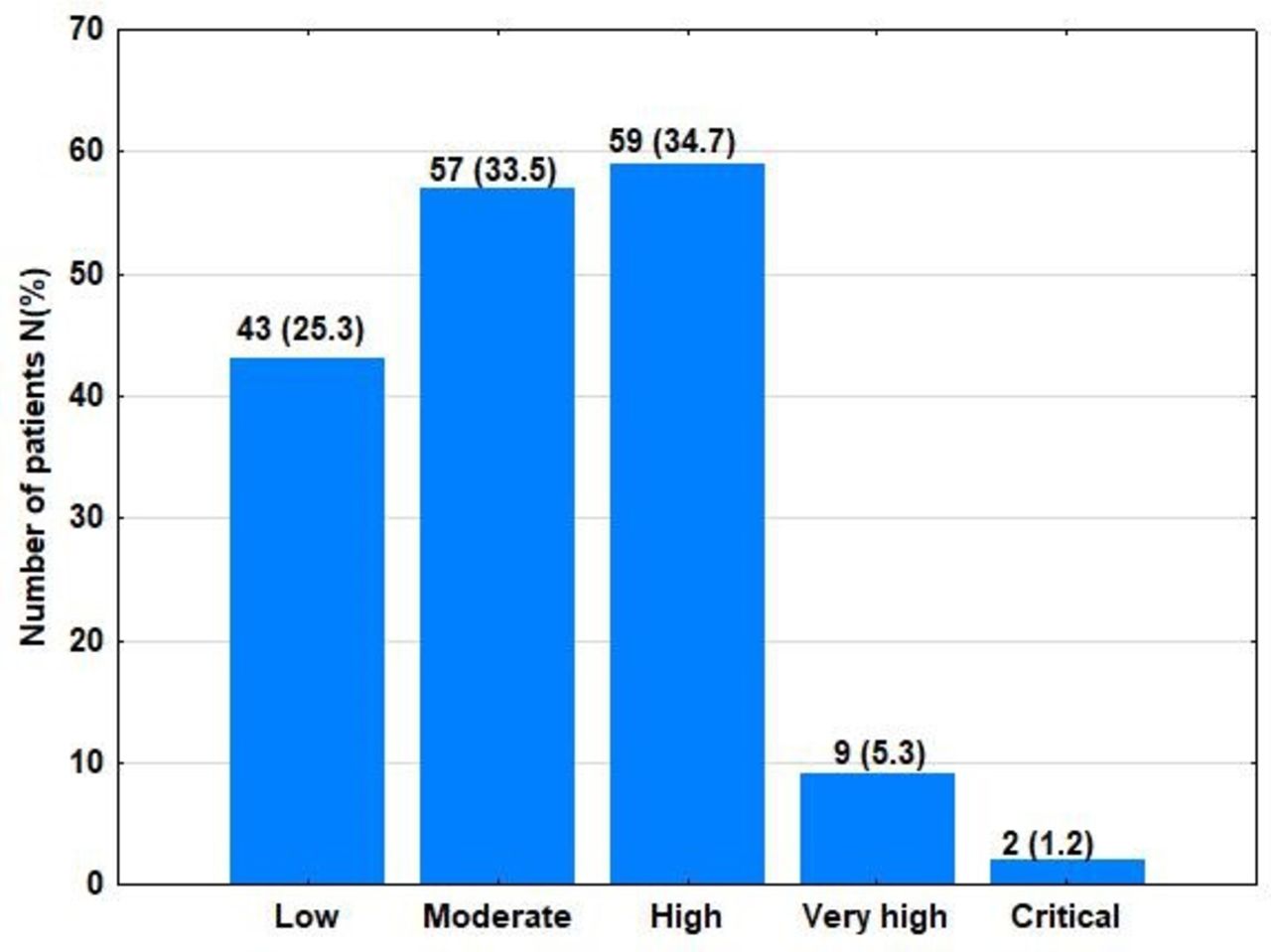
Distribution of patients according to the 2019 WHO’s revised cardiovascular disease risk prediction chart.
The conventional sequences (T1, T2 and FLAIR) on 1.5T MRI were 3D, acquired in sagittal plane, with axial and coronal automatic reconstruction. SWI and DWI were acquired in axial plane. Parameters were the following: T1-3D MPRAGE: TE, 26 ms; TR, 2000 ms; TI, 900 ms; flip angle, 8°; section thickness, 1 mm; in-plane voxel size, 1×1×1mm; 256 matrix; total acquisition time, 4. 30 min; T2-3D SPACE (sagittal sampling perfection with application optimised contrast using different flip-angle evolutions): TE, 381 ms; TR, 3200 ms; flip angle, 120°; slices, 1 mm; in-plane voxel size, 1×1×1mm; total acquisition time, 6 min; T2-3D SPACE FLAIR: TE 335 ms, TR 5000 ms, TI 1800 ms.; flip angle, 120°; section thickness, 1 mm; matrix 256; in-plane voxel size, 1×1×1; total acquisition time, 5.30 min; SWI: TE, 40 ms; TR, 49 ms; flip angle, 15; section thickness, 1.6 mm; matrix 128; acquisition time, 5:50 min; and DWI: TR, 1310 ms; TE, 99 ms; isotropic voxels; b-value 0 and b-value 1000; slices, 2 mm; acquisition time 0.06 s/slice; matrix 128.
The imaging markers were defined by the STandards for ReportIng Vascular changes on nEuroimaging consortium, which unified definitions of CSVD biomarkers based on key neuroimaging characteristics.19 The MRIs were evaluated by an experienced neuroradiologist (ZMH-D) who was blind to clinical and laboratory details.
White matter hyperintensities (WMH) of vascular appearance were defined as hyperintense images in T2 and FLAIR, with absence of cavitation. Evaluation of WMH was performed in axial FLAIR images, WMH were independently evaluated using the semiquantitative Fazekas scale. WMH20 less than 10 mm from the ventricular system were categorised as periventricular. Each transverse slice was reviewed, the coronal and longitudinal slices were also analysed using MPR (multiplanar reconstruction) method of displaying three-dimensional WMH. A modification of Fazekas scale was used to assess the different types of hyperintense signal abnormalities surrounding the ventricles and in the deep white matter. Periventricular hyperintensity (PVH) and separate deep WMH signals (DWMH) were graded as: 0—absence of PVH and DWMH, 1—pencil-thin lining surrounding the lateral ventricles or in a cap around the frontal horns and/or isolated, punctate foci hyperintensities in white matter; 2—PVH in soft halo and/or subcortical hyperintensity foci beginning to confluence; 3—irregular PVH and/or large confluent areas extending to the deep white matter.
Lacunes were identified as cavities with fluid, appearing in FLAIR sequences as hypointense cavities, surrounded by a hyperintense halo, between 3 and 15 mm in diameter. PVS are commonly microscopic, and not visible on conventional neuroimaging, but when enlarged they are identified as small well-defined images (usually smaller than 3 mm in diameter), with a signal intensity equal to the cerebrospinal fluid in T2 sequence. They are most frequently located in basal ganglia, centrum semiovale, and corona radiata, following the orientation of the perforating arteries. Microbleeds were identified as small hypointense lesions (2-5 mm in diameter) in T2*/SWI (susceptibility weighted imaging) sequences.19
Additionally, a global CSVD score, ranging from 0 to 4, according to the presence of vascular lesions (WMH, lacunes, microbleeds, PVS) as defined by Staals et al, was also employed.21 Since the population studied was asymptomatic, and the burden of vascular lesions was expected to be low, the global CSVD score was assigned two categories according to the severity of lesions: 0–1, when none or only one type of WMH or PVS was detected; and 2–4, when combinations of 2–4 vascular lesions were identified. WMH Fazekas 3, lacunes and microbleeds were considered as more severe vascular lesions and classified as 2-4 CSVD score.22
Data analyses
To test associations between variables, χ2 and Student’s t-tests were performed for categorical variables and continuous variables, respectively. A multivariate regression analysis was completed to determine the independent association of CV risk (as measured with the WHO revised chart) and hypertension with the severity of the global CSVD imaging score. Multivariate regression analysis was also applied to evaluate the independent association of risk factors with the severity of brain damage in each of the CV risk groups (LR and M/H). Statistical processing was carried out with the STATISTICA V.10.0 program for Windows and the level of significance was set at p<0.05.
Results
One hundred and seventy patients were included in the study, distributed according to CV risk in two groups: 43 patients in the low-risk group (LR-patients) (25.3%) and 127 patients in the moderate-high-very high-critical risk group (M/HR-patients) (74.7%). Among the M/HR-patients, 57 classified as moderate risk (33.5%), 59 as high risk (34.7%), 9 as very high risk (5.3%) and 2 as critical (1.2%) (figure 2).
M/HR-patients were significantly older than LR-patients, smoked more frequently, and had higher serum triglyceride values. Although the frequency of arterial hypertension did not differ between groups, M/HR-patients displayed significantly higher SBP readings at inclusion. There were no diabetic patients in the LR group (table 1).
Characteristics of demographic, clinical and laboratory variables in the study groups
The MRI findings detailed in table 2 revealed that 51.2% of all subjects presented more severe global CSVD (CSVD scores: 2–4). WMH were the most frequent MRI lesions encountered, being significantly more frequent and severe in the M/HR group. Overall, lacunes and microbleeds were seen in a small group of patients (8.2% and 2.9% respectively), with no significant difference between the two study groups. Enlarged PVS, although frequently detected, were not associated with CV risk. Additionally, it is important to emphasise that 32.6% of low-risk patients presented global CSVD severity 2, with a predominance of WMH and enlarged PVS. Nevertheless, two of them exhibited lacunes and two exhibited WMH Fazekas 3, which are considered more severe vascular lesions.
Characteristics of neuroimaging findings in the study groups
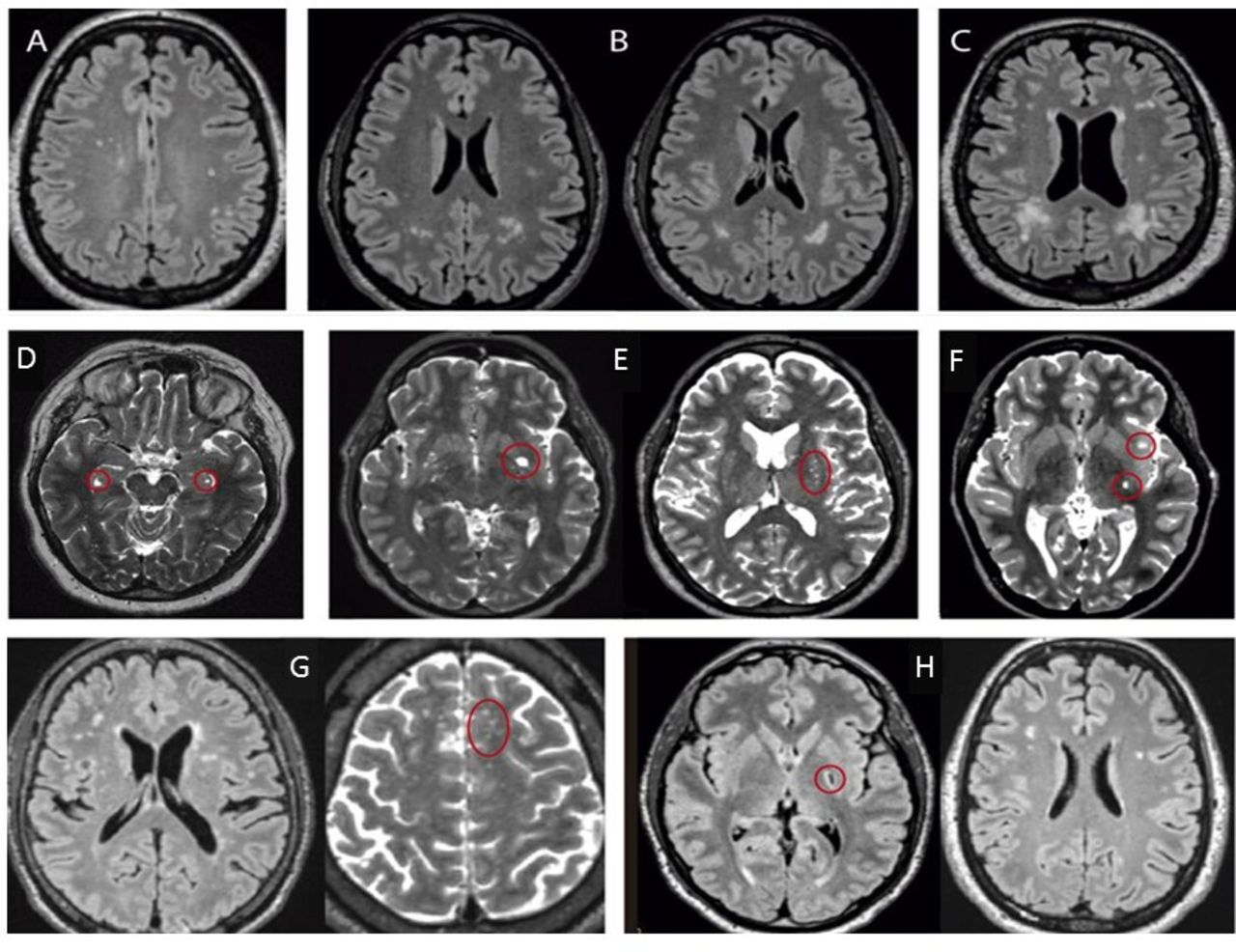
The MRI of three asymptomatic hypertensive patients (aged 35–50 years), with several years of hypertension evolution and low CV risk according to the WHO 2019 revised CV risk chart, showing WMH, PVS and lacunes, are shown in figure 3.

{kind=link}
{kind=link}
{kind=link}
Magnetic resonance images (MRI) show cerebral small vessel disease (CSVD) in low-risk patients (A-H). In A, isolated, punctate foci white matter hyperintensities (WMH) on FLAIR (Fluid Attenuated Inversion Recovery) sequence (Fazekas 1) are seen. Subcortical WMH foci beginning to confluence are shown in B (Fazekas 2) and irregular periventricular hyperintensity areas extending to subcortical white matter in the posterior brain regions (Fazekas 3) in C. Enlarged perivascular spaces (PVS) (red circles) are visualized in T2 sequence, at different locations: hippocampus (D), basal ganglia (E), next to thalamus and insula (F). Images G and H show two patients with CSVD score 2. In G, WMH Fazekas 1 (cap-shaped hyperintensities around the frontal horns and isolated WMH) on FLAIR and PVS (red circle) on T2 are shown. Lacune of ischemic origin on left globus pallidus and WMH Fazekas 1 are seen in FLAIR sequence in H.
A multivariate regression analysis was performed with global CSVD imaging score as the dependent variable, and hypertension and CV risk (classified as LR and M/HR risk) as independent variables. Although both CV risk and hypertension were associated independently with asymptomatic CSVD score, hypertension exerted a greater toll on the severity of brain damage (table 3).
Multiple regression analysis of total CSVD score severity in asymptomatic individuals
Multivariate regression analyses were calculated independently in the LR and M/HR groups, with global CSVD imaging score as the dependent variable. The WHO revised CV risk was substituted with risk factors known to contribute with target organ damage (age, sex, hypertension, diabetes, smoking and blood cholesterol and triglycerides) as independent variables. In LR patients only hypertension was independently associated with the severity of brain damage (multiple R=0.641; F=2.68; p=0.04 (hypertension: p=0.006)); whereas in M/HR patients, it was age and hypertension (multiple R=0.453; F=3.72; p=0.001 (age: p=0.03; hypertension: p=0.000)).
Discussion
This study evidenced a significant number of neurologically healthy individuals recruited from CV risk consultations in primary healthcare areas, displaying cerebral small vessel involvement (51.2%) as expressed through the global CSVD score, as well as an association of the CV risk score with the burden of CSVD. This supports the close-fitting association between CSVD and vascular risk factors which can result in the future occurrence of acute or chronic cerebral complications. The main result was the demonstration of asymptomatic CSVD even in subjects with low CV risk, and the independent association of age and hypertension with this condition.
Previous studies in Cuba had revealed that the proportion of subjects with low CV risk fluctuated between 59% and 86% in asymptomatic adults.23 24 With the revised WHO CV disease risk prediction charts, this proportion will undoubtedly change, considering that the cut-off for low CV risk has been set to <5%, instead of <10% as previously established.15 This study, although not strictly a community study, revealed that the proportion of LR subjects declined to 25% employing the15 revised charts for the calculation of global CV risk. The increase of patients with moderate CV risk alerts us in the need of taking actions in order to reduce the burden of cardio-cerebrovascular disease, with the application of pharmacological and non-pharmacological therapies to control modifiable risk factors and target organ damage. This would subsequently reduce CV morbimortality, which is in accordance with Cuba’s epidemiological reality, where CV disease and stroke are among the first 3 causes of death.13
The prevalence of asymptomatic CSVD detected in this study was similar and even lower when compared with other reported series.25 26 Despite the application of the revised risk prediction charts, it was surprising to perceive that 33% of low-risk patients exhibited imaging signs of CSVD, with more severe lesions indicating a global CSVD severity of 2 (including lacunes and Fazekas 3 for WMH). Therefore, these individuals with a calculated low CV risk, already exhibited considerable brain involvement.
Several studies have evaluated CV risk in individuals with risk factors employing different charts, but none approached the impact on the brain.17 27 Recently Nam et al reported a correlation between CV risk score (employing the model developed by the American College of Cardiology/American Heart Association) and the burden of CSVD in a dose–response manner in a neurologically healthy population28; but no information concerning the prevalence of CSVD in LR patients was available.
A small investigation was recently conducted by us in 39 hypertensive patients, where CV risk was assessed with the PAHO CV risk calculator.23 Although the MRI variables were not evaluated in the same manner, a high frequency of MRI lesions was encountered in patients with low to moderate CV risk, suggesting a limited association of brain parenchymal involvement with the level of CV risk.
A more detailed insight into the specific MRI lesions in CSVD reveals the importance they have at a subclinical stage for individuals with apparently low CV risk.
In the current investigation, the presence of PVS was very frequent in individuals with all levels of CV risk (including LR patients), and considering that more than 75% of them were hypertensive, this would support the effect of hypertension on the glymphatic system, expressed through the demonstration of enlarged PVS.29 Very recently Gao et al also reported the frequent occurrence of PVS in a very large cohort of individuals without neurological involvement.30
More severe WMH (Fazekas 2–3) were encountered in one third of the patients included in this investigation, being significantly more frequent and severe in the M/HR group. It is important to emphasise that these more severe WMH scores were also present in 14% of LR patients. Other studies have reported considerable evidence of asymptomatic CSVD in non-elderly individuals, where WMH were the most frequent lesions, as in our study.31 32 Additionally, the relation of high blood pressure values with WMH lesions and their progression in neurologically asymptomatic subjects has been demonstrated.33 34
Lacunes and microbleeds were present less frequently in this cohort, but percentages were similar to those reported in asymptomatic individuals from population-based studies.3 These lesions represent more severe vascular involvement, and although not significantly associated with the degree of CV risk, their prevalence was slightly higher in patients with more elevated risk. Nevertheless, the occurrence of lacunes in two patients with low CV risk, constitutes a warning sign that cannot be overlooked.
The multivariate analysis conducted in this study revealed an independent association of CV risk prediction and hypertension with the burden of global CSVD. When the CV risk groups were analysed independently, the only risk factor associated with the severity of brain damage was hypertension, even in the low-risk group. This analysis confirmed the importance of hypertension, as a morbid condition, in determining the burden of asymptomatic CSVD.
The revised WHO CV risk charts include SBP measurement, but not the diagnosis of hypertension. An isolated measurement of SBP could mask the long-time effects on the brain of possibly elevated blood pressure peaks during the day or of previous periods with poor blood pressure control. This could explain why some apparently neurologically healthy individuals classify as having a low CV risk, while there is widespread MRI evidence signalling definite brain involvement.
The recent revised charts for the calculation of CV risk, automatically classify subjects with diabetes mellitus as having high CV risk. It should be kept in mind that non-diabetic subjects with neuroimaging signs of CSVD are at a high risk of developing stroke, dementia and depression, in a similar overall ratio than individuals with diabetes.35
If arterial hypertension received the same level of risk as diabetes mellitus in these charts, a patient suffering from hypertension would never classify as low CV risk, notwithstanding if this condition was under control or not.
The HEARTS app is a risk stratification approach oriented most specifically to CV risk, which is particularly suited for primary settings with limited resources, where saving the greatest number of lives at the lowest cost is the priority. Nevertheless, despite its high discriminative capacity, it is not intended to cover the entire context of CV risk.16 When applied seeking for cerebrovascular risk prediction, the results are not so clear; and although more severe asymptomatic brain lesions were associated with middle-high CV risk, a considerable number of individuals classifying as LR, actually exhibited substantial evidence of subclinical CSVD. Thus, for individuals with LR, especially if they suffer from arterial hypertension, screening methods for asymptomatic CSVD at primary settings need to be developed, in order to establish more personalised attention to avoid serious neurological complications.36 37
The main strength of this investigation was that, to the best of our knowledge, it would be the first study to evaluate the association between CV risk and neuroimaging findings of asymptomatic CSVD employing a particular predictive tool (HEARTSapp), and estimating the prevalence of CSVD in low CV risk individuals. However, there were some limitations related with sample inclusion. First, the sample size was relatively small, especially for the LR group, and second, there may be an inclusion bias, due to the fact that the asymptomatic individuals were consecutively included from only three health areas in Havana and not randomly selected.
Conclusions
CV risk stratification through the HEARTS app has limited utility for predicting brain health in individuals with low CV risk. Although more severe subclinical brain lesions were associated with higher CV risk, there are evidences supporting the importance of identifying silent target organ damage to the brain in individuals with apparently low CV risk, especially if they suffer from arterial hypertension.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics Committee and the Scientific Council of the Institute of Neurology and Neurosurgery. ID: 0325-2018. Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors ZMH-D, AG-Q and MP-Z designed data collection tools, monitored data collection for the whole investigation, wrote the statistical analysis plan, cleaned and analysed the data, and drafted and revised the paper. Additionally, they are responsible for the overall content as guarantors. MP-M, MAP and EHH-M conducted the neurological examination of the patients, monitored data collection for the whole investigation, and revised the final version of the manuscript. SG-G and MBM, monitored data collection for the whole investigation, participated in the statistical analysis plan, cleaned and analysed the data, and drafted and revised the final version of the manuscript. ZMH-D also diagnosed and classified the brain MRI, and together with YMA and AAD processed MRI. The latter two researchers also drafted and revised the final version of the manuscript.
Funding This investigation is part of a larger research project for which we received funding from the Cuban Ministry of Health (grant 1801016).
Competing interests No, there are no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.