Article Text

Abstract
Introduction Shortening the time from stroke onset to treatment increases the effectiveness of endovascular stroke therapies.
Aim This study aimed to predict the modified Rankin Scale score at 90 days post-stroke (mRS-90d score) in patients with acute ischaemic stroke (AIS) with respect to four types of treatment: conservative therapy (CVT), intravenous thrombolysis only (IVT), mechanical thrombectomy only (MT) and pretreatment with IVT before MT (IVT+MT).
Patients and methods This nationwide observational study included 124 484 confirmed cases of acute stroke in Sweden over 6 years (2012–2017). The associations between onset-to-treatment time (OTT), patient age and hospital admission National Institutes of Health Stroke Scale (NIHSS) score with the five-levelled mRS-90d score were retrospectively studied. A generalised linear model (GLM) was fitted to predict the mRS-90d scores for each patient group.
Results The fitted GLM for CVT patients is a function of age and NIHSS score. For IVT, MT and IVT+MT patients, GLMs additionally employed OTT variables. By reducing the mean OTTs by 15 min, the number needed-to-treat (NNT) for one patient to make a favourable one-step shift in the mRS was 30 for IVT, 48 for MT and 21 for IVT+MT.
Discussion and conclusion This study demonstrates linear associations of mRS-90d score with OTT for IVT, MT and IVT+MT, and shows in absolute effects measures that OTT reductions for IVT and/or MT produces substantial health gains for patients with AIS. Even moderate OTT reductions led to sharp drops in the NNT.
- statistics
- stroke
- interventional
- MRS
Data availability statement
Data are available upon reasonable request. Aggregate data supporting the findings of this study are available upon request from a qualified investigator.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The comparative effectiveness of intravenous thrombolysis (IVT) and/or mechanical thrombectomy (MT) on clinical outcomes in patients with acute ischaemic stroke has been well studied, and the association between time delays to treatment start with declining likelihood of favourable functional outcomes has been derived from comparative analyses across different treatment modalities. Modelling of clinical outcomes would preferably delineate these associations in absolute effect measurements for respective types of treatment, to help guide reconfigurations of acute stroke services more precisely.
WHAT THIS STUDY ADDS
This study demonstrated linear associations between modified Rankin Scale score at 90 days post-stroke (mRS-90d score) and symptom onset to treatment time for IVT, MT and IVT+MT. It provides models for predicting the mRS-90d score in individual patients based on age, hospital admission National Institutes of Health Stroke Scale score and time from symptom onset to treatment initiation with IVT and/or MT. Predictive models enable the calculation of trade-off effects between time delays to treatment with IVT and MT.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study makes it possible to model clinical outcomes for the reconfiguration of acute stroke services with respect to specific patient population characteristics and the level of accessibility to IVT-ready hospitals and comprehensive stroke centres. The expected health gain from reducing the time from symptom onset to treatment initiation seems to be substantially greater for patients treated with IVT prior to MT than for patients treated with MT alone. This finding requires further confirmation in future studies.
Introduction
Shortened onset-to-treatment time (OTT) for intravenous thrombolysis (IVT) leads to reduced mortality, fewer cases of symptomatic intracranial haemorrhage (sICH) and improved functional outcomes at hospital discharge in patients with acute ischaemic stroke (AIS).1 The comparative benefit of complementary treatment with mechanical thrombectomy (MT) on functional outcomes at 3 months post-stroke in patients with AIS caused by anterior circulation large vessel occlusion (LVO) also displays associations with OTTs.2 The established connections between OTTs and patient outcomes have spurred the development of emergency medical services (EMS) transportation systems, stroke healthcare infrastructure and prehospital triage protocols to improve the delivery of acute stroke care with IVT only, MT only or IVT plus MT (IVT+MT) to treat eligible patients with AIS.3–5 Still, ineligibility due to time delays exceeding 4½ hours from stroke onset to hospital admission accounts for one-third of all patients with AIS who do not receive IVT in Sweden.
The proportion of patients with AIS undergoing treatment with either MT alone or IVT+MT varied substantially among Swedish healthcare regions.6 Inadequate access to and underused delivery of acute stroke treatment prevails globally.7–10 Modelling the impact of patient age, the National Institutes of Health Stroke Scale (NIHSS) score at hospital admission and OTTs on patient outcomes following treatment with IVT only, MT only, IVT+MT or conservative therapy (CVT), defined as treatment with neither IVT nor MT, may help guide ongoing optimisation and improvement efforts in acute stroke care management.11–14 This study aimed to fit regression models for predicting the modified Rankin Scale score at 90 days from stroke onset (mRS-90d score) in patients with AIS, with respect to the type of acute stroke treatment: CVT, IVT only, MT only and IVT+MT.
Methods
This nationwide retrospective observational study included all patients with a confirmed AIS diagnosis in Sweden from 2012 to 2017.
Data sources
The personal identification number assigned to every nationally registered individual in Sweden enables linking of patient data across registers. The National Board of Health and Welfare handled the initial consolidation and anonymisation of data from registries; it administers the Cause of Death Register that contains all underlying causes of death coded with the International Classification of Diseases, 10th Revision (ICD-10) in Sweden since 1997,15 and the National Patient Register that keeps records of all inpatient care in Sweden since 1987, including diagnosis at hospital discharge encoded with the Swedish modification of three-levelled ICD-10 (ICD-10-SE).16 All hospitals in Sweden that admit patients with acute stroke report to the Swedish stroke healthcare register (Riksstroke), which covers approximately 89% of all stroke-related medical care events in Sweden annually.17 The two operative actors (SOS Alarm and Sjukvårdens larmcentral) jointly keep all the emergency call operator data in Sweden, comprising medically indexed call-out data of EMS.
Study population
Based on the ICD-10-SE encodings for acute stroke diagnosis in Riksstroke, all 124 484 confirmed cases of acute stroke in Sweden from 2012 to 2017 remained in its register after the merger with linked acute stroke data from the Cause of Death Register and the National Patient Register. Subsequent linking to EMS call-out data on cases of suspected stroke in the emergency call operator records yielded 72 640 confirmed cases of acute stroke with matching EMS call-out records. The dismissal of all cases of AIS with reported posterior circulation LVO followed the exclusion of all cases of acute stroke with diagnostic codes other than cerebral infarction (I63). Hence, the study population for analysis consisted of all cases of cerebral infarction, with anterior circulation LVO or without occlusion site reporting, classified into four patient groups according to the type of treatment (figure 1).

Study population classified into four patient groups for analysis. IV, intravenous.
Descriptive statistics
Descriptive statistics of the study population and for each of the four patient groups included baseline patient variables and admission and treatment variables. The calculated mean values are presented with the corresponding SD; median values are complemented by the IQR, the 5th and 95th percentiles and the absolute number of cases underlying calculus; and proportions are displayed as percentages in conjunction with absolute numbers of cases. Patient baseline characteristics included age, sex, wake-up symptoms of stroke and recurrent stroke, with the latter three in the form of binary variables (man/woman or yes/no). In addition to the NIHSS score for assessment of stroke symptom severity on a scale ranging from 0 (minimum symptom severity) to 42 (maximum symptom severity), the set of patient characteristics assessed at hospital admission also included the modified Reaction Level Scale for assessment of patients’ consciousness level on a three-level assessment scale ranging from 1 to 3 (1=alert, 2=drowsy, 3=unconscious). Two binary variables—interhospital transfer and thrombolysis alert—also constituted hospital admission characteristics. The thrombolysis alert variable denotes whether the emergency call operator activates a specially designated pathway through the prehospital and hospital admission phases for patients with suspected stroke, bound directly for treatment with IVT.18 The time variables included for analysis are the estimated time lapses (in minutes) from stroke onset to hospital admission and stroke unit admission. The OTTs for treatment with IVT and MT were measured in minutes and presented as median times. The proportion of patients with sICH following treatment with IVT only, MT only or IVT+MT has also been reported.
Clinical outcomes
The primary clinical outcome was the translated version of the mRS-90d, which employs an algorithm for attainment of mRS-90d scores.19 It is based on self-reported functional outcomes in the Riksstroke register at the 3-month follow-up assessment of activities of daily living (ADL) for patients who are post-stroke with regards to level of dependency, mobility, dressing and toileting and type of housing. The ordinary mRS ranges from perfect health (mRS 0) to death (mRS 6), with denotations of increasing functional disability level in-between. The translated version fuses the three lowest mRS scores commonly associated with functional independence (mRS 0, 1 and 2) into a single score (mRS 0–2), while the interpretation of the remaining mRS scores (mRS 3, 4, 5 and 6) remains unaltered. Consequently, the translated version of the mRS in this study employs a five-level scoring scale ranging from functional independence (mRS 0–2) to death (mRS 6), hereafter denoted simply as mRS-90d.
Estimations of the number of patients needed-to-treat (NNT) for an aggregated, favourable one-step shift on the mRS-90d scale were obtained by inverting the prediction modelled shifts in the mean mRS-90d scores resulting from hypothetical reductions in the mean OTT in the IVT only, MT only and IVT+MT patient groups.
Predictive modelling—variable selection and goodness of fit
With the conditional probability limit for type I error set to 5% (α=0.05), all variables were tested for the statistical significance of individual parameters. Assessment of all subset combinations in the variable selection process included the examination of all possible two-way interactions. Insertion of dispersion parameter adjustments was used when appropriate. During model development, the primary outcome was treated as an interval-type variable. The selected modelling variables underwent further assessment of the numerical variable transformations. The model selection process employed regression analysis with the aim of providing the best fit for model prediction of the primary clinical outcome (mRS-90d) for each of the four patient groups, striving for as few independent modelling variables as possible without incursion of substantial loss in prediction accuracy. In comparisons of models with the same set of modelling variables, the root mean square error is applied as a selection criterion; otherwise, the Akaike information criteria guide model selection. Calculation of additional goodness-of-fit measurements to complement assessments of model performance in fitted generalised linear models (GLMs) includes the coefficient of determination (R2) for GLMs without intercept and the mean arctangent absolute percentage error.20 21
All statistical analysis and modelling are produced by the utilisation of software tasks in SAS Enterprise Guide V.6.1, SAS Enterprise Miner Workstation V.13.1. Specifically, the high-performance data mining environment in SAS Enterprise Miner facilitates model development and comparisons.
Results
The four patient groups for analysis consisted of 63 964 cases of cerebral infarction (I63), with anterior circulation LVO or without occlusion site reporting. CVT was chosen in 54 424 cases, while IVT was reported in 8405 cases. Treatment with MT alone was reported in 558 cases, while IVT+MT accounted for another 577 cases (figure 1).
The CVT patient group contained the most patients, displayed the highest mean age (77.5 years) and had the lowest median NIHSS score (3) across the four patient groups at hospital admission. Conversely, the lowest mean age (71.7 years) and the highest median NIHSS score (14) were found in the IVT+MT patient group.
As many as 97.3% and 98.6% of cases in the IVT only and IVT+MT patient groups, respectively, were admitted to the hospital via the thrombolysis alert pathway compared with 86.3% of cases in the MT only patient group. The MT only and IVT+MT groups displayed interhospital transfers in 24.5% and 21.1% of cases, respectively.
Both the mean and median OTT for IVT in the IVT+MT patient group were 23 min shorter than those in the IVT only patient group (table 1). In comparison to MT only patients, the mean OTT to MT was 41 min shorter in IVT+MT patients. In contrast, the median OTT to MT was 10 min longer for IVT+MT patients than for MT only patients (table 1).
Patient baseline, admission and OTT variables
The highest proportion of patients with sICH following acute stroke treatment was reported in the IVT+MT patient group (4.2%), followed by the IVT only patient group (2.8%) and the MT only patient group (0.9%).
mRS-90d
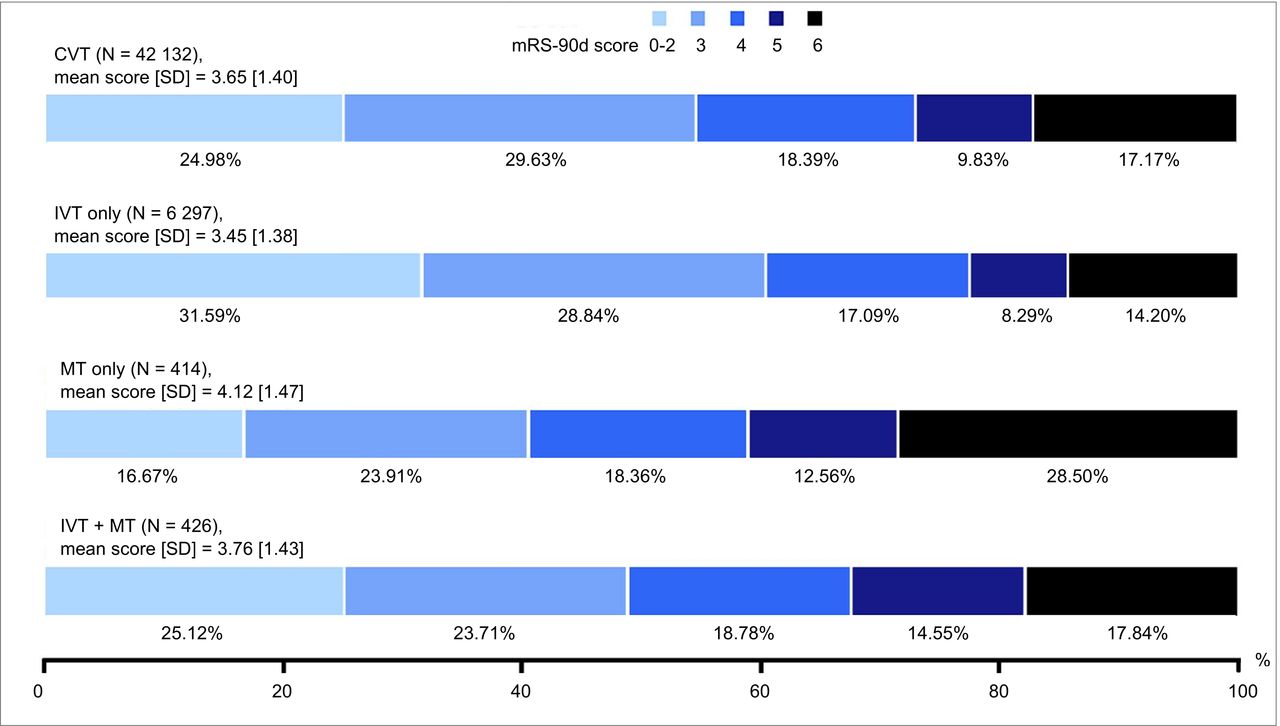
The mRS-90d score distributions varied among the four patient groups, as shown in figure 2. The highest level of functional independence (31.6%) and lowest mortality (14.2%) were observed in the IVT only patient group. In contrast, the MT only patient group displayed the lowest proportion of patients with functional independence (16.7%) and the highest mortality (28.5%).
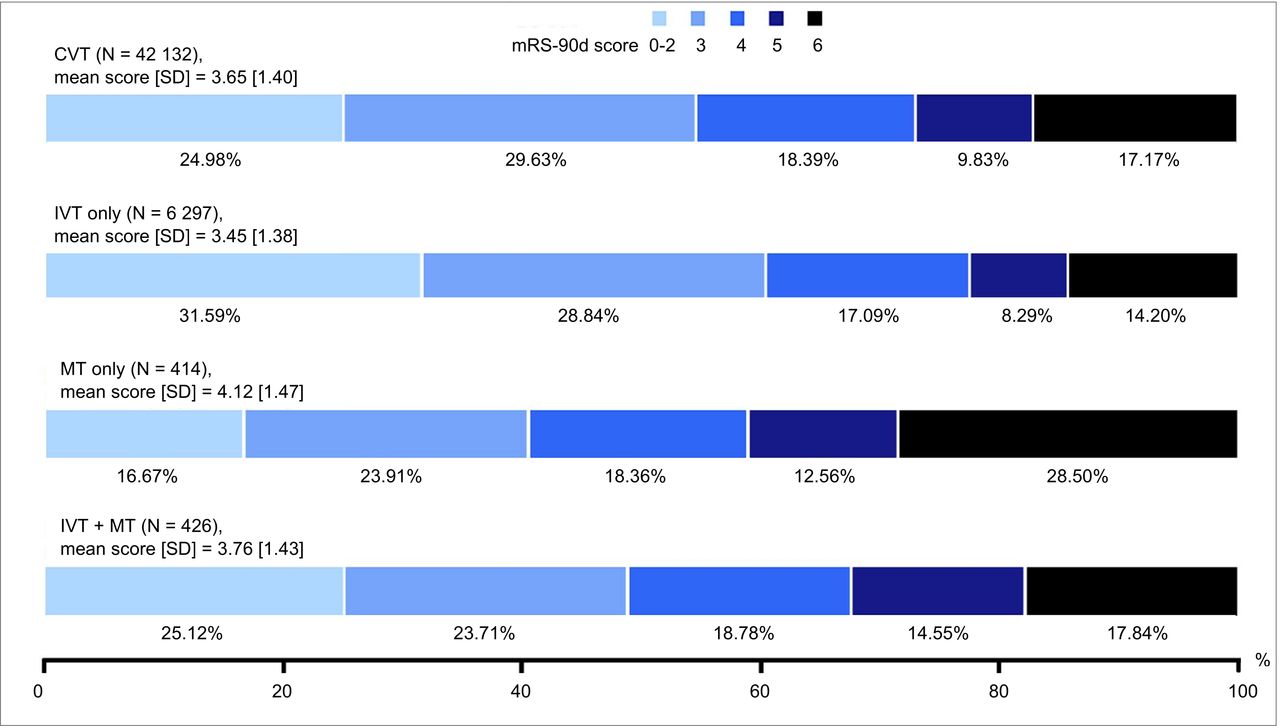
mRS-90d score distribution (%), mean score (SD) and number of cases (N) in respective patient group. CVT, conservative therapy; IVT, intravenous thrombolysis; mRS-90d, modified Rankin Scale score at 90 days post-stroke; MT, mechanical thrombectomy.
Fitted prediction models
The maximum likelihood parameter estimates of the selected GLMs were fitted under the assumption of a normal distribution with an identity link function and dispersion parameter adjustments. Two-way interactions failed to improve the overall model performance.
The fitted GLM for the prediction of mRS-90d scores in patients treated with CVT exploits the age and NIHSS score variables. For each additional year of age (all else being equal), the GLM proposed an upward shift equal to 0.0388 steps on the mRS-90d scale. The impact of hospital admission NIHSS score was even greater. With a proposed parameter estimate of 0.0960, a 10-point shift in the NIHSS score (all else being equal) is sufficient to accomplish a one-step shift on the mRS.
While the explanatory power of age and hospital admission NIHSS remained important for predicting mRS-90d scores, the predictive GLMs for the other three patient groups emphasised the time-critical aspects of treatment efficiency. The exponentiation of age and NIHSS variables in these GLMs highlights the OTT-dependent treatment effects of IVT and MT on the mRS-90d score. The impact of age on patient outcomes was the greatest in the MT only group. The highest sensitivity to the NIHSS score distinguished the fitted GLM of the IVT only patient group (table 2).
GLMs for predicting the mRS score at 90 days in patients with AIS according to type of acute stroke treatment
The proportion of patient observations employed in the prediction modelling differed among the patient groups. The selected patient observations displayed a higher average age than the entire patient group’s mean age for each of the four patient groups, whereas the median hospital admission NIHSS score, OTT to IVT, OTT to MT and mean mRS-90d scores were identical or differed only slightly in this respect (table 2).
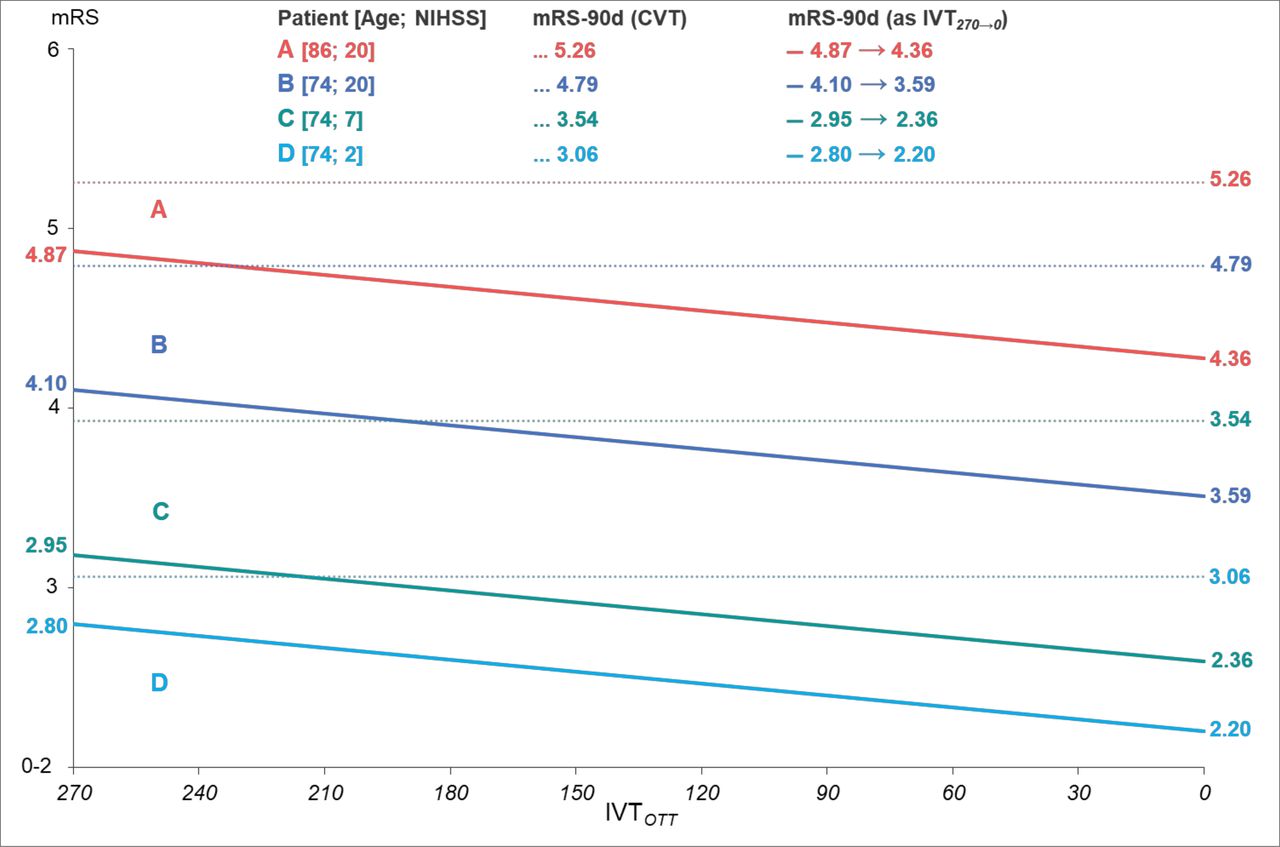
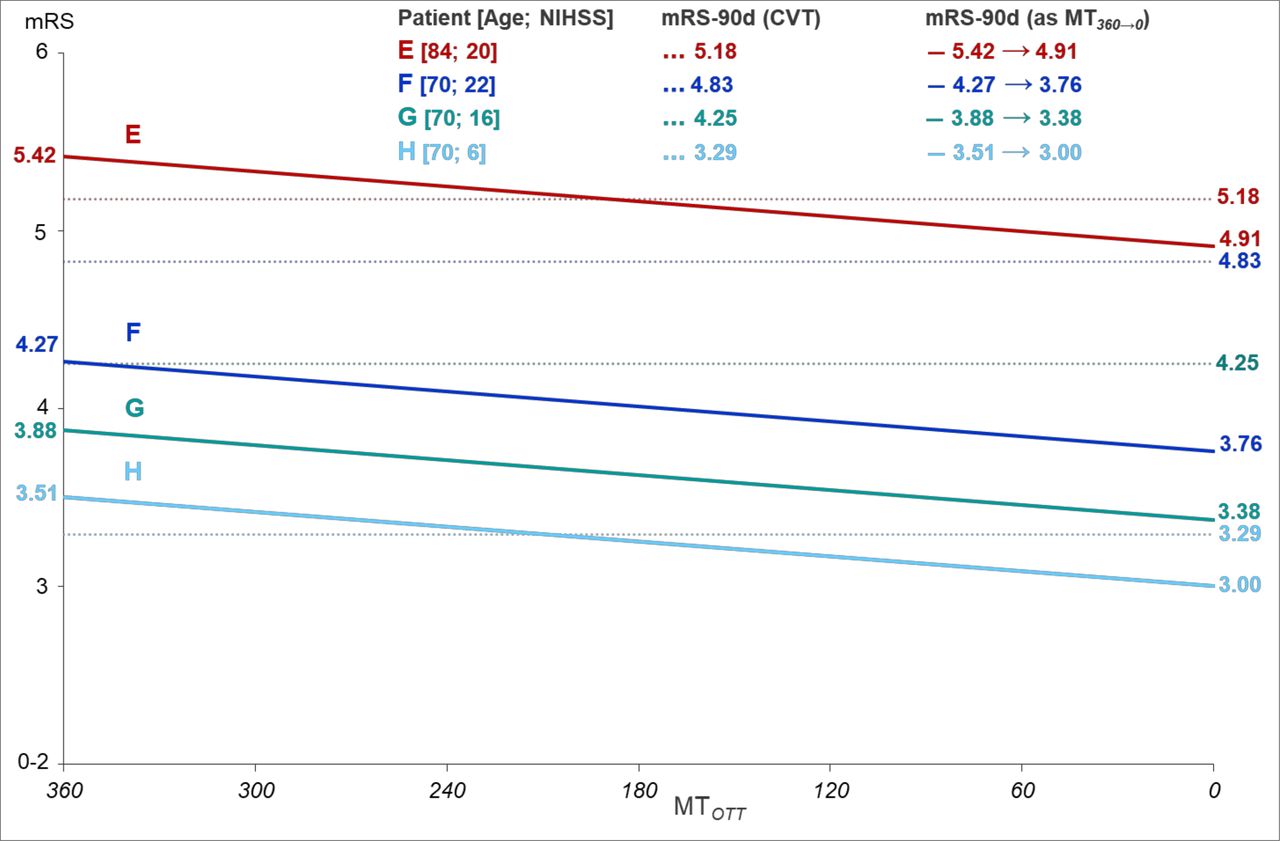
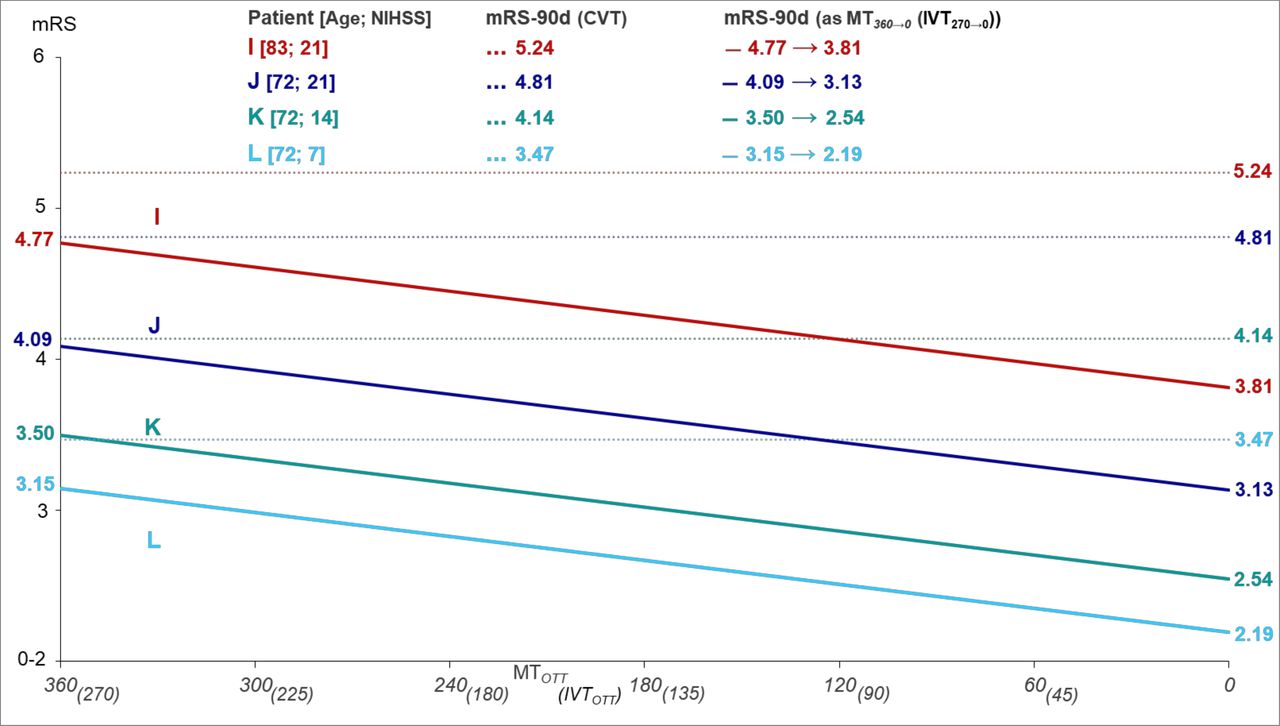
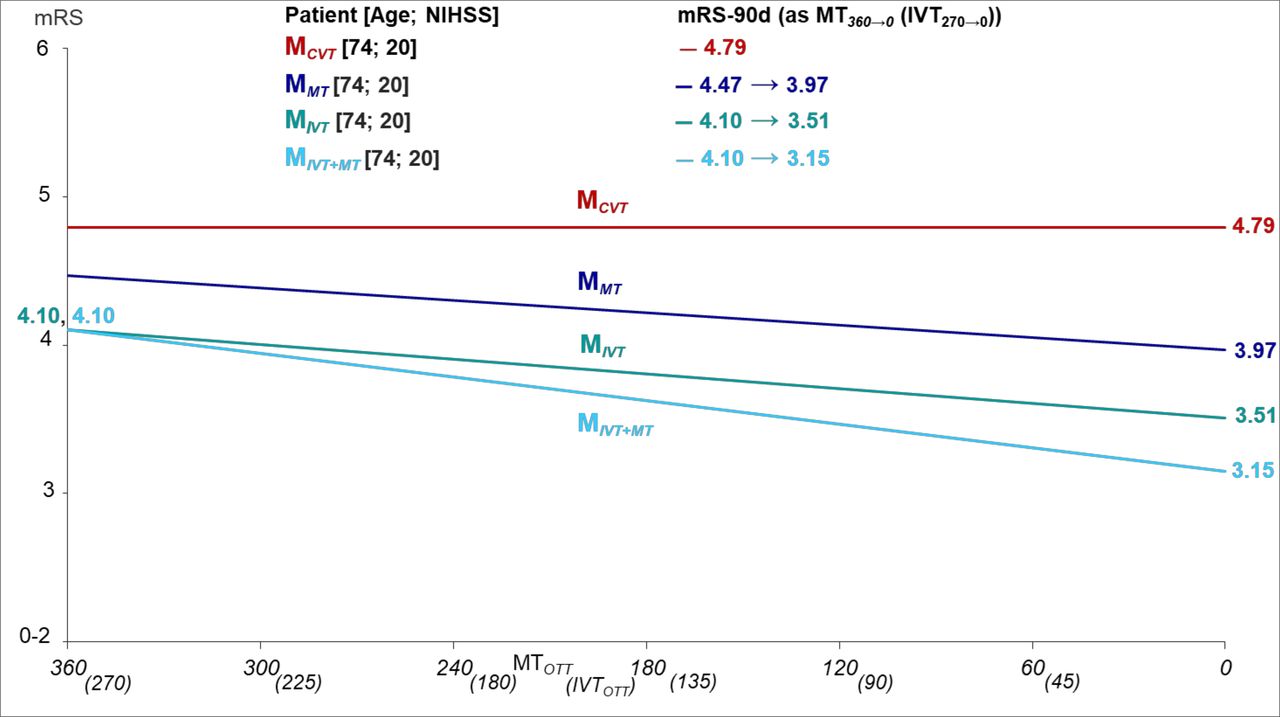
To elucidate the association between OTT and the mRS-90d score, as reflected in the fitted GLMs, predicted mRS-90d scores in patients of different ages and hospital admission NIHSS scores following treatment with IVT (figure 3), MT (figure 4) and IVT+MT (figure 5) were delineated graphically over current OTT windows, and juxtaposed to alternative treatment with CVT. Furthermore, the example case of a single patient juxtaposes the predicted mRS-90d scores following treatment with each of the four types of acute stroke treatments (figure 6).

Example cases (A, B, C and D) of prediction modelled mRS-90d scores in patients treated with IVT only, based on age, NIHSS and OTTIVT. CVT, conservative therapy; IVT, intravenous thrombolysis; mRS-90-d, modified Rankin Scale score at 90 days post-stroke; NIHSS, National Institutes of Health Stroke Scale; OTT, onset-to-treatment time.

Example cases (E, F, G and H) of prediction modelled mRS-90d scores in patients treated with MT only, based on age, NIHSS and OTTMT. IVT, intravenous thrombolysis; mRS-90-d, modified Rankin Scale score at 90 days post-stroke; MT, mechanical thrombectomy; NIHSS, National Institutes of Health Stroke Scale; OTT, onset-to-treatment time.

Example cases (I, J, K and L) of prediction modelled mRS-90d scores in patients treated with IVT+MT, based on age, NIHSS, OTTIVT and OTTMT. CVT, conservative therapy; IVT, intravenous thrombolysis; mRS-90-d, modified Rankin Scale score at 90 days post-stroke; MT, mechanical thrombectomy; NIHSS, National Institutes of Health Stroke Scale; OTT, onset-to-treatment time.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Example cases (MCVT, MMT, MIVT and MIVT+MT) of the prediction modelled mRS-90d score in patient M given type of acute stroke treatment and based on age, NIHSS and OTTIVT and/or OTTMT where applicable. CVT, conservative therapy; IVT, intravenous thrombolysis; mRS-90-d, modified Rankin Scale score at 90 days post-stroke; MT, mechanical thrombectomy; NIHSS, National Institutes of Health Stroke Scale; OTT, onset-to-treatment time.
Number needed to treat
If the mean OTT for IVT decreases by 15 min, the estimated NNT for an aggregated one-step shift on the mRS-90d scale is 30 for IVT only patients. The corresponding NNT estimates for the MT only and IVT+MT patient groups are 48 and 21, respectively, following 15 min reduction in mean OTT.
Discussion
OTT has a major impact on the effectiveness of treatment with IVT only, MT only and IVT+MT in patients with AIS. Analysis of patient outcomes from OTT reductions commonly features estimations of mRS-90d scores based on relative effect measurements. The development of predictive models for estimating patient outcomes for different types of acute stroke treatment, regardless of the comparable effectiveness of alternative treatments, could help guide further adaptation of acute stroke care management for specific types of treatment and improve functional outcomes in patients with AIS.
To fit the predictive models to each of the four types of acute stroke treatment in this study, it was necessary to acquire appropriate types and quantities of patient observations for analysis. This was achieved by matching patient registry data from the National Board of Health and Welfare and Riksstroke with data records from two emergency call operators in Sweden. The aim was to set out prediction models with the simplest possible expression with regression analysis, and without incursion of prediction accuracy loss in comparison to neural network models and simple decision trees designed with machine learning. This study demonstrated linear associations between the mRS-90d score and OTT to IVT only, MT only and IVT+MT. The predictive models estimated the impact of OTT reductions on mRS-90d scores in patients with AIS using absolute effects measures. The results are in analogy with the incorporated evidence in the current guidelines for acute stroke care management and further strengthen the established associations of OTT with IVT and MT from previous studies.22–25
The predictive GLMs reinforced the baseline NIHSS score as the most important predictor variable of mRS-90d scores in patients with AIS in all four patient groups.26 Thus, despite the higher mean age, the comparatively low median hospital admission NIHSS scores of the CVT and IVT only patient groups accounted for the lower mean mRS-90d scores of these two patient groups compared with the MT only and IVT+MT patient groups.
For patients treated with IVT+MT, the expected downward shift on the mRS-90d following OTT reductions was substantially larger than that for patients treated with MT only, a finding that requires corroboration in future studies. The proportion of patients with reported incidence of sICH in the MT only patient group was surprisingly low, while being just slightly low in the IVT+MT patient group, in comparison to reported sICH rates in patients treated with MT only or IVT+MT in recent studies.27 This study observed a lower sICH rate in the MT only patient group than in IVT+MT patient group, in accordance with Bigdata Observatory platform for Stroke of China-based registry study findings.28
In comparison with pooled patient-level data from five trials in the Highly Effective Reperfusion Using Multiple Endovascular Devices (HERMES) collaboration, the mRS-90d score distribution of MT-treated patients in this study differed notably.29 Among the MT-treated patients in this study (ie, MT only and IVT+MT patients), the reported proportion of patients with functional independence (mRS 0–2) at 90 days post-stroke was 21% compared with 46% in HERMES. The higher median age of MT-treated patients in this study (72 vs 68 years), with a more than doubled median OTT to IVT (201 vs 100 min), may be ascribed to partial explanations for the disparity in mRS-90d score distributions. Certainly, further explanation may be attributable to the sizeable difference between the reported median OTT to MT of 373 min in this study and the reported median time from stroke onset to reperfusion of 285 min for MT patients in HERMES. Furthermore, this study included observations of patients treated with MT that predated the roll-out of second-generation MT devices in clinical practice. Thus, the use of suboptimal MT devices in combination with the limited interventional experience at comprehensive stroke centres during the early years of the study period may also account for some of the differences in the mRS-90d score distribution of MT patients in this study compared with HERMES.
The potential influence of unidentified confounding factors adhering to observational studies limits the certainty of the evidence. The proportion of missing data across patient groups, as shown in table 2, entails a risk of bias in the data, which may impede the internal validity of the results. Thus, despite displaying conformity with previous literature on the connections between OTT and functional outcomes in patients with AIS, the presence of unknown context-specific confounders that decimate the internal validity of predictive GLMs cannot be ruled out. Fitting the GLMs with as few independent and commonly accessible variables as possible simplifies the modelling framework’s transferability beyond the scope of this study, insofar as the specific parameter estimates of the independent variables in the presented GLMs reflect the unique age, NIHSS score and OTT distributions of the Swedish stroke population.
The algorithm employed in this study for calculating mRS-90d scores based on patients who had a stroke’s self-reported levels of ADL concatenates the mRS-scores 0, 1 and 2 into mRS-score 0–2. Thus, the fitted GLMs predicted patients who had a stroke’s mRS-90d scores on a 5-level scale. How the predictive GLMs would perform on the 7-levelled scale and whether such GLM fittings would alter the established linearised associations between mRS-90d scores and OTT for IVT and MT in this study, remains unanswered.
Optimisation problems can be stated to help find potential solutions for both strategic and tactical decision problems in systems of care for acute stroke, such as location-allocation problems concerned with the optimal placement of comprehensive stroke centres and the allocation of EMS vehicles. The demonstrated feasibility of fitting GLMs that predict the mRS-90d scores in patients with AIS by estimating the impact of patient age, hospital admission NIHSS and OTTs on IVT and MT in absolute effect measures enables system optimisation of acute stroke care with respect to patient outcomes.30
The results suggest that even modest time reductions during the prehospital and in-hospital phases of acute stroke care elevate the treatment effectiveness of IVT and MT and subsequently carry substantial health gains for patients with AIS. Moreover, mean OTT reductions may also increase the proportion of patients eligible for acute stroke treatment with IVT only, MT only or IVT+MT.
Data availability statement
Data are available upon reasonable request. Aggregate data supporting the findings of this study are available upon request from a qualified investigator.
Ethics statements
Patient consent for publication
Ethics approval
This study conformed to the ethical principles set in the 1964 Declaration of Helsinki for medical research involving identifiable human materials and data. Data were obtained with ethical approval (Dnr 2017/487–31 and Dnr 2019–00721) from the Swedish Ethical Review Authority.
Acknowledgments
We are grateful to the Swedish National Board of Health and Welfare, Riksstroke, Sjukvårdens larmcentral and SOS Alarm Sverige AB for helping with the data retrieval.
References
Footnotes
Contributors NEV: Study conceptualisation and design, data acquisition, analysis and interpretation, drafting and writing of the manuscript, and guarantor for the overall content. TT: Study conceptualisation and design, revision of the manuscript for intellectual content. PW: Study conceptualisation and design, revision of the manuscript for intellectual content. JL: Revising the manuscript for intellectual content. L-ÅL: Study conceptualisation and design, revision of the manuscript for intellectual content and study supervision.
Funding This study was supported by the Center for Advanced Research in Emergency Response (CARER) at Linköping University, Sweden, and Region Östergötland, Sweden.
Competing interests NEV reports academic grants from Linköping University, and has had research contract with Bayer. TT reports academic grants from University of Gothenburg, Sahlgrenska University Hospital, Sigrid Juselius Foundation and Wennerström Foundation. He has/has had research contracts with Bayer, Boehringer Ingelheim, Bristol Myers Squibb and Portola Pharm. He has/has had advisory board memberships with Bayer, Boehringer Ingelheim, Bristol Myers Squibb and Portola Pharm. TT has filed two international patents: new therapeutic uses (method to prevent brain oedema and reperfusion injury), and thrombolytic compositions (method to prevent post-thrombolytic haemorrhage formation). PW reports academic grants from University of Umeå and the Swedish Heart and Lung foundation. He has/has had research contracts with Abbott and Bristol Myers Squibb. JL reports no conflict of interest. L-ÅL has/has had research contracts with Bayer, Boehringer Ingelheim, AstraZeneca and Janssen. He has/has had attained advisory boards with Bayer, Boehringer Ingelheim, Pfizer, BMS, MSD and GSK.
Provenance and peer review Not commissioned; externally peer reviewed.